
|
# # # # Ibuprofen is a nonsteroidal anti-inflammatory drug that is used for treating pain, fever, and inflammation. Previous preclinical research has demonstrated that ibruproen has the ability to reduce the loss of neurons in models of Parkinson’s, and epidemiological data suggests that it may lower the risk of actually developing the condition. Recently published research points towards a specific sub-set of individuals vulnerable to Parkinson’s that ibuprofen may be particularly useful for: LRRK2-genetic variant carriers. In today’s post, we will discuss the origins of ibruprofen, review some of the previous research indicating neuroprotective properties, and do a deep dive into the new LRRK2 data. # # # # |
 Source: BBC
Source: BBC
This story starts in 1953.
And it begins with two chemists – Stewart Adams and John Nicholson (Stewart is the chap in the banner photo at the top of this post holding the container of pills) – who were both working for Boots, a health/beauty retailer and pharmacy chain in the UK.
![]() Source: Boots
Source: Boots
Stewart and John were on a mission: To produce a new drug for rheumatoid arthritis.
You see, in 1953 there were only two drugs available for treating inflammatory pain: a corticosteroid drug and high dose aspirin. And neither of them was ideal. The chemists started their quest by looking for the activity of variations of aspirin, hoping to find a powerful alternative.
 Adams (left) & Nicholson (middle). Source: Boots
Adams (left) & Nicholson (middle). Source: Boots
Their search was not easy – it took 16 years and they screened over 20,000 molecules – but output of that effort was a drug called ibuprofen (sold under ‘Brufen’).
Legend has it that Adams initially tested the drug on himself as treatment for a particularly bad hangover (Source).
Ibuprofen was launched on the 3rd February 1969 as a treatment for rheumatoid arthritis in the United Kingdom, and it was introduced in the United States in 1974. It went on to become one of the most prescribed drugs in history and it is still widely used. In fact in 2015, Boots UK sold an average of one pack of ibuprofen every 2.92 seconds and, across all UK retailers, the sales figures for the medicine reached over £150 million.
This is all very interesting, but what does it have to do with Parkinson’s?
Well, ibuprofen has some interesting properties, which were highlighted in the early 2000s:
 Title: Ibuprofen protects dopaminergic neurons against glutamate toxicity in vitro.
Title: Ibuprofen protects dopaminergic neurons against glutamate toxicity in vitro.
Authors: Casper D, Yaparpalvi U, Rempel N, Werner P.
Journal: Neurosci Lett. 2000 Aug 11;289(3):201-4.
PMID: 10961664
In this study, the researchers wanted to examine whether treating cultured rodent neurons with aspirin, acetaminophen, or ibuprofen could protect cultured dopamine neurons from an over stimulation (excitotoxicity) of a neurotransmitter called glutamate. They found that ibuprofen could protect both dopaminergic and non-dopaminergic neurons, suggesting possible neuroprotective properties for this treatment.
And this result was replicated by other research groups, including in animal models of Parkinson’s (Click here and here for some early examples).
Then in 2003, this report was published:
 Title: Nonsteroidal anti-inflammatory drugs and the risk of Parkinson disease.
Title: Nonsteroidal anti-inflammatory drugs and the risk of Parkinson disease.
Authors: Chen H, Zhang SM, Hernán MA, Schwarzschild MA, Willett WC, Colditz GA, Speizer FE, Ascherio A.
Journal: Arch Neurol. 2003 Aug;60(8):1059-64.
PMID: 12925360 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers examined medical and health-related data collected from the records of 142,902 US men and women who participated in the two large longitudinal studies, the Health Professionals Follow-up Study (HPFS) and the Nurses’ Health Study (NHS).
|
– Background – Started in 1986, the HPFS sends questionnaires to US health professionals (dentists, optometrists, etc) – aged 40-75 – every couple of years. Participants in the study answer questions dealing with diseases and health-related issues (e.g. smoking, physical activity, etc). The questionnaire is supplemented by another questionnaires which is sent every four years, that deals with dietary information. The NHS study – which was established in 1976 and then expanded in 1989 – has also collected questionnaire-based information from 238,000 registered nurses. Similar to the HPFS, every two years the study participants receive a questionnaire dealing with diseases and health-related topics. – |
The investigators identified 415 cases of Parkinson’s (236 men and 179 women) within the data set. Next, they looked at the medication that individuals were taking at the start of the study and they wanted to see if any of them could be influencing the risk of developing Parkinson’s. They found that participants who reported regular use of non-aspirin nonsteroidal anti-inflammatory drugs (like ibruprofen) at the start of the study had a lower risk of being diagnosed with Parkinson’s during the follow up period than nonregular users.
The pooled multivariate relative risk was 0.55 (95% confidence interval, 0.32-0.96, P =.04). Any number lower than 1.0 indicates a reduced likelihood of an event occurring.
This study was followed up by another report from the same researchers that expanded on the results with a different data set:
 Title: Nonsteroidal antiinflammatory drug use and the risk for Parkinson’s disease.
Title: Nonsteroidal antiinflammatory drug use and the risk for Parkinson’s disease.
Authors: Chen H, Jacobs E, Schwarzschild MA, McCullough ML, Calle EE, Thun MJ, Ascherio A.
Journal: Ann Neurol. 2005 Dec;58(6):963-7.
PMID: 16240369
In this study, the researchers analysed data from the American Cancer Society’s Cancer Preven-tion Study II (CPS-II) Nutrition Cohort, which had collected medical information from 86,404 men and 97,786 women since the study was initiated in 1992.
The results of this study indicated that there was a reduced the risk of developing Parkinson’s among ibuprofen users when compared with nonusers (the relative risks were 0.73 for users of fewer than 2 tablets/week, and 0.62 for 1 or more tablets/day. No association was found for use of aspirin or other nonsteroidal antiinflammatory drugs and reducing PD risk.
The researchers concluded that ibuprofen “use may delay or prevent the onset of Parkinson’s“.
The same researchers have subsequently repeated this analysis and found the same result (Click here to read more about this).
|
# RECAP #1: Preclinical and epidemiological data suggest that the nonsteroidal anti-inflammatory drug ibruprofen may have neuroprotective properties in the context of Parkinson’s. Multiple studies analysing medical data from large cohorts have indicated that regular users of the drug are less likely to develop Parkinson’s. # |
So what does the newly published data suggest?
This is the recently published report:
 Title: Nonsteroidal Anti-Inflammatory Use and LRRK2 Parkinson’s Disease Penetrance.
Title: Nonsteroidal Anti-Inflammatory Use and LRRK2 Parkinson’s Disease Penetrance.
Authors: San Luciano M, Tanner CM, Meng C, Marras C, Goldman SM, Lang AE, Tolosa E, Schüle B, Langston JW, Brice A, Corvol JC, Goldwurm S, Klein C, Brockman S, Berg D, Brockmann K, Ferreira JJ, Tazir M, Mellick GD, Sue CM, Hasegawa K, Tan EK, Bressman S, Saunders-Pullman R; Michael J. Fox Foundation LRRK2 Cohort Consortium.
Journal: Mov Disord. 2020 Jul 14. Online ahead of print.
PMID: 32662532
In this study, the researchers analysed data from two large international study cohorts: the Parkinson’s Disease Genetic and Environmental Modifiers (collected from 26 research sites) and the Michael J. FoxFoundation LRRK2 Cohort Consortium (collected from 14 research sites). These cohorts contained data from 577 individuals – 259 (44.9%) of whom were carriers of a genetic variation in the LRRK2 gene and had Parkinson’s, while the remaining 318 (55.1%) had a genetic variation in the LRRK2 gene, but did not have Parkinson’s.
What is the LRRK2 gene?
A gene is a section of DNA that provides the instructions for a particular protein. A gene is the blue print, which gives rise to RNA (a facsimile of the plans). The RNA can then be used to make protein.
Leucine-rich repeat kinase 2 (or LRRK2 – pronounced ‘lark 2’) – also known as ‘Dardarin‘ (from the Basque word “dardara” which means “trembling”) – is an enzyme that has many functions within a cell – from supporting efforts to move things around inside the cell to helping to keep the power on (involved with mitochondrial function).

The many jobs of LRRK2. Source: Researchgate
The LRRK2 gene – the DNA instructions for making LRRK2 protein – is made up of many different regions. Each of those regions is involved with the different functions of the eventual protein. As you can see in the image below, the regions of the LRRK2 gene have a variety of different functions:
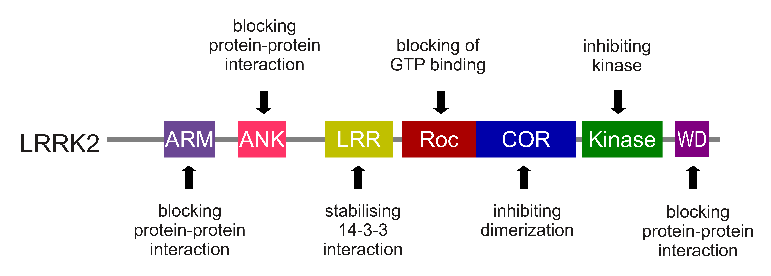
The regions and associated functions of the LRRK2 gene. Source: Intechopen
Genetic variations (tiny errors in the coding of DNA) within the LRRK2 gene are recognised as being some of the most common with regards to increasing ones risk of developing Parkinson’s (LRRK2 variants are present in approximately 1-2% of all cases of Parkinson’s).

The structure of Lrrk2 and where various mutations lie. Source: Intech
As the image above suggests, mutations in the PARK8 gene are also associated with Crohn’s disease (Click here and here for more on this) – though that mutation is in a different location to those associated with Parkinson’s. And one particularly common Parkinson’s-associated LRRK2 mutation – called G2019S – is also associated with increased risk of certain types of cancer, especially for hormone-related cancer and breast cancer in women – Click here to read more about this. If you have a G2019S mutation, no reason to panic – but it is good to be aware of this association and have regular check ups.
The G2019S mutation (the name designates its location on the gene) is the most common LRRK2 mutation. In some populations of people it can be found in 40% of people with Parkinson’s (Click here to read more about this). But what is interesting about this mutation is that it gives rise to a LRRK2 enzyme that is hyperactive.
 LRRK2 protein. Source: Youtube
LRRK2 protein. Source: Youtube
As a protein, LRRK2 interacts with many different types of other proteins, and you can imagine that in a finely balanced environment like the cells that a mutant ‘hyperactive’ form of LRRK2 is going to cause problems. The consequences of this constantly active form of LRRK2 protein is believed to be influential in the cell death in LRRK2-associated Parkinson’s.
Ok, so the researchers were analysing medical data from people with and without Parkinson’s who have a genetic variant in their LRRK2 gene. What did they find?
In their analysis, the researchers divided the LRRK2 genetic variants into two groups:
- Pathogenic variants – these variants increase an individual’s susceptibility to developing Parkinson’s. They are inherited and exhibit an age-dependent nature (G2019S and R1441X are examples of this).
- Risk variants – these variants modestly increase the risk of developing Parkinson’s (G2385R and R1628P are examples of this).
Overall, they found that regular nonsteroidal anti-inflammatory drug use was associated with a reduced risk of developing Parkinson’s (odds ratio, 0.34; 95% confidence interval, 0.21-0.57). An odds ratio lower than 1.0 indicates a reduced likelihood of an event occurring.
And this effect was apparent for both the pathogenic and risk variant subgroups – the odds ratio for the pathogenic variant group was 0.38 (95% confidence interval, 0.21-0.67) and the odds ratio for the risk variant group was 0.19; 95% confidence interval, 0.04-0.99).
Of particular interest, however, is when they focused in on ibuprofen and aspirin separately, they also found the same associations: the odds ratio for ibuprofen use 0.19 (95% confidence interval, 0.07-0.50 and the odds ratio for aspirin was 0.51 (95% confidence interval, 0.28-0.91).
The researchers concluded that the findings support “a growing body of research evidence involving inflammatory pathways in PD pathogenesis“.
The results obviously point towards nonsteroidal anti-inflammatory drugs as being potentially of interest to reducing the risk of developing Parkinson’s. But the researchers acknowledge that “the optimal dose and duration of exposure and the exact mechanisms by which protection may be exerted are, however, unknown“.
|
# # RECAP #2: Genetic variations in the LRRK2 gene are associated with an increased risk of developing Parkinson’s. Newly published research analysing individuals with and without Parkinson’s who also carry a LRRK2 genetic variation indicates that regular use of nonsteroidal anti-inflammatory drugs (like ibuprofen) may reduce the risk of Parkinson’s developing. # # |
I have Parkinson’s, should I start taking ibuprofen?
As I am always saying, I am not a clinician, just a research scientist, and I can not give medical advice here. That said, it is important to understand here that while we have plenty of evidence building that nonsteroidal anti-inflammatory drugs (like ibuprofen) can reduce the risk of developing Parkinson’s, we have very little data that this class of drugs will do anything post diagnosis. Obviously, what is required is a randomised clinical trial to explore this.
There are, however, some important matters to consider about the long term use of nonsteroidal anti-inflammatory drugs (like ibuprofen). Such a treatment regime is associated with significant risks.
Regular use of ibuprofen can cause kidney and liver damage, as well as bleeding in the stomach and bowels. There are also concerns that over use of nonsteroidal anti-inflammatory drugs increase risk of heart attack and stroke (Source).
These drugs are designed for short term use in reducing pain and inflammation.
So, if not ibuprofen than what?
There are a number of clinical trial programs that are testing anti-inflammatory approaches for Parkinson’s. These include inhibiting the inflammasome.
Inflammasomes are multi-protein formations, present inside of cells in your body, and they can amplify the immune response to damage or a pathogen. Recent preclinical research suggests that blocking the inflammasome can rescue models of Parkinson’s (Click here to read a recent SoPD post on this topic)
 Researchers have also reported that the Parkinson’s-associated protein alpha synuclein can promote the activation of inflammasomes in the immune cells of the brain: the microglia.
Researchers have also reported that the Parkinson’s-associated protein alpha synuclein can promote the activation of inflammasomes in the immune cells of the brain: the microglia.
This has given rise to the development of NLRP3 inhibitors (NLRP3 is a key protein involved in inflammasomes). The first of these inhibitors to reach the clinic is Inzomelid, which is being developed by a biotech firm called Inflazome.

In 2019, the company initiated Phase I clinical testing in healthy volunteers (Click here to read more about this). That trial finished in early 2020 (Click here to read more about this), and Inflazome is now preparing for Phase II clinical testing. They are particularly interested in clinically testing their drug in neurodegenerative conditions like Parkinson’s.
In addition to the inflammasome targeting approach, there are other anti-inflammatory treatments being clinically tested.
Researchers at Cambridge University are preparing to test the immunosuppressive medication, Azathioprine, in people with Parkinson’s (Click here to read more about this trial).
 (FULL DISCLOSURE: The author of this blog is an employee of The Cure Parkinson’s Trust, which is a supporter of the AZA-PD study)
(FULL DISCLOSURE: The author of this blog is an employee of The Cure Parkinson’s Trust, which is a supporter of the AZA-PD study)
Another anti-inflammatory approach is being developed by a biotech firm called Inmune Bio.
 This company is developing a drug called XPro1595, which targets soluble TNF. Tumor Necrosis Factor (TNF) is a potent immune signaling molecule (a cytokine) and it is intimately involved in inflammation. But Xpro1595 is different to current clinically approved TNF inhibitors, as it only neutralises soluble TNF, while not affecting trans-membrane TNF (this is an important difference). Inmune Bio has conducted a Phase I clinical study of XPro1595 in individuals with moderate Alzheimer’s (Click here to read more about this trial) and the results of that study have been announced (Click here to read more about this). It would be interesting to see this agent tested in Parkinson’s, perhaps with LRRK2 genetic variant subset analysis.
This company is developing a drug called XPro1595, which targets soluble TNF. Tumor Necrosis Factor (TNF) is a potent immune signaling molecule (a cytokine) and it is intimately involved in inflammation. But Xpro1595 is different to current clinically approved TNF inhibitors, as it only neutralises soluble TNF, while not affecting trans-membrane TNF (this is an important difference). Inmune Bio has conducted a Phase I clinical study of XPro1595 in individuals with moderate Alzheimer’s (Click here to read more about this trial) and the results of that study have been announced (Click here to read more about this). It would be interesting to see this agent tested in Parkinson’s, perhaps with LRRK2 genetic variant subset analysis.
So what does it all mean?
There is accumulating evidence in Parkinson’s research that inflammation is playing a role in the development of the condition.
New data indicates that this is particularly relevant in individuals with genetic variations in their LRRK2 genes. LRRK2 is present at high levels in cells associated with immune response in the body, so it is not surprising that medications like nonsteroidal anti-inflammatory drugs could be having a beneficial effect in individuals carrying LRRK2 variants.
Whether anti-inflammatory therapies can have any effect on the course of the condition post diagnosis is yet to be determined. There is considerable clinical trial activity in this area though and we will hopefully not have to wait too long to have an answer to this question.

All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
EDITOR’S NOTE: The information provided by the SoPD website is for information and educational purposes only. Under no circumstances should it ever be considered medical or actionable advice. It is provided by research scientists, not medical practitioners. Any actions taken – based on what has been read on the website – are the sole responsibility of the reader. Any actions being contemplated by readers should firstly be discussed with a qualified healthcare professional who is aware of your medical history. While some of the information discussed in this post may cause concern, please speak with your medical physician before attempting any change in an existing treatment regime.
In addition, some of the companies mentioned in this post are publicly traded companies. That said, the material presented on this page should under no circumstances be considered financial advice. Any actions taken by the reader based on reading this material is the sole responsibility of the reader. None of the companies have requested that this material be produced, nor has the author had any contact with any of the companies or associated parties. This post has been produced for educational purposes only.
Further, the author of this post is an employee of the Cure Parkinson’s Trust. The Trust has not asked for this post to be written, and there has been no effort to highlight the work of the Trust over others (perceptions of any bias should be directed to the author). This post has been written by the author solely for the purpose of sharing what the author considers interesting information.
The banner for today’s post was sourced from Nottinghampost

Inflammation plays a central role in the motor issues caused by Parkinson’s. I’m less certain of its significance in the spread of aggregated alpha-synuclein through the nervous system as per the Braak process. So damping down inflammation would seem to be directed primarily at damping down the inflammatory process within the nigrostriatal area, which is responsible for the gradual destruction of dopamine neurons there. The other Parkinson’s-related issues like dysautonomia and dementia, might persist, even with a good anti-inflammatory treatment in place.
The problem, as you say, is that long-term treatment with anti-inflammatories like ibruprofen can lead to very serious and deleterious side-effects. I also notice that azathioprine works by reducing white blood cell counts–a very general form of immune suppression–and can have other serious side-effects as well, including cancer, which is especially associated with long-term use.
That is why my partner and I have taken the approach of using a cocktail of over-the-counter anti-inflammatories and anti-oxidants, including curcumin, EGCg, baicalin and NAC, which work synergistically against specific aspects of the inflammatory feedback loop in the nigrostriatal area, while presenting a very benign side-effect profile that allows many patients to use them safely over a long interval.
I’ve written up our approach along with links to studies and review articles that seem to provide support for their use for this purpose. It can be viewed at this location:
https://www.smartpatients.com/conversations/41861
LikeLike