
|
Last year – two years after actor Robin Williams died – his wife Susan Schneider Williams wrote an essay entitled The terrorist inside my husband’s head, published in the journal Neurology. It is a heartfelt/heartbreaking insight into the actor’s final years. It also highlights the plight of many who are diagnosed with Parkinson’s disease, but experience an array of additional symptoms that leave them feeling that something else is actually wrong. Today’s post is all about Dementia with Lewy bodies (or DLB). In particular, we will review the latest refinements and recommendations of the Dementia with Lewy Bodies Consortium, regarding the clinical and pathologic diagnosis of DLB. |

Robin Williams. Source: Quotesgram
On the 28th May of 2014, the actor Robin Williams was diagnosed with Parkinson’s disease.
At the time, he had a slight tremor in his left hand, a slow shuffling gait and mask-like face – some of the classical features of Parkinson’s disease.
According to his wife, the diagnosis gave the symptoms Robin had been experiencing a name. And this brought her a sense of relief and comfort. Now they could do something about the problem. Better to know what you are dealing with rather than be left unsure and asking questions.
But Mr Williams sensed that something else was wrong, and he was left unsure and asking questions. While filming the movie Night at the Museum 3, Williams experienced panic attacks and regularly forgot his lines. He kept asking the doctors “Do I have Alzheimer’s? Dementia? Am I schizophrenic?”
Williams took his own life on the 11th August 2014, and the world mourned the tragic loss of a uniquely talented performer.

Source: WSJ
When the autopsy report came back from the coroner, however, it indicated that the actor had been misdiagnosed.
He didn’t have Parkinson’s disease.
What he actually had was Dementia with Lewy bodies (or DLB).
What is Dementia with Lewy bodies?
Dementia with Lewy bodies (or DLB; also known as Lewy body dementia), is the second most common type of progressive dementia, after Alzheimer’s disease. It generally begins after the age of 50, and affects about 0.1% of those over 65 years of age. As with Parkinson’s disease, males appear to be more commonly affected than females.
Dementia with Lewy bodies causes a progressive decline in mental abilities. Yes, memory is impaired, but typically not as much as one sees with Alzheimer’s disease. Judgment, on the other hand, is usually affected early on in the condition and people with Dementia with Lewy bodies also have sleep disturbances (for example, physically acting out of dreams while one is sleeping), visual hallucinations (most commonly people or animals that are not there), and fluctuations in their levels of alertness and attention.

Issues with attention. Source: Incareofdad
But it is the external features of Dementia with Lewy bodies that often cause it to be misdiagnosed as Parkinson’s disease. People with Dementia with Lewy bodies often present Parkinson’s disease-like symptoms such as rigid muscles, slow movement and tremors.
What causes Dementia with Lewy bodies?
We do not know.
While 10-20% of Parkinson’s disease is associated with tiny alterations in one’s DNA (genetic variations), there appears to be less of a genetic component to Dementia with Lewy bodies. Most cases appear to be sporadic.
When researchers look in the brains of people who passed away with Dementia with Lewy bodies, they will quite often find many of the characteristic pathological features of both Parkinson’s disease and Alzheimer’s disease. As the name suggests, Lewy bodies are very present in the brains of people with Dementia with Lewy bodies. These are the circular deposits of alpha synuclein protein inside cells that classical define the Parkinsonian brain.

Before we review the recommendations, I though it may be of interest to describe the process behind the effort.
The Dementia with Lewy Bodies (DLB) Consortium last outlined their recommendations on the diagnosis and management of Dementia with Lewy bodies way back in December 2005 (Click here to read more about that report). So it was about time for an update.
These updates take time, however, and involve a lengthy process which can be broken down into four stages that are focused around a large conference:
- Pre-conference inquiries
- Preconference working groups
- Conference
- Post-conference activities
The pre-conference inquiries began in February of 2014 when a group of international experts met at Cold Spring Harbor in New York. Based on the North Shore of Long Island, the Cold Spring Harbor laboratories is a is a private, non-profit research institution. Established in the 1890, it has also been a centre of biology education for a very long time, and is regularly used by the research community as a venue for conferences.
Impressive fact about Cold Spring Harbor: It has been home to eight researchers who have been awarded the Nobel Prize in Physiology or Medicine.

Cold Spring Harbor. Source: Wikimedia
The point of the pre-conference meeting was to review the current status of knowledge about Dementia with Lewy bodies and to begin developing an agenda for the larger consortium meeting. Another important part of the pre-conference meeting was the establishing of four pre-conference working groups which were established to review the current recommendations and to:
- Identify elements in need of amendment, and those not needing to be changed
- Suggest new topics for potential inclusion
- Identify any anticipated future developments.
The groups prioritised lists of topics for consideration at the larger consortium event. These topics were placed under the general headings:
- Clinical diagnosis
- Clinical management and trial design
- Pathology, genetics, biomarkers and basic science
- Global harmonization
The conference itself was held from the 1st – 4th December 2015 in Fort Lauderdale (Florida) and it was attended by over 390 clinicians, scientists, patients and care partners (Click here to see the abstracts of the meeting). At the meeting, efforts were made to determine consensus for each of the items that had been highlighted for the future recommendations.

International Dementia with Lewy Bodies Conference. Source: LBDA
After the conference, preparations for the final recommendations report were initiated. A first draft was circulated to all participating authors on August 3rd 2016 for review and a revised version circulated for final approval on September 8th 2016. That final report was then submitted and it is the report that was published recently in the journal Neurology:

Title: Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium.
Authors: McKeith IG, Boeve BF, Dickson DW, Halliday G, Taylor JP, Weintraub D, Aarsland D, Galvin J, Attems J, Ballard CG, Bayston A, Beach TG, Blanc F, Bohnen N, Bonanni L, Bras J, Brundin P, Burn D, Chen-Plotkin A, Duda JE, El-Agnaf O, Feldman H, Ferman TJ, Ffytche D, Fujishiro H, Galasko D, Goldman JG, Gomperts SN, Graff-Radford NR, Honig LS, Iranzo A, Kantarci K, Kaufer D, Kukull W, Lee VMY, Leverenz JB, Lewis S, Lippa C, Lunde A, Masellis M, Masliah E, McLean P, Mollenhauer B, Montine TJ, Moreno E, Mori E, Murray M, O’Brien JT, Orimo S, Postuma RB, Ramaswamy S, Ross OA, Salmon DP, Singleton A, Taylor A, Thomas A, Tiraboschi P, Toledo JB, Trojanowski JQ, Tsuang D, Walker Z, Yamada M, Kosaka K.
Journal: Neurology. 2017 Jul 4;89(1):88-100.
PMID: 28592453 (This article is OPEN ACCESS if you would like to read it)
Wow. What a long process!
Indeed. But to be fair, thousands (literally) of people were involved in the process, and one or two of them probably had opinions that may not have fit so well with what some of the other people involved in the process may have been thinking about a particular aspect of Dementia with Lewy bodies.
Such matters take time.
So what do the new recommendations say?
The current recommendations maintains most of the previous diagnostic criteria, but importantly they improve on earlier versions by better defining clinical features and diagnostic biomarkers. Importantly, it provides guidance on the most optimal methods to determine and interpret the clinical features of Dementia with Lewy bodies.
The recommendation agrees that essential to a diagnosis of Dementia with Lewy bodies is dementia. This may not occur in the early stages of the condition, but it will become more evident as the disease progresses. Problems with attention tests, executive function and conceptualising what one is seeing may occur early.
In addition to this there are four core clinical features (the first three of which generally appear in the early stages of the condition):
- Fluctuations in cognition – occurring as spontaneous alterations in attention, and mental arousal
- Recurrent, complex visual hallucinations – these occur in up to 80% of people with DLB
- REM sleep behaviour disorder – recurrent dream enactment behaviour; often proceeds the cognitive issues
- One or more of the characteristic features of Parkinson’s disease – occurs in over 85% of people with DLB
The new recommendations also includes new supportive clinical features, such as hypersomnia (or excessive daytime sleepiness), depression, and severe sensitivity to anti-psychotic drugs.
There is also new guidance on ‘indicative biomarkers‘ for Dementia with Lewy bodies, which include:
- Reduced dopamine processing as determined by brain imaging – this is usually tested by a DAT-Scan similar to Parkinson’s disease. The image below demonstrates normal dopamine processing (bright yellow regions) in the control brain (left) and Alzheimer’s brain (AD, right) when compared to the Dementia with Lewy bodies brain (DLB) in the middle:

DAT-Scan of normal control brain (left), DLB (middle), and AD (right). Source: Asanagi987
- Abnormally low iodine-metaiodobenzylguanidine scintigraphy – this is a scan of the nerves around the heart (Click here for a good OPEN ACCESS review of this topic). In the image below, you can see such a scan of the torso, with the liver apparent at the bottom of each image and the region of interest being the heart (the dotted circle in the top row). Note the lack of grey pixels in the heart of the DLB subject (in the dotter circle).

Scintigraphy of Alzheimer’s disease (AD), Dementia with Lewy bodies (DLB) and normal control (NC). Source: PMC
- Relative preservation of medial temporal lobe structures on brain scans (CT/MRI) – people with Alzheimer’s disease show greater shrinkage of medial temporal lobe structures of the brain than people with Dementia with Lewy bodies. In the image below you can see a CT brain scan from a 61-year-old man with Dementia with Lewy bodies (DLB) and a 69-year-old male with Alzheimer disease (AD). Note the lack of shrinkage of the medial temporal lobes in the circled area in panel A when compared to panel B.
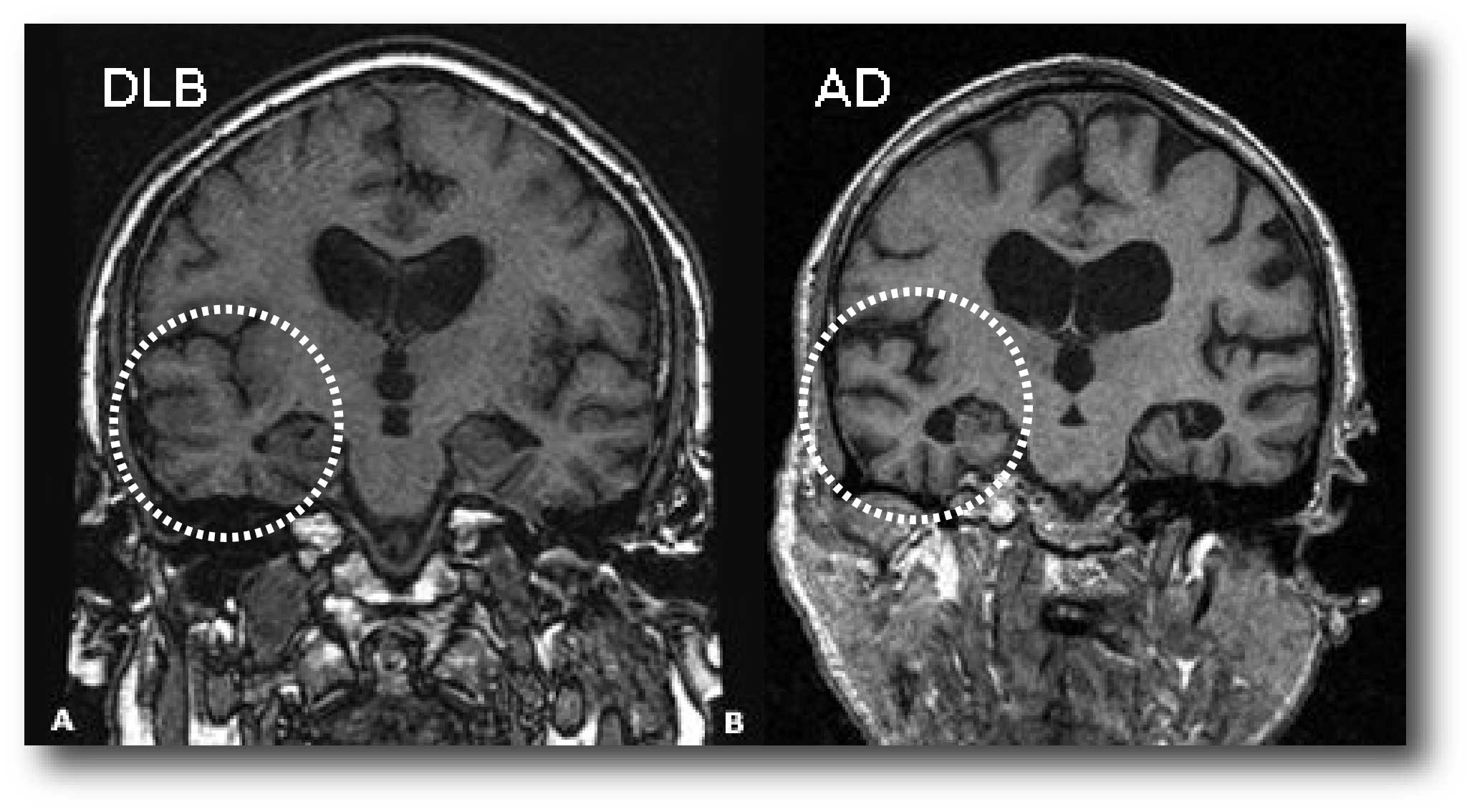
Temporal lobe size in a brain scan. Source: Cursoenarm
- Reduced activity in the visual region of the brain – this is also determined by brain imaging tests (FDG-PET imaging). As you can see activity (indicated in red) in the visual region of the brain (blue arrows) is well preserved in Alzheimer’s disease (AD) and Normal controls (NC), but reduced in Dementia with Lewy bodies (DLB):

The visual region of the brain is on the left of each image. Source: PMC
Next the recommendations focus on clinical management. Treatment of Dementia with Lewy bodies is focused on the cognitive, psychiatric, motor, and other non-motor symptoms which represent the core features of the condition. For cognitive issues, the recommendations propose the use of cholinesterase inhibitors in Dementia with Lewy bodies, as previous studied have shown improving cognition, global function, and activities of living (Click here for more on this). The report is less excited about the use of Memantine in Dementia with Lewy bodies, suggesting that the benefits are less clear, but the drug is well-tolerated and may be used either as monotherapy or in conjunction with cholinesterase inhibitors.
For depression, the report is in agreement with general advice on depression in cases of dementia, that is that the use of selective serotonin re-uptake inhibitors are options in Dementia with Lewy bodies. On the treatment of Parkinsonisms, the report notes that people with Dementia with Lewy bodies are often less responsive to dopaminergic treatments than in people with Parkinson’s disease. In addition, the use dopamine-based medication may also be associated with an increased risk of psychosis in Dementia with Lewy bodies. Levodopa can be used at very low doses to help minimise the effects of Parkinsonisms.
On pathological features/examination of the Dementia with Lewy bodies brain, the report suggests few changes from the previous report.
In summarising the recommendations, the report suggests that “In order to best advance DLB research, global harmonization efforts are required to create networks of researchers and research participants who share common platforms for data and biomarker collection, outcome measures for clinical–translational research, and shared terminology across language, cultures, and traditions”.
What does it all mean?
There are some cases of Parkinson’s disease that may not necessarily be Parkinson’s disease. We currently have about a 10% error rate when we re-visit cases at the postmortem stage. In addition, there are different kinds of Parkinsonisms that can account for some misdiagnosed cases of Parkinson’s disease (such as vascular Parkinsonism or multiple systems atrophy). Dementia with Lewy bodies falls into this latter set.
There are people who present a very “Parkinson’s disease” -like set of physical features when they arrive at the clinic. But as their condition continues, it becomes apparent that they may actually be affected by Dementia with Lewy bodies. Hopefully the new set of guidelines will help in providing better assessment, diagnosis and care for those affected individuals, and spare individuals who – as in the case of Robin Williams – have been misdiagnosed and left unsure and asking questions.
The banner for today’s post was sourced from BMJ.

{kind=link}
Thanks – seems well written from my lay understanding
LikeLike
It’s interesting to see that one or more of the features of Parkinson’s occur in over 85% of people with LBD. I just found out my aunt has LBD so I’ve been doing some research to understand it more. Thanks for the information-I’ve learned a lot about LBD today.
LikeLike
Hi Oscar,
Thanks for your comment – glad you liked the post. There are a lot of interesting overlaps between all of the various conditions (Parkinson’s, Parkinson’s plus, & LBD). It will be interesting to see what the new year brings with regards to research and clinical trial results.
All the best,
Simon
LikeLike
Neuropathologist can not differentiate at autopsy between parkinson’s disease with dementia and Dementia with lewy bodies, hence term lewy body dementia for both diseases. These may be different diseases to clinicians who focus on symptoms; but for a pathologist, they are the same basic disease, a synucleinopathy. Most common is 3rd variation, Incidental Lewy body disease; persons with Lewy bodies in brains,but no clinical manifestations.
LikeLike