
|
Recently researchers have provided very interesting evidence that a form of vitamin B3, called Nicotinamide Riboside, may have beneficial effects for Parkinson’s. Their data suggests that nicotinamide riboside was able to rescue problems in mitochondria – the power stations of cells – in both fly and human cell-based models of Parkinson’s. And the results also suggest that this treatment could prevent the neurodegeneration of dopamine producing neurons. In today’s post, we will discuss what nicotinamide riboside is, what is does in the body, how it may be having its beneficial effect, and we will consider the pros and cons of taking it as a supplement. |

My pile of research reports to read. Source: Reddit
We have a serious problem in biomedical research at the moment.
Serious for ‘planet research’ that is (Good for ‘planet patient’! – click here to understand this sentence).
The problem is very simple: there is too much research going on, and there is now too much information to be absorbed.
There has been an incredible increase in the number of research reports for ‘Parkinson’s’:

For Parkinson’s research alone, every day there is about 20 new research reports (approximately 120 per week). It used to be the case that there was one big research report per year. Then progress got to the crazy point of one big finding per month. And now things are ‘completely kray kray’ (as my 5 year old likes to say), with one new major finding every week!
On top of this, everyday there are new methodology reports, new breakthroughs in other fields that could relate to what is happening in PD, new clinical trial results, etc… The image below perfectly represents how many researchers are currently feeling with regards to the information flow:

How I feel most days. Source: Lean
Don’t get me wrong.
These are very exciting times, big steps are being made in our understanding of conditions like Parkinson’s. It’s just that it is really hard keeping up with the amazing flow of new data.
And this is certainly apparent here on the SoPD website. Occasionally, a few days after I publish something on a particular topic on the SoPD website, a fascinating new research report on that same topic will be published. When I get a chance to read it, I will sometimes add an addendum to the bottom of a post highlighting the new research.
Every now and then, however, the new research deserves a post all of its own.
Which is the case today.
A week after I published the recent Vitamin B3/Niacin post, a new study was published that dealt with a different form of Vitamin B3, called Nicotinamide Riboside. And the results of that study were really interesting.
Wait a minute. Vitamin B3 comes in different forms?
Yes it does. There are three forms to vitamin B3:
- Nicotinic acid (NA or Niacin)
- Nicotinamide (Nam)
- Nicotinamide riboside (NR)

The different forms of Vitamin B3. Source: Longecity
All three forms are used by your body in the production of nicotinamide adenine dinucleotide.
What is nicotinamide adenine dinucleotide?
Nicotinamide adenine dinucleotide (or NAD) is a protein that plays a very critical role in a wide range of cellular reactions. Importantly, it is a required co-factor in a process of passing hydrogen electrons from one protein to another, which is essential for the continued production of energy (in the form of ATP) by the mitochondria in cells.
Mitochondria are the power stations of each cell. They help to keep the lights on. Without them, the party is over and the cell dies. They are tiny bean shaped objects that reside inside of almost every cell in your body.
How do they supply the cell with energy?
They convert nutrients from food into Adenosine Triphosphate (or ATP). ATP is the fuel which cells run on. Given their critical role in energy supply, mitochondria are plentiful (some cells have thousands) and highly organised within the cell, being moved around to wherever they are needed.

Source: Mangomannutrition
Without NAD, the production of ATP starts to go wrong very quickly. NAD is present in every cell and it is essential for normal functioning.
How are the three forms of vitamin B3 involved in NAD production?
NAD is produced two ways:
- a de novo pathway (the production of fresh NAD)
- a salvage pathway (the recycling of NAD)
The schematic below is basically what the production of NAD looks like:

NAD production. Source: Wikipedia
On the left side of this image is the de novo production pathway, while on the right is the circular salvage pathway.
In the de novo route, an essential amino acid called ‘tryptophan‘ (Trp) is the starting point for the production of NAD. And this applies to the vast majority of vertebrates and single cell organism investigated thus far. Tryptophan is used in the body to make proteins (like NAD) and certain brain-signaling chemicals. In the production of NAD, it is converted into quinolate (QA), which is then converted to Nicotinic acid mononucleotide (NaMN).
Now one issue with this initial pathway, however, is that whole “and certain brain-signaling chemicals” part in the paragraph above. You see, tryptophan is also used in the production of the chemical serotonin (which is a neurotransmitter, like dopamine). Given the importance of both NAD and serotonin production, the body has a second method of producing NAD – and this is where Nicotinic acid (or niacin) comes into the story.
Nicotinic acid can also be used to produce Nicotinic acid mononucleotide (NaMN).
NaMN is then transferred to form nicotinic acid adenine dinucleotide (NaAD), which in turn forms nicotinamide adenine dinucleotide (NAD). And that is basically the de novo production pathway.
NAD production. Source: Wikipedia
Now, NAD is so critical for normal functioning that cells can not rely solely on the de novo pathway for their supply. Thus, they have developed a system of recycling NDA, which is called the ‘salvage pathway’.
On the salvage pathway, cells can recycle NAD and (as you can see on the right side of the image above) that involves two of the forms of vitamin B3 (Nicotinamide (Nam) and Nicotinamide riboside (NR)) in a cycling process.
Both nicotinamide (Nam) and nicotinamide riboside (NR) can be used to produce nicotinamide mononucleotide (NMN), which in turn can be converted into NAD. Nicotinamide riboside (NR) is converted to nicotinamide mononucleotide (NMN) by nicotinamide riboside kinase enzymes while nicotinamide (Nam) is converted into nicotinamide mononucleotide (NMN) by nicotinamide phosphoribosyltransferase (NAMPT – try to remember this one, we’ll be coming back to it further below).
And using these de novo and salvaging methods, a cell can keep itself supplied with NAD. If this process of NAD production is of interest to you, click here for a very good review of the topic.
Ok, enough of the biology lesson – let’s move on.
So what new research has been published?
Last week, this report was made available:

Title: The NAD+ Precursor Nicotinamide Riboside Rescues Mitochondrial Defects and Neuronal Loss in iPSC and Fly Models of Parkinson’s Disease.
Authors: Schöndorf DC, Ivanyuk D, Baden P, Sanchez-Martinez A, De Cicco S, Yu C, Giunta I, Schwarz LK, Di Napoli G, Panagiotakopoulou V, Nestel S, Keatinge M, Pruszak J, Bandmann O, Heimrich B, Gasser T, Whitworth AJ, Deleidi M.
Journal: Cell Rep. 2018 Jun 5;23(10):2976-2988.
PMID: 29874584 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers were interested in the cellular response resulting from a disruption in a region of DNA that is referred to as GBA.
What is ‘GBA’?
GBA is a gene – a section of DNA that provides the instructions for making a particular protein. In the case of the GBA gene, the protein is an enzyme, called Glucocerebrosidase. Genetic variations in the GBA gene are some of the most commonly associated genetic risk factors for Parkinson’s.
What does Glucocerebrosidase do?
Glucocerebrosidase (also known as GCase) helps with the digestion and recycling of glucocerebrosides inside cells. The enzyme is located and active inside ‘lysosomes‘.
What are Lysosomes?
Lysosomes are small bags of degradative enzymes – like glucocerebrosidase – that can be found inside of cells.
On a continual regular basis, small parts of the external layer of the cell membrane is brought inside the cell. This is a process called endocytosis. It occurs when the cell consumes resources from the outside world in order to find what it needs to function and survive. As a section of cell membrane is brought into the cell, it forms a vesicle (which is a term used to refer to small spherical bags of stuff inside cells). Given the process by which that vesicles was formed, it is referred to as an endosome (sometimes it is also called a vacuole).

Source: Socratic
Once the endosome is inside the cell and detached from the rest of the membrane, it will bind to another vesicle which is called a lysosome. And as I mentioned above, lysosome is a small bag that is full of digestive enzymes, which help to break down the contents of the endosome.

How lysosomes work. Source: Prezi
The lysosome will fuse with the endosome/vacuole and the enzymes from the lysosome will mix with the material in the vacuole and digest it (or it break down into more manageable components).
Now, in this new study, the investigators collected skin cells from people with GBA genetic mutations and they converted those skin cells (or fibroblasts) into neurons via a trick of molecular biology. Those skin cells became induced pluripotent stem (or iPS) cells (which you can read about by clicking here). And these iPS cells can be encouraged to become any cell that you want, such as a neuron (or brain cell).
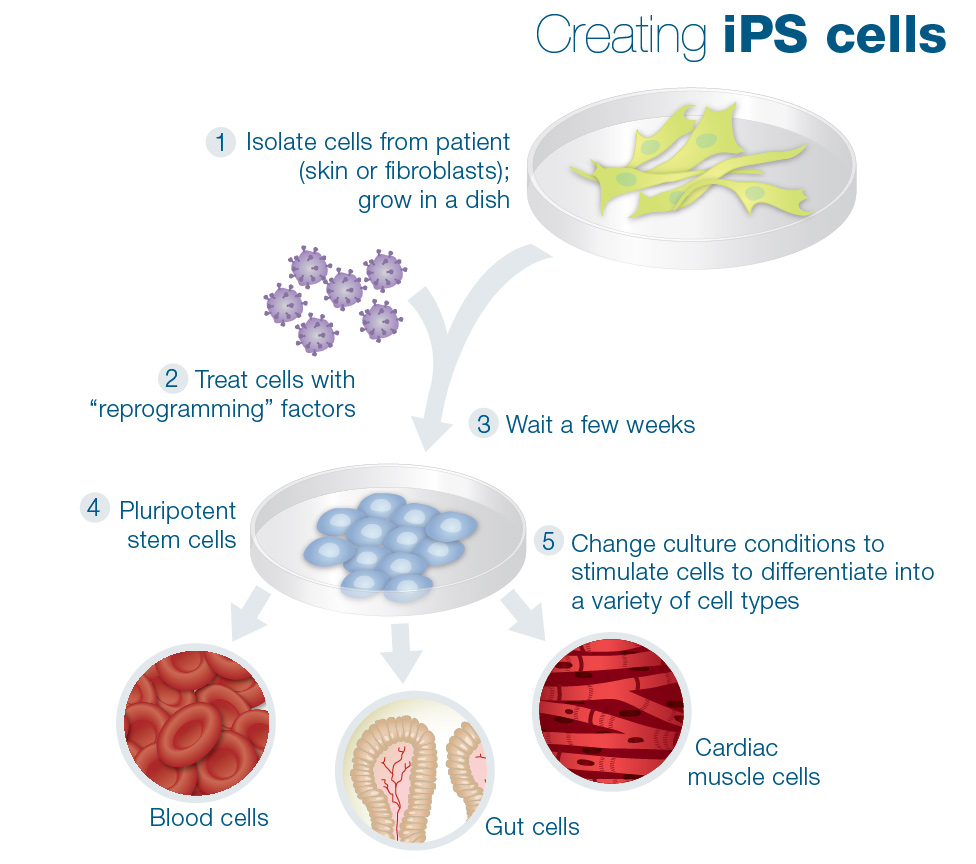
Making IPS cells. Source: learn.genetics
When the researchers compared the biology of the neurons derived from people with GBA genetic mutations with neurons from healthy control subjects, they found that the GBA cells had significant differences in their normal biology… beyond the usually reported lysosomal issues.
For example, the GBA mutation neurons displayed signs of endoplasmic reticulum stress.
What is the endoplasmic reticulum?
The endoplasmic reticulum (or ER) is the assembly line where proteins are produced in a cell. It is closely attached to the nucleus of the cell.

The endoplasmic reticulum. Source: Britannica
The nucleus is where the blue prints/designs for each protein are kept in the form of DNA. A template of each plan for a protein can be generated (in the form of RNA), and that is converted (via a process called translation) into protein. A large part of that protein production process is conducted in the endoplasmic reticulum.
When the endoplasmic reticulum is under stress, the production of protein is not optimal.
The researchers also found that the GBA mutations were having an impact on the function of the mitochondria. As I mentioned above, mitochondria are the bean-shaped power stations of each cell.
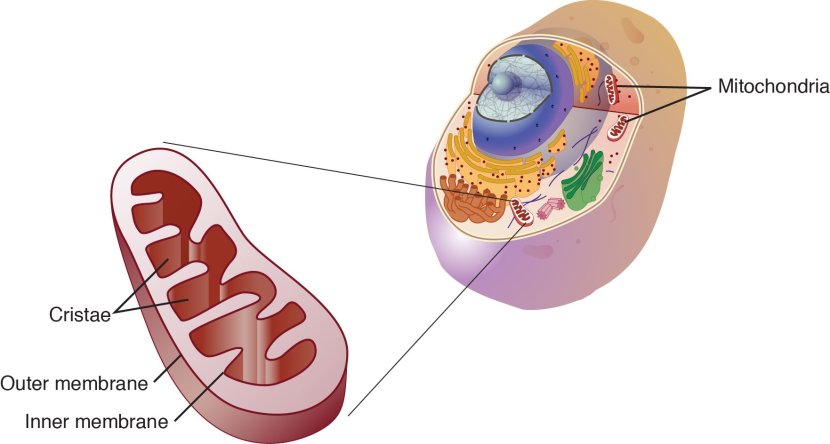
Mitochondria and their location in the cell. Source: NCBI
The researchers reported that the cells carrying GBA mutation cells displayed mitochondria with morphological and functional defects.

Altered morphology in the GBA mitochondria. Source: Cell
The microhondria in these cells also exhibited significantly reduced basal respiration and oxygen consumption rates, suggesting that the mitochondria were under performing in their task.
What does any of this have to do with the NAD production we discussed above?
Well, a great deal of NAD production, use and salvaging occurs in and around the mitochondria.
And when the researchers looked at NAD levels in the cells carrying GBA mutations, they found significant differences in the levels of key components of the NAD production process.
Next, the investigators wanted to know if they could rescue these issues in NAD production in the cells carrying GBA mutations. They started by treating normal control neurons with nicotinamide (NAM), nicotinamide mononucleotide (NMN), or nicotinamide riboside (NR), and then measuring NAD levels.
They found that nicotinamide mononucleotide (NMN) and nicotinamide riboside (NR) had the strongest effect in boosting NAD levels.
Given that nicotinamide riboside has previous been shown to be safe in humans, the researchers focused their attention on treating the cells carrying GBA mutations with nicotinamide riboside. They found that nicotinamide riboside treatment significantly improved many aspects of mitochondria function.
Remarkably, nicotinamide riboside treatment also increased levels of autophagy in the cells carrying GBA mutations. Autophagy being the waste disposal system of the cell.
And finally, the researchers wanted to test whether the response they were observing in cells could also be seen in living animals. They chose genetically engineered flies for this purpose:

Flies. Source: TheConservation
Flies carrying GBA genetic mutations suffer an age-dependent loss of dopamine neurons (similar to the situation in Parkinson’s in humans) and this cell loss is accompanied by progressive defects in the ability of the flies to climb. When the investigators treated flies carrying GBA mutations with nicotinamide riboside, they reported a significant reduction in the number of dopamine neuron dying, and a rescue of climbing ability in the flies.
The scientists concluded their study by suggesting that nicotinamide riboside “may be a valuable therapeutic approach due to its high bioavailability, minimal toxicity, and evidence of its ability to cross the blood-brain barrier”. They also proposed that “future studies will explore the potential therapeutic benefits of combining NAD boosters with chaperones and GCase activators”.
Wow! This is really interesting. Where can I get me some of that nicotinamide riboside stuff?
Nicotinamide riboside is a widely available supplement, but there is a small catch: it is rather pricey.
A company called Chromadex controls the intellectual property (the patents) for production and use of nicotinamide riboside.

Most of those patents were awarded between 2010 and 2012 (they were originally issued to Dartmouth University, Cornell University, and Washington University). Chromadex started sell nicotinamide riboside to suppliers under the label NIAGEN™ in 2013. They also now sell Niagen to customers under the label ‘Tru Niagen’.
In 2014, Chromadex started supplying other companies with nicotinamide riboside. One of those companies is called Elysium Health, which claimed to include nicotinamide riboside as an ingredient in their product Basis.
![]()
But this particular arrangement… um, well it turned ugly… and then lawyers got involved… and it got even uglier! There are blog posts on the web with titles like ‘The legal battle to end all legal battles’ describing this sad tale (Click here and here to learn about different levels of ugly). Chromadex has stopped supplying Elysium with Niagen, and it is unclear where Elysium is now acquiring their nicotinamide riboside.
If you are looking for a product that contains nicotinamide riboside, check the list of ingredients and make sure it contains wording something along the lines of “ChromaDex Inc.’s proprietary Nicotinamide Riboside ingredient, Niagen®. Niagen is a registered trademark of ChromaDex, Inc.”
Is Niagen safe?
Naigen has been tested to very high levels in rodents:

Title: Safety assessment of nicotinamide riboside, a form of vitamin B3
Authors: Conze DB, Crespo-Barreto J, Kruger CL.
Journal: Hum Exp Toxicol. 2016 Jan 20. pii: 0960327115626254.
PMID: 26791540
In this study, the researchers conducted 14-day and 90-day rat toxicology studies. The study basically looked at weight change in organs such as liver, kidneys and brain following treatment. There was also some more detailed (histological) analysis, but this did not include the brain. The lowest observed adverse effect level for Niagen was 1000 mg/kg/day, and no observed adverse effects were found at 300 mg/kg/day.
TWO IMPORTANT DETAILS TO NOTE HERE:
- PLEASE DO NOT USE THOSE LEVELS OF NIAGEN AS A GUIDE AS THEY WERE CONDUCTED IN RODENTS.
- NO ASSESSMENT OF NIAGEN ACCESSING THE BRAIN WAS MADE IN THIS STUDY (ONLY THE WEIGHT OF THE BRAIN WITH/WITHOUT TREATMENT WAS REPORTED).
More recently, a clinical study was conducted on healthy humans and this report was published:

Title: Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults.
Authors: Martens CR, Denman BA, Mazzo MR, Armstrong ML, Reisdorph N, McQueen MB, Chonchol M, Seals DR.
Journal: Nat Commun. 2018 Mar 29;9(1):1286.
PMID: 29599478 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers conducted a 2 × 6-week randomised, double-blind, placebo-controlled crossover clinical study, in which participants ingested either Niagen (500 mg, twice per day) or a placebo for 6 weeks before being blindly shifted to the opposite treatment. The results suggest that Niagen was well tolerated and effectively at stimulating a 60% increase in NAD levels in the blood of healthy middle-aged and older adults (30 participants in total) when compared to placebo-treated levels.
Another (shorter) clinical study found similar results with Niagen treatment (Click here to read those results).
And there has also recently been a placebo-controlled, double-blinded clinical study, funded by the company Elysium, investigating the safety of the product Basis in 120 healthy older (60-80yrs) adults people has also been published. The participants who took the normal recommended dose of Basis for a month saw a 40 percent increase in their NAD blood levels. Those who took the higher dose (twice the recommended amount) saw a 90 percent boost (Click here to read the research report).
PLEASE NOTE: NO INVESTIGATION OF THE COMPONENTS OF NIAGEN OR BASIS ACCESSING THE BRAIN WERE MADE IN EITHER OF THESE CLINICAL STUDIES.
Is there any other research looking at nicotinamide riboside in models of Parkinson’s?
No, there isn’t (and please correct me if I’m wrong here).
The research report reviewed in today’s post is the first to look at nicotinamide riboside in the context of Parkinson’s. Thus, while the new results are very interesting, there is currently very little additional evidence supporting the use of nicotinamide riboside for Parkinson’s.
There has been evidence published, however, suggesting some neuroprotective properties for nicotinamide riboside in other brain-related conditions, such as:

Title: Stimulation of nicotinamide adenine dinucleotide biosynthetic pathways delays axonal degeneration after axotomy.
Authors: Sasaki Y, Araki T, Milbrandt J.
Journal: J Neurosci. 2006 Aug 16;26(33):8484-8491.
PMID: 16914673
In this study, the researchers found that nicotinamide riboside treatment could delay axonal degeneration in cell cultures (dorsal root ganglion cells).
And more recently, nicotinamide riboside treatment has been shown to have beneficial effects in worm and mouse models of Alzheimer’s:

Title: Enhancing mitochondrial proteostasis reduces amyloid-β proteotoxicity.
Authors: Sorrentino V, Romani M, Mouchiroud L, Beck JS, Zhang H, D’Amico D, Moullan N, Potenza F, Schmid AW, Rietsch S, Counts SE, Auwerx J.
Journal: Nature. 2017 Dec 14;552(7684):187-193.
PMID: 29211722 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers observed that nicotinamide riboside significantly increased the fitness and lifespan of genetically engineered worms that produce too much of the Alzheimer’s-related protein beta amyloid. Nicotinimade riboside was also reported to reduce the aggregation of beta amyloid protein in these worms, as well as reducing aggregate levels in cells and a mouse model of Alzheimer’s.
And perhaps as a result of this (and other similar results – Click here and here to read those) there is now a double blind clinical trial recruiting people with mild cognitive impairment/early Alzheimer’s to take Niagen for 10 weeks (Click here to read more about this clinical trial). There is also a second clinical trial seeking to find a safe and cost-effective strategy for decreasing age-related memory loss (Click here to read more about that trial).
But it is important to understand that there is currently very little in the way of supporting evidence for nicotinamide riboside in the context of ‘Parkinson’s’.
Is there any other research suggesting any associations between Parkinson’s and NAD processing?
Yes, there is.
Other parts of the NAD pathway have been investigated, and of particular interest is nicotinamide phosphoribosyltransferase (NAMPT – up near the top of this post I told you to remember this component of the NAD production process).
If you recall from the biology lesson, nicotinamide (Nam) is converted into nicotinamide mononucleotide (NMN) by NAMPT.

NAMPT’s place in the world. Source: Alivebynature
And there was some interesting research related to NAMPT and Parkinson’s published a couple of years ago:

Title: Integrative transcriptomic meta-analysis of Parkinson’s disease and depression identifies NAMPT as a potential blood biomarker for de novo Parkinson’s disease.
Authors: Santiago JA, Littlefield AM, Potashkin JA.
Journal: Sci Rep. 2016 Sep 29;6:34579. doi: 10.1038/srep34579.
PMID: 27680512 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers found that the levels of NAMPT were higher in the blood of recently diagnosed, drug-naive people with Parkinson’s. The levels were not high enough for NAMPT to be considered a potential biomarker for early PD, but the results suggest that something NAD-related in happening in people with Parkinson’s.
And there has been investigations of NAMPT in models of Parkinson’s:

Title: NAMPT protects against 6-hydroxydopamine-induced neurotoxicity in PC12 cells through modulating SIRT1 activity
Authors: Zou XD, Guo SQ, Hu ZW, Li WL.
Journal: Mol Med Rep. 2016 May;13(5):4058-64.
PMID: 27035562
In this study, the scientists took two groups of cells and treated them with either an inhibitor of NAMPT (called FK866) or nicotinamide mononucleotide (NMN – the product of NAMPT activity). This resulted in the cells either having lower levels of NAD (with FK866 treatment) or higher levels of NAD (with NMN treatment). The researchers then treated the cells with a neurotoxin (6-OHDA) and observed what happened.
I’m sure by now you can probably guess the results.
NMN treatment markedly reduced the negative effects of the neurotoxin, while FK866 treatment made the situation for the neurotoxin exposed cells a lot worse.
And this research is supported by similar results from an independent group of scientists:

Title: Nicotinamide mononucleotide improves energy activity and survival rate in an in vitro model of Parkinson’s disease.
Authors: Lu L, Tang L, Wei W, Hong Y, Chen H, Ying W, Chen S.
Journal: Exp Ther Med. 2014 Sep;8(3):943-950. Epub 2014 Jul 14.
PMID: 25120628 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers used a different neurotoxin (rotenone) but observed similar results by treating their cells with nicotinamide mononucleotide (NMN) – the production of NAMPT. Nicotinamide mononucleotide treatment restored NAD levels in the neurotoxin treated cells. The investigators concluded that “NMN may be a promising therapeutic drug for PD”.
And there are suggestions that this need for niacin could be beneficial in genetic forms of Parkinson’s:

Title: Enhancing NAD+ salvage metabolism is neuroprotective in a PINK1 model of Parkinson’s disease<
Authors: Lehmann S, Loh SH, Martins LM.
Journal: Biol Open. 2016 Dec 23. pii: bio.022186.
PMID: 28011627 (this article is OPEN ACCESS if you would like to read it)
In this study, the researchers analysed flies with genetic mutations in the Parkinson’s associated PINK1 gene. They found that PINK1 mutant flies have decreased levels of NAD and problems with their mitochondria (the power stations of each cell – Click here to read a previous post on PINK1 and mitchondria).
The researchers were curious to determine if a diet supplemented with compound that can help increase the production of NAD would rescue the mitochondrial defects observed in the PINK1 mutant fly. Specifically, they fed the flies a diet high in the NAD precursor nicotinamide (or Nam). They found that not only did nicotinamide rescue the mitochondrial problems in the flies, but it also protected neurons from degeneration.
OK, so it may not all be ‘Parkinson’s-related’ or ‘nicotinamide riboside-related’, but you have to admit that it sounds very positive, right?
Yeah,… I guess it does…
I have a terrible feeling that there’s a ‘but’ coming?
Well, it is a hypothetical ‘but’.
What do you mean?
The thing with a lot of these beneficial biological pathways (such as NAC – Click here for a previous post on this), is that too much of a good thing can be bad… in unforeseen ways.
And there are some concerns within the research community about the unknown consequences of raising levels of NAD in the body, particularly from the stand point of cancer. There is now research that suggests raising NAD levels may not be such a great idea if there is the risk of certain types of cancer (particularly brain cancer):

Title: NAMPT overexpression induces cancer stemness and defines a novel tumor signature for glioma prognosis.
Authors: Lucena-Cacace A, Otero-Albiol D, Jiménez-García MP, Peinado-Serrano J, Carnero A.
Journal: Oncotarget. 2017 Aug 28;8(59):99514-99530.
PMID: 29245920 (This report is OPEN ACCESS if you would like to read it)
In this study, the investigators found that high levels of NAD resulted in gliomas – the most lethal and prevalent primary brain tumors in adults – becoming resistance to therapies that target these tumors (such as Temozolomide). They also found that increasing NAMPT levels (which we just discussed above) in glioma cell lines increases the tumorigenic properties of these cells. The investigators reported that blocking NAMPT function in glioma cells increased their chances of dying, which led them to conclude that inhibiting NAMPT represents a very interesting therapeutic target for brain cancer.
And other research groups have found similar results (Click here to read more about this).
Now please note that this is not scaremongering, and that none of the research published thus far suggests that increasing NAD levels via supplements can or will cause an increase in the risk of brain cancer. We are discussing it here simply because it is a hypothetical risk, and researchers have expressed concern about these sorts of unknown risks of raising NAD levels.
I see. Are there good natural sources of nicotinamide riboside?
Unfortunately food is not a great source of nicotinamide riboside.
The highest levels are found in milk.
A study published in 2016, measured how much of this nicotinamide riboside is found in organic and conventional cow’s milk:

It concluded that an 8 ounce (~200mls) glass of conventional milk will have about 0.90 µmol of nicotinamide riboside.
Yeast is another potential source of nicotinamide riboside – it was in yeast that this NAD precursor was first discovered (Click here to read more) – but yeast also contains very small levels of nicotinamide riboside.
And some of you may be thinking that since yeast is used in the production of beer…
Guess what?
Sadly, to date, no research has been published on the levels of nicotinamide riboside in beer, so this food group is probably best not used as a source of this NAD precursor.
So what does it all mean?
Phew, long (winding) post.
(Congrats if you are still reading this in just one sitting – I’ll make this summing up very brief and the next post will be shorter. I promise).
New research identifies another form of vitamin B3 – nicotinamide riboside – that displays beneficial effects in models of a specific version of Parkinson’s. The results are very interesting and suggest that this particular vitamin deserves further investigation. It would certainly be interesting to see what effects nicotinamide riboside has beyond GBA-associated issues.
I will be following with interest any new research that gets published on this topic. And you can be sure that it will get a mention here on the SoPD.
ADDENDUM: 11/07/2018
It has just come to my attention (thanks Chris), that a clinical trial of Nicotinamide Riboside is being set up in Norway. Being led by Dr Charalampos Tzoulis of the University of Bergen, the NOPARK Study will be a randomised, double-blind trial involving 200 participants with newly diagnosed Parkinson’s. They will be randomly and blindly assigned (on a 1:1 ratio) to either the nicotinamide riboside group or the placebo group, and they will be treated and observed for 52 weeks.
The primary outcome measure will be efficacy, based on the MDS-UPDRS (‘Movement Disorder Society Unified Parkinson’s Disease rating Scale’ – a clinician-based rating scale) and the secondary outcome will be levels of NAD metabolites in the blood.
The study has not yet started recruiting, but they hope to report results in October, 2021. For more information regarding this study, please click here.
EDITOR’S NOTE: The information provided by the SoPD website is for information and educational purposes only. Under no circumstances should it ever be considered medical or actionable advice. It is provided by research scientists, not medical practitioners. Any actions taken – based on what has been read on the website – are the sole responsibility of the reader. Any actions being contemplated by readers should firstly be discussed with a qualified healthcare professional who is aware of your medical history. While some of the information discussed in this post may cause concern, please speak with your medical physician before attempting any change in an existing treatment regime.
In addition, some of the companies mentioned in this post are publicly traded companies. That said, the material presented on this page should under no circumstances be considered financial advice. Any actions taken by the reader based on reading this material is the sole responsibility of the reader. None of the companies have requested that this material be produced, nor has the author had any contact with any of the companies or associated parties. This post has been produced for educational purposes only.
The banner for today’s post was sourced from biochemj

{kind=link}
dairy seems like a complicated topic —
Parkinsons disease and bacteriophages as its overlooked contributors
George Tetz, Stuart Brown, Yuhan Hao
doi: https://doi.org/10.1101/305896
https://www.biorxiv.org/content/early/2018/04/22/305896
LikeLike
Hi Diana,
Thanks for the comment. Yes, this manuscript has received a lot of media attention. Given that the research hasn’t been through the peer-review process I am reluctant to say too much about it yet, but given a lot of other recent research on the topic of potential bacterial/viral influencers in Parkinson’s there may be a post on this topic coming soon. I have a personal bias for the idea of viral load playing a role in PD, and this research is very interesting to me. And the issue of dairy has been discussed in a previous post (https://scienceofparkinsons.com/2016/12/07/milk-yes-milk-and-parkinsons-disease/).
Kind regards,
Simon
LikeLike
I found fully 32 nutrients on pubmed.com indicated for PD, many limiting or dissolving TAU protein clumps.
Mucuna Pruriens was the most promising, w long range human studies showing comparability w the effects of drugs
w/out side effects associated w the limited terms of effectiveness of the pharmaceuticals.
LikeLike
I would also like to thank you for the effort that you put in to send out these articles. They highlight relevant research that I certainly would not have access to and would not understand anyway.
LikeLike
Great article! I wish we knew the % of people with PD who had mitochondrial dysfunction. Just not enough clearly defined subtypes it seems to me…
Simon, if you’re able to reply, can you please explain “rescue” in the context of scientific papers? To me it implies that those little fruit flies were climbing poorly, then started climbing better after treatment.
I’m hoping to be rescued if that’s the correct definition.
LikeLike
Hi Paul,
You are welcome. Thanks for the kind comment.
Simon
LikeLike
Hi Double,
Glad you liked the article – I hope all is well. A recent research report (https://www.ncbi.nlm.nih.gov/pubmed/29270838) has suggested that mitochondrial issues occur throughout the Parkinsonian brain, including areas that are usually spared from the cell loss (such as the cerebellum). But this is a hotly debated topic. I am not sure if the percentage of this could even be worked out as mitochondrial performance is reduced in all of us as we age. It would be a very grey statistic.
‘Rescued’ is an overly used word in Parkinson’s (and all of biological) research. Sometimes it means a statistically significant shift in the number of cell surviving or improved motor performance on a given task, but this may only be a partial recovery. And other times the word ‘rescue’ involves a complete restoration of function. As researchers livelihoods rely on how well they can sell the impact of their research, it is probably best to assume the former (statistically significant shift) when reading the word ‘rescue’ rather than the latter (complete restoration).
Are you feeling rescued of any confusion? Or have I simply confused the situation further?
Kind regards,
Simon
LikeLike
Thanks Simon! I guess I need to dig deep to the data and not the language 🙂
I visit here frequently to be ‘rescued’ of confusion, ‘protected’ from ignorance, and to have my fears ‘ameliorated’.
You really make a difference for us.
LikeLike
Very helpful article. I’ve been considering NR for a relative who has PD, but have a few concerns regarding safety, specifically for someone who has PD.
Looking at the chart that shows how NR enables increased production of NAD+ from its breakdown products (i.e., “recycling” of NAD+), I see that one by-product of this increased NAD+ production is additional ADP-ribose.
This article from 2014 is titled “Poly (ADP-ribose) in the pathogenesis of Parkinson’s disease.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4206713/
The article shows that poly ADP-ribose (PAR) enables a process of cell death called parthanatos (essentially, death by PAR).
From that article:
“A recent report on Parkinson’s disease animal model demonstrates that poly (ADP-ribose) (PAR) dependent cell death, also named parthanatos, is accountable for selective dopaminergic neuronal loss. Parthanatos is a programmed necrotic cell death, characterized by PARP1 activation, apoptosis inducing factor (AIF) nuclear translocation, and large scale DNA fragmentation…
“Using NAD+ as a substrate, PARP can elongate ADP-ribose chains via a (1→2) O-glycosidic bond…
“Cells can die due to excessive generation of PAR (11) which is considered as a cell death messenger. This type of cell death is termed parthanatos, as previously mentioned, by combining “PAR” and the word “Thanatos” which refers to the god of death in Greek mythology (25)…
“[P]arthanatos definitely contributes to several types of cell death including neurodegeneration…
“[A] recent study using PD mouse models suggested that PAR-dependent cell death is dominant in slowly progressing dopaminergic neurodegeneration in vivo…
“PARP1 is exceptionally abundant in nigra dopaminergic neuronal cell types compared to others (i.e., approximately three times more abundant in nigra dopaminergic neurons compared to other neurons or astrocytes). Although PARP1 is quite an abundant nuclear protein in general, the additional pool present in dopaminergic neurons may provide a broader window of PAR regulation. It is conceivable that dopaminergic neurons may be more keenly susceptible to parthanatic cell death, in response to the same PARP1 activating stimuli…
“AIMP2-PARP1 signaling pathway in vivo suggests that parthanatos could be involved in slowly progressing dopaminergic neurodegeneration in PD. Speculation on how to prevent dopaminergic cell loss in PD may now be expanded to specifically target the parthanatic cell death cascade.”
According to this other article, when NAD+ breaks down into ADP-ribose, that ADP-ribose gets aggregated into chains that then damage neurons through inducing the release of AIF (cell death effector).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4450718/
Figure 2 of that article purports to show the elongation of ADP-ribose into poly ADP ribose (PARP) chains.
I have *not* found any information that specifically associates NR with any deleterious effects on PD progression, or even any articles that make a connection between NR and parthanatos. But putting two and two together (maybe getting five) I have some concerns about that possibly occurring. The several safety studies that you mention, while fine to assessing acute effects, do not seem to be of sufficient duration to assess possible negative effects upon PD progression. Although, the drosophila study that shows actual improvements in climbing ability is somewhat encouraging in thinking that, whatever the negatives, there could be an overall benefit.
A further concern is that when I read accounts from people taking NR in crowdsourced reviews of Niagen, while there are many positive reports, a significant minority report negative effects such as extreme headaches.
I’d be very interested to hear your thoughts regarding whether the above concerns seem valid.
LikeLike
Hi Lou,
Thank you very much for your really interesting comment – brilliant stuff. I also appreciate and have a lot of respect for the proactive approach you are taking to help your relative.
My apologies for the delay in responding to your question, but it was one which has required some homework and consulting of NAD experts. The short answer is ‘Yes, it could be detrimental if excess PAR is not metabolised quickly’. And the second half of that sentence is key.
It is important not to view biological processes like the NAD pathway in isolation. There are checks and balances for each step in this process – enzymes that monitor each enzyme – to make sure the system is running smoothly. But this is also where variations between individuals can come into play, and it is impossible to predict how each person is going to react to a particular treatment. At present we simply do not have the methods of determining this.
PAR metabolism is mediated by PAR polymerases (PARPS) and PAR glycohydrolase (PARG). In contrast to the family of PARPs, only one gene for PARG has been detected in mammals and insects. So there could be a bit of vulnerability in the system there. Different people may have different levels of PARG (due to differences in the regulation of PARG levels). This is why it is wise (if one is inclined to do so) to gradually start NAD-based supplements in a graded fashion (and always in consultation with one’s clinician). The system should be able to adapt over time, as opposed to a sudden overload of high dose supplement.
And there has very recently been a study published that was looking at this issue of dysregulation of redox resulting from too much Nicotinamide Riboside supplementation being applied too quickly (https://www.ncbi.nlm.nih.gov/pubmed/30007015). After 21 days the researchers observed problems in the treated animals, but the important thing to note in this study was the dosing of 300mg/kg in rats. That is equivalent to 48mg/kg in human which means 3400mg per day
(https://www.fda.gov/…s/ucm078932.pdf). That is a crazy amount of NR supplement. Almost 3.5 times the dose being tested in the NOPARK clinical trial mentioned above.
So long-answer-short, yes there could be PAR-associated issues with NAD-based supplements, but at present we are not sure on how to determine which dose will work for which individual. This will require more research.
I hope this helps.
Kind regards,
Simon
LikeLike
Sorry, I did not notice your very informative reply until just now. So, the crux of the matter is whether the PAR can be cleared away promptly by the usual mechanisms. And the expectation would be that it could be, but, we can’t be entirely sure whether that will in fact occur for any given individual.
Regarding the anecdotal reports of issues with Niagen, here are some unpleasant symptoms, taken exclusively from one-star reviews on Amazon (see link below). Now, there are a lot more good reviews for this product than bad ones, but still, you have to wonder – what caused these problems? And, is it possible that whatever caused them could result in long-term bad effects for even those who initially got good results? Here are some of the problems reported:
terrible insomnia
terrible nightmares if/when I happened to finally fall asleep for an hour
panic attacks, anxiety and raised my diastolic & systolic BP by 20+ points, increasing potential of stroke risk for me. Went to my doc yesterday and the nurse noticed my BP was 160 over 138 which is way high. Stopped taking niagen today, and my BP is back to normal with meds.
Gave me heart palpitations.
caused a powerful feeling of lethargy that persisted for several days after I stopped taking it. It was undeniable and unpleasant. I was drained of motivation to get things done and quickly tired of common tasks.
intense thirst
INTENSE fatigue each day, increasing to such an extent that by the 10th day I could barely get out of bed.
After taking for 2 weeks developed constant headache, nausea and fatigue.
First day I took two caps and I couldn’t sleep. Chaulked it up to stress. Second day I took it I felt like my heart was going to blow out my chest. Waited a couple days, only took one capsule and back to not sleeping and feeling anxious.
I took this for a month and felt terrible from day 1. I was extremely groggy all day everyday, had zero energy and felt like crap. I also had headaches everyday to every other day. I’ve been off of it for 2 days now and already feel much better.
Gave me terrible diarrhea and gas.
For the first few days I felt great. But increasingly i became spacey and found it hard to concentrate. Plus I became edgy and emotional. After two weeks I was either crying over nothing or in an absolute rage. This was completely out of character for me. The only new thing I had added or changed was this product. I stopped immediately and noticed improvement within a couple of days. Now I’m back to normal.
Extreme fatigue for me.
Made me sick. It gave me headaches and diarrhea. I then tried to cut down to 1 pill a day instead of two. Still headaches. Then I tried one pill every other day. Still headaches and didn’t fell good on it. As soon as I stopped, I felt much better.
I took one pill for three days and I was like a speed freak.
Looking at the above, it seems that these symptoms are not inconsistent with what one would expect from neuroinflammation. And my working hypothesis regarding NR leading to more NAD+ leading to more ADP-ribose leading to more PAR leading to parthanatos/neuroinflammation could be an explanation for this.
Your go-slow approach might well have worked for those posting these results. And, there might be tremendous benefit for those who do not have these issues. But personally, I am skittish in the face of such reports, and probably will not be trying this until some more specific and reassuring information is uncovered.
LikeLike
There’s one review in particular, from a poster self-identified as a physician, that seems to show initial benefits followed by troubling symptoms:
“As a physician, I experimented with Niagen after reading about its effects on animals. During the first week of medication, I started to recall more of my dreams; I also felt more energetic in my three day a week 3 mile runs, which could be placebo since I had no objective measurement. After about a month, I experienced some pressure on my chest and checked my pulse, which became irregular. I’m healthy otherwise, on no medication except for multivitamins and Omega 3. I did an EKG and detected some PAC’s (premature atrial contractions), which could be normal for a 62 y/o man. I also experienced cramping at times in my calf muscles during my routine 3 mile runs. The irregular heart beat got worse after less than three months of taking Niagen. I stopped Niagen, and the irregular heart beats resolved after two days. I searched literatures and found an article in the Journal of the American College of Cardiology Jan. 2008 issue, that linked nicotinamide adenosine dinucleotides (NAD) to atrial fibrillation. I don’t have any further information about Niagen; so this is just my personal experience.”
I have no real understanding of the chemistry involved in these reports, but this seems to be the study he is referencing:
https://www.sciencedirect.com/science/article/pii/S0735109707032743?via%3Dihub
I also found this study that did seem to show an effect on the heart, but again, this is just my uninformed dumping of a search result, without understanding the underlying chemistry (which may make all the difference):
https://jbiomedsci.biomedcentral.com/articles/10.1186/s12929-016-0267-y
Anyway, again, I’m avoiding NR at this point based on fear rather than on any true understanding of its hazards.
LikeLike
Thanks for your amazing contributions toward understanding PD. Is there any research on PD and NAD IV?
LikeLike
Hi John,
Thanks for the comment – glad you like the website. There was a study back in the early 1990s that compared oral NADH and intravenous infusion NADH and the conclusion was that the results were comparable (https://www.ncbi.nlm.nih.gov/pubmed/8101414). So while I appreciate that there are lots of companies offering intravenous NAD etc, there may not be a big difference from the oral version.
I hope this helps.
Kind regards,
Simon
LikeLike
It gave me heart palpitations at night as I try to go to sleep.
LikeLiked by 1 person
So, I found this article in Parkinson’s News Today from Oct. of 2018 that claims NAD makes Parkinson’s Disease symptoms worse… in mice?
https://parkinsonsnewstoday.com/2018/10/10/nicotinamide-exacerbates-motor-symptoms-of-parkinsons-disease-in-mice/
LikeLiked by 1 person
Hi Louiscsr,
Thanks for your comment. It is an interesting research report. The model used in that study had a different mechanism of action compared to many of the others, which is discussed by the authors in the discussion section of the report. It something to keep in mind when exploring these agents – that the model used may be effecting the outcome of the study.
Kind regards,
Simon
LikeLike
Whenever I receive 5-6 I.V’s of NAD at 1000 mg per dose, most of my PD symptoms are improved by 80-90%. I feel like a new person-energetic, fine motor skills improve, but most of all my horrible back pain (I guess from dystopia?) is gone. The problem is keeping the NAD levels up. I’m considering taking a powdered form of NMN orally everyday – 1000mg to help convert to NAD until I can afford the next round of NAD I.V’s. But they are indeed a life changer!
LikeLike