
|
# # # # Over the past two decades, pharmaceutical companies have shifted from maintaining large in-house drug development platforms to a model that involves acquiring small biotech firms with interesting agents once those companies reach a certain point in their maturation. This week a biotech firm called Inflazome was bought by the big pharma Roche. Inflazome has been developing a novel NLRP3 inhibitor, which targets inflammasome activation and the company has had Parkinson’s in it’s sights as far as indications of interest. In today’s post, we will discuss what the inflammasome is, how NLRP3 inhibitors work, and what will be happening next. # # # # |
 Source: Science
Source: Science
One of the hottest areas of Parkinson’s research world is ‘inflammation‘ (cheesy pun intended).
What is inflammation?
When cells in your body are stressed or sick, they begin to release tiny messenger proteins which inform the rest of your body that something is wrong.
When enough of these messenger proteins are released that the immune system becomes activated, it can cause inflammation.
Inflammation is a critical part of the immune system’s response to trouble. It is the body’s way of communicating to the immune system that something is wrong and activating it so that it can help deal with the situation.
By releasing the messenger proteins (called cytokines), injured/sick cells kick off a process that results in multiple types of immune cells entering the troubled area of the body and undertaking very specific tasks.
 The inflammatory process. Source: Trainingcor
The inflammatory process. Source: Trainingcor
The strength of the immune response depends on the volume of the signal arising from those released messenger proteins. And there are processes that can amplify the immune response.
One of those processes is called inflammasomes.
What are inflammasomes?
Inflammasomes are multi-protein formations that are present inside of cells in your body. They detect pathogenic agents or stressors that have found their way inside of cells, and once these inflammasomes detect something that should not be there, they activate the release of highly pro-inflammatory messenger proteins (called cytokines) such as interleukin-1b (IL-1b) and IL-18.
These cytokines are released into the world outside of the cell and alert the immune system that something is not quite right.
 Source: Youtube
Source: Youtube
There are difference types of inflammasomes and they vary based on what activates them. For example, the presence of RNA from a particular virus may activate one type of inflammasome, while a certain toxin will cause the assembly of a different inflammasome.
For the purpose of keeping things simple in today’s post, we are going to focus on one of the most well characterised inflammasomes.
It is called the NLRP3 inflammasome:
 The NLRP3 inflammasome. Source: Twitter
The NLRP3 inflammasome. Source: Twitter
The name of this particular inflammasome is derived from one of the three core components: a protein called NLRP3.
What is NLRP3?
NLRP3 is an abbreviation that is a lot easier to say than “Nucleotide-binding domain, Leucine-Rich-containing family, Pyrin domain-containing-3“.
As I mentioned above, inflammasomes are multi-protein formations. Critically, inflammasomes are made up of three primary components:
- a sensor protein
- an adaptor protein
- a zymogen procaspase-1 (don’t panic about how complicated this last one sounds just yet, we’ll come back to it in a second!).
NLRP3 is a sensor protein.
It act as a “pattern-recognition receptor“. That is to say, NLRP3 is a protein that recognises a particular pattern in the shape or structure of certain ‘activators’ (think, a virus or stressor). These activator patterns are called pathogen-associated molecular patterns (or PAMPs). There are many different forms of sensors, which help to recognise all the various patterns of troublesome agents.
 Activation of NLRP3 inflammasome. Source: Nature
Activation of NLRP3 inflammasome. Source: Nature
When NLRP3 protein is first produced by a cell, it floats around in an inactive state waiting for PAMPs to interact with it and activate it.
NLRP3 can actually be activated by a wide range of agents, including:
- low intracellular potassium concentrations
- Viruses (such as influenza A and Hepatitis C)
- Bacteria (including neisseria gonorrhoeae)
- Bacterial toxins (such as nigericin and maitotoxin)
- Inorganic particles (think titanium dioxide, silicon dioxide, and asbestos)
- Crystallized molecules (like cholesterol crystals and urate crystals in atherosclerosis and gout, respectively)
Once activated, the NLRP3 protein will start binding to other activated NLRP3 proteins and this is the beginning of the formation of a NLRP3 inflammasome.
And this is where the second component of the inflammasome comes into the picture: the adaptor protein
This is getting complicated. What is the adaptor protein?
Don’t panic.
If you are not interested in the biology lesson here, skip down to the first recap and read on from there.
In the NLRP3 inflammasome, there is a protein called PYCARD, which is sometimes referred to as ASC (or “Apoptosis-associated speck-like protein containing a CARD”). This is the adaptor protein. For simplicity sake, for the rest of this post, we will refer to the adaptor protein in the NLRP3 inflammasome as ASC.
An interesting feature of the adaptor protein ASC has recently been shown to act in a prion-like fashion (Click here to read more about this). Emerging evidence suggests that ASC is also released from inflammasome‐activated cells as ‘ASC specks’. These ASC specks accumulate in inflamed tissues, where they can continue to encourage the production of mature cytokines. There is also evidence of interactions with other proteins.
When the NLRP3 protein becomes activated and starts binding to other activated NLRP3 proteins, ASC will bind to it and this process attracts the zymogen procaspase-1.
Ok, now can I panic? That sounds REALLY complicated. What is the zymogen procaspase-1?
A zymogen is simply an inactive precursor of an enzyme, and procaspase-1 is the precursor to the enzyme caspase-1.
And what is caspase-1?
Caspase-1 is the enzyme that causes the release of the proinflammatory messenger protein (the cytokines that we mentioned above), IL-1b and IL-18.
So the take home message here is: By forming an inflammasome, NLRP3, ASC, and procaspase-1 cause the activation of caspase-1 which in turn results in the release of proinflammatory cytokines.
Clear as mud?
|
# RECAP #1: Inflammation is a natural process that our bodies use to let the immune system know that something is wrong. By sending out tiny messenger proteins, damaged cells can activate the immune system to respond. Sometimes a stronger than normal immune response is required and this is where ‘inflammasomes’ can help to amplify the message being sent to the immune system. # |
So blocking the inflammasome could reduce inflammation?
Yes.
But how is any of this related to Parkinson’s?
So next time you are out to dinner with friends, try to drop the word ‘inflammaging’ into the conversation.
‘Inflammaging’?
It is the idea that as we ‘age’, an imbalance occurs in our ability to manage ‘inflammation’ (hence the combination of the words: inflamm-aging).
 Source: PMC
Source: PMC
The proposal is that as we get older there is a chronic low-grade inflammation, which may be influential in later cognitive issues or the development of neurodegenerative conditions like Alzheimer’s and Parkinson’s (Click here for a nice discussion on this concept of inflammaging)
Is there any evidence to support this idea?
There is an accumulating body of evidence supporting the idea of inflammaging (for example, click here, here and here to read some of the reports supporting the notion).
In addition, there has been a lot of preclinical work focused on targetting the inflammasome aspect of inflammation (as a potential approach to treating neurodegenerative conditions) which supports the inflammaging idea.
And the results have been interesting. For example, last year this research report was published:
 Title: Systemic inflammation impairs microglial Aβ clearance through NLRP3 inflammasome.
Title: Systemic inflammation impairs microglial Aβ clearance through NLRP3 inflammasome.
Authors: Tejera D, Mercan D, Sanchez-Caro JM, Hanan M, Greenberg D, Soreq H, Latz E, Golenbock D, Heneka MT.
Journal: EMBO J. 2019 Sep 2;38(17):e101064.
PMID: 31359456 (This report is OPEN ACCESS if your want to read it)
In this study, the researchers found that systemic (wide-spread or whole body) inflammation in mice affects microglia in an age‐dependent manner.
What are microglia?
Microglia are some of the helper cells in the brain – they act as the resident immune cells. When infection or damage occurs, the microglia become ‘activated’ and start cleaning up the area.
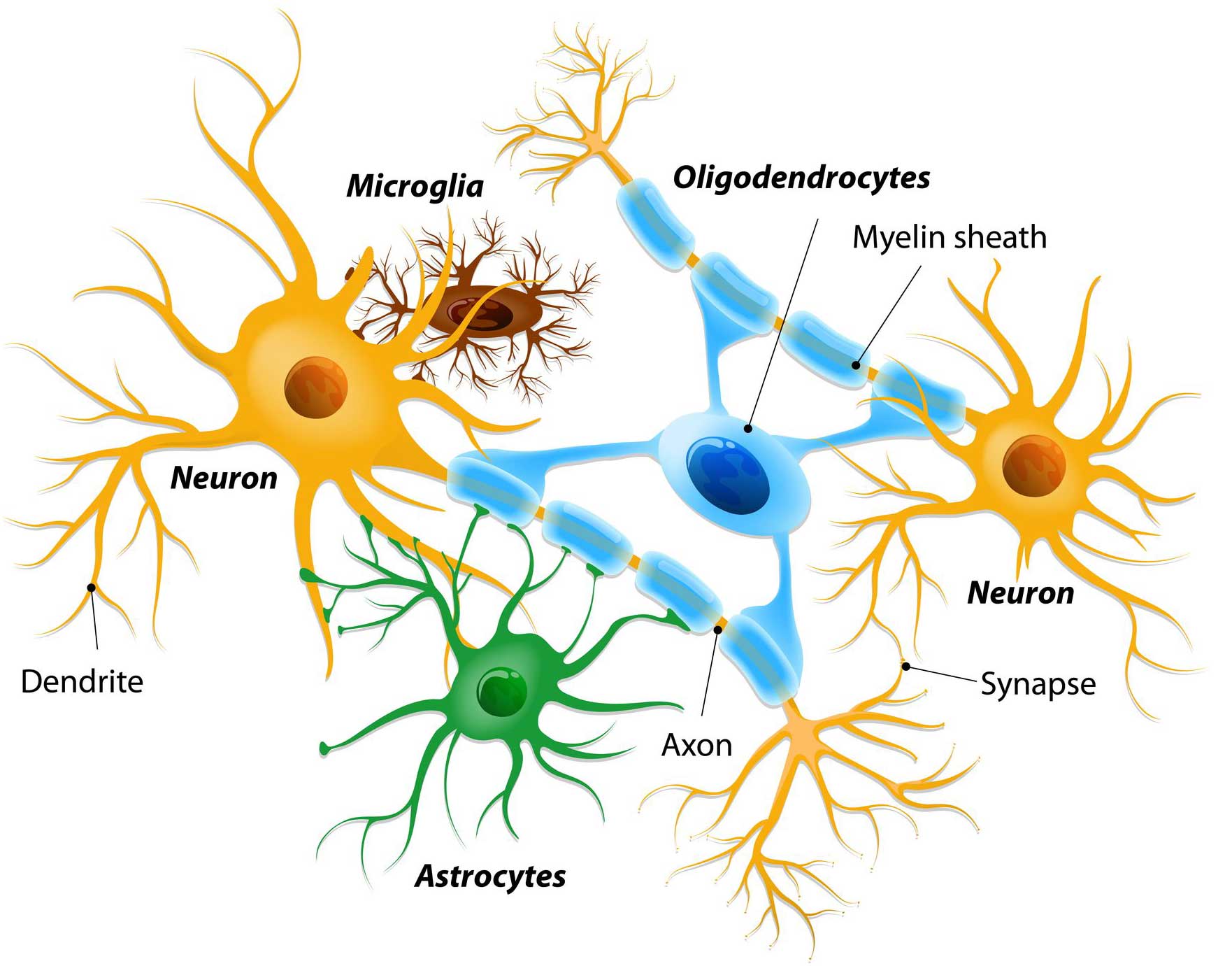 Different types of cells in the brain. Source: Dreamstime
Different types of cells in the brain. Source: Dreamstime
The researchers reported that the response of microglia in aged mice was reduced compared to young mice (when the mice were challenged with systemic inflammation). But when the researchers repeated the experiment in genetically engineered mice which do not produce NLRP3 (a key component of the inflammasomes discussed above), the age-associated reduction was lost – the older mice were the same as the younger mice.
Next the researchers wanted to determine if this NLRP3 effect could influence a mouse model of Alzheimer’s, so they assessed mice that were genetically engineered to produce large amounts of the Alzheimer’s associated protein amyloid precursor protein (APP; bearing both the Swedish mutation and PSEN1 mutation). This genetic manipulation results in mice that display many of the hallmarks of Alzheimer’s, such as the build up of Alzheimer’s beta amyloid associated protein.
These mice usually start to exhibit the accumulation of beta amyloid protein (called plaques) after 5 months of age. So as you can see in the graph on the left side of the image below, at 5 months of age, the APP mice and APP mice with no NLRP3 have similar low levels of plaques (white and light grey columns). There is no difference between the two groups of mice.
 Source: PMC
Source: PMC
But by 15 months of age, the APP mice have much higher levels of plaques in their brains than the APP mice with no NLRP3 (dark grey and really dark grey columns in the left-hand side graph). In addition, the plaques that were present in the 15 month old APP mice with no NLRP3 were smaller than the APP mice with normal NLRP3 function.
This result suggested to the investigators that inflammation may be reducing the ability of microglia (over time with aging) to clear the accumulating beta amyloid protein in the APP mice. By blocking NLRP3 function, this situation appears to be reversed.
And the effect does not appear to be limited to beta amyloid.
These same researchers published another report late last year indicating similar results with Tau protein:
 Title: NLRP3 inflammasome activation drives tau pathology.
Title: NLRP3 inflammasome activation drives tau pathology.
Authors: Ising C, Venegas C, Zhang S, Scheiblich H, Schmidt SV, Vieira-Saecker A, Schwartz S, Albasset S, McManus RM, Tejera D, Griep A, Santarelli F, Brosseron F, Opitz S, Stunden J, Merten M, Kayed R, Golenbock DT, Blum D, Latz E, Buée L, Heneka MT.
Journal: Nature. 2019 Nov 20. [Epub ahead of print]
PMID: 31748742
In this study, the scientists reported that the neurodegenerative protein Tau can activate the NLRP3 inflammasome. Tau is another protein that accumulates in conditions like Alzheimer’s and Parkinson’s (we discussed Tau in the previous SoPD post – click here to read that post).
The researchers also found that loss of NLRP3 function reduced tau aggregation, and prevented cognitive issues and neurodegeneration in a mouse that was genetically engineered to produce high levels of Tau. Importantly, they also demonstrated that pharmacological inhibition of the infammasome (with a drug that inhibits NLRP3) can reduced tau aggregation and the neurodegeneration observed in these mice.
Note here that some of the scientists involved in this and the previous report are associated with a company called IFM Therapeutics – more about this company below.
|
# # RECAP #2: Blocking inflammasome function appears to reduce the pathological signs of neurodegeneration in models of Alzheimer’s. These effects can be achieved via treatment with drugs inhibiting components of the inflammasome (such as NLRP3). # # |
This sounds great for Alzheimer’s, but what about Parkinson’s?
So in late 2018, this report was published:
 Title: Inflammasome inhibition prevents α-synuclein pathology and dopaminergic neurodegeneration in mice
Title: Inflammasome inhibition prevents α-synuclein pathology and dopaminergic neurodegeneration in mice
Authors: Gordon R, Albornoz EA, Christie DC, Langley MR, Kumar V, Mantovani S, Robertson AAB, Butler MS, Rowe DB, O’Neill LA, Kanthasamy AG, Schroder K, Cooper MA, Woodruff TM.
Journal: Sci Transl Med. 2018 Oct 31;10(465)
PMID: 30381407 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers began by assessing postmortem human brains for signs of inflammasome activation. They used samples from 5 late-stage Parkinson’s brains and 5 control brains, and they found evidence of increased cleaved caspase 1 and ASC (hallmarks of inflammasome activation) in the Parkinsonian brains. When they looked at which cell types were producing the markers of inflammasomes in the PD brains, they found that the resident immune cells – microglia – were activated and had increased levels of NLRP3 and ASC.
Next the investigators looked at blood samples collected from 21 people with Parkinson’s and they found further evidence of inflammasome activation, suggesting that a ‘systemic’ (body-wide) increase in inflammasome activity may be occurring in Parkinson’s.
 Source: PMC
Source: PMC
The researchers then shifted their attention to animal models of PD, to determine if inflammasome activation is also occurring. Across multiple models (neurotoxin-based, genetic, and alpha-synuclein preformed fibrils), they found evidence of NLRP3 inflammasome activation.
Given that fribrils of alpha synuclein can cause NLRP3 activation (see above), the researchers in this current study wanted to evaluate the response of microglial cells to preformed fibrils of alpha synuclein protein. They collected microglia cells from normal mice and mice that were genetically engineered to have no NLRP3. They grew these cells as separate cultures and then exposed the cells to preformed fibrils of alpha synuclein protein.
They found that even when normal microglia were exposed to preformed fibrils of alpha synuclein protein, they would start to form characteristic ASC specks and release IL-1b 24 hours later. When microglia with no NLRP3 were exposed to preformed fibrils of alpha synuclein protein there was no release of IL-1b or formation of ASC specks (even at 24 hours after treatment). Interestingly, the alpha synuclein exposure did not cause pyroptosis in the microglia from normal mice.
Given the lack of response in microglia with no NLRP3 protein, the investigators next exposed the normal microglia to a drug called MCC950.
What is MCC950?
MCC950 is a potent small-molecule inhibitor of NLRP3.
Some of the researchers involved in this current study, were also part of a previous study which identified MCC950.
Here is that report:
 Title: A small molecule inhibitior of the NLRP3 inflammasome is a potential therapeutic for inflammatory diseases
Title: A small molecule inhibitior of the NLRP3 inflammasome is a potential therapeutic for inflammatory diseases
Authors: Coll RC, Robertson AA, Chae JJ, Higgins SC, Muñoz-Planillo R, Inserra MC, Vetter I, Dungan LS, Monks BG, Stutz A, Croker DE, Butler MS, Haneklaus M, Sutton CE, Núñez G, Latz E, Kastner DL, Mills KH, Masters SL, Schroder K, Cooper MA, O’Neill LA.
Journal: Nat Med. 2015 Mar;21(3):248-55.
PMID: 25686105 (This report is OPEN ACCESS if you would like to read it)
In 2001, a set of diarylsulfonylurea-containing compounds were identified as potent inhibitors of IL-1b. In this more recent study, the researchers characterised of those compounds (named MCC950). They found that pre-treating cells with MCC950 inhibited ASC speck formation in pro-inflammatory situations, but curiously they also found that MCC950 does not prevent inflammasome formation (by directly blocking NLRP3 oligomerization or NLRP3-ASC interactions). The exact mechanims is still to be determined, but MCC950 was found to be a potent inhibitor of the NLRP3 inflammasome.
In the more recent study, when the investigators exposed normal microglia to preformed fibrils of alpha synuclein protein and treated those cells with MCC950, they witnessed a significant reduction in NLRP3 inflammasome activation. Even at very low doses, MCC950 was able to block the release of IL-1b.
As a result of this result, the researchers next turned their attention to models of Parkinson’s. Three models in fact. They tested MCC950 in a neurotoxin model (6-OHDA), a genetic model (MitoPark), and an alpha synuclein model of PD (pre-formed fibrils).
 A lab mouse. Source: USNews
A lab mouse. Source: USNews
Not only did the reasearchers find that MCC950 entered the brain (crossing the blood brain barrier is one of the great challenges of any PD-oriented treatment), but it also improved motor features and reduced the level of dopamine cell loss in all three of these models of Parkinson’s. In addition, MCC950 was found to be a potent inhibitor of inflammation in the brain, reducing IL-1b, Caspase-1, and ASC levels dramatically.
This is really interesting. What did they do next?
The researchers were interested to have a look at what effect MCC950 treatment may have on the spread of alpha synuclein pathology in the pre-formed fibrils model of Parkinson’s. The analysed the brains of mice 8 months after the fibrils had been injected and they found signs of alpha synuclein in regions beyond the dopamine system in mice that were NOT treated with MCC950 (these regions included the cerebral cortex).
In mice that were treated with MCC950 (following the delivery of pre-formed alpha synuclein fibrils), however, there was a very different picture: While there was no difference in the total amount of alpha synuclein being produced in the brain, there was a marked reduction in the number of alpha synclein aggregates.
These results led the researchers to conclude that that chronic NLRP3 activation contributes to the propagation of pathology seen in the pre-formed fibrils model, and pharmacological inhibition of NLRP3 using MCC950 can effectively reduce this pathological process.
For those interested, this is a video of Dr Richard Gordon (University of Queensland – and one of the lead scientists on the MCC950 study) discussing this work:
|
# # # RECAP #3: Evidence of inflammasomes activation in the Parkinsonian brain has been reported. The Parkinson’s-associated protein alpha synuclein can activate inflammasome, and blocking NLRP3 appears to beneficial in preclinical models of Parkinson’s. MCC950 is a NLRP3 inhibitor being developed for Parkinson’s. # # # |
Are there any clinical trials of MCC950?
This drug has been developed by a company named Inflazome.
And Inflazome has now started a Phase I clinical trials of a variation of this drug, another NLRP3-inhibitor called Inzomelid.
The company completed Phase I clinical studies in ealry 2020 (click here to read more about those investigations) and inzomelid was found to be safe and well tolerated in double-blind evaluations in healthy volunteers (Click here to read more about this).
The agent also exhibited positive results in the treatment of Cryopyrin-Associated Periodic Syndrome (or CAPS). CAPS is a very rare auto-inflammatory disease driven by a mutation affecting the NLRP3 inflammasome. The US FDA has been granted “Orphan Drug Designation” to Inflazome for inzomelid (Click here to read more about this), but the company was also very interested in pursuing Parkinson’s as an additional indication.
We had been awaiting news of Phase II clinical plans but then… well, COVID-19.
But on the 21st September, the inflazome website suddenly disappeared and it was replaced by a single page, which started out with:
 The large pharmaceutical company Roche had decided to purchase Inflazome and take on all of its inflammasome intellectual property.
The large pharmaceutical company Roche had decided to purchase Inflazome and take on all of its inflammasome intellectual property.
 And for those who are worried about big pharma running away from neurodegenerative conditions like Parkinson’s, this is the same Roche that is developing the alpha synuclein immunotherapy prasinezumab which is targetting Parkinson’s (Click here to read a previous SoPD post about this).
And for those who are worried about big pharma running away from neurodegenerative conditions like Parkinson’s, this is the same Roche that is developing the alpha synuclein immunotherapy prasinezumab which is targetting Parkinson’s (Click here to read a previous SoPD post about this).
With the Inflazome acquisition, Roche appears to be planning to advancing inzomelid across multiple inflammation-based indications, starting with a Phase II study for CAPS being conducted in the UK later this year (Source).
The future development of inzomelid will also include Phase II studies for Parkinson’s, and those trials will most likely make use of an NLRP3-targeted PET imaging tracer, that Inflazome has developed with funding from the Michael J. Fox Foundation (Click here to read more about this).
We look forward to learning more about the Parkinson’s trial in the not too distant future.
Is MCC950 the only inflammasome targetting molecule?
No, not at all.
There are numerous biotech companies actively developing clinical programs around the NLRP3 target. For example, above we briefly mentioned IFM Therapeutics.
 On April 1st (no joke) of last year, the major pharmaceutical company Novartis acquired one clinical and two preclinical programs targeting the NLRP3 inflammasome from IFM Therapeutics.
On April 1st (no joke) of last year, the major pharmaceutical company Novartis acquired one clinical and two preclinical programs targeting the NLRP3 inflammasome from IFM Therapeutics.
The clinical program is for a drug called IFM-2427 which is a systemic antagonist of NLRP3 being targeted at an array of chronic inflammatory disorders (including gout, atherosclerosis and nonalcoholic steatohepatitis (NASH)). The two preclinical programs, however, include a gut-directed molecule for the treatment of inflammatory bowel disease but (more importantly) a brain-penetrant molecule which is being developed for targetting neurodegenerative conditions like Alzheimer’s and Parkinson’s (Source).
In addition, another inflammation focused biotech company called NodThera has identified its lead NLRP3 targetting drug candidate, called NT-0167 which the company is now developing for clinical evaluation (Click here to read more about this).
 And one interesting aspect of the recent Inflazome acquisition by Roche is that in late 2018, the biotech company Genentech (which is a subsidiary of Roche), bought up Jecure Therapeutics – a biotech firm with a portfolio of preclinical NLRP3 inhibitors aimed at various inflammatory conditions (Click here to read more about this).
And one interesting aspect of the recent Inflazome acquisition by Roche is that in late 2018, the biotech company Genentech (which is a subsidiary of Roche), bought up Jecure Therapeutics – a biotech firm with a portfolio of preclinical NLRP3 inhibitors aimed at various inflammatory conditions (Click here to read more about this).
![]() For those interested, click here to read more about the biotech efforts to develop NLRP3 inhibitors.
For those interested, click here to read more about the biotech efforts to develop NLRP3 inhibitors.
So what does it all mean?
Chronic inflammation is believed to be playing a role in many cases of Parkinson’s. There is evidence that the inflammasome – an amplifying mechanism for imflammatory processes – may be influential. Biotech firms have been developing inhibitors of the inflammasome, and now their efforts have matured to a point where large pharmaceutical companies are prepared to step in and buying their agents to take forward in clinical development.
2020 has been a dreadful year for many reasons, but as we start preparing the annual review of Parkinson’s research here at the SoPD, it is amazing how much activity there has been despite COVID-19’s best efforts. And one of the quiet area of activity has been in industry acquisitions.
News that inflammasome-focused biotech firm Inflazome was being bought by a pharmaceutical company was no surprise – they are in a red hot field. That Swiss-based Roche was the acquirer was not a big surprise either given their interest in immunology. But as the rest of the world is dealing with COVID, a number of these deals are quietly being done (other examples are Biogen‘s tie up with Denali – Click here to read an SoPD post about this, Bayer‘s acquisition of Asklepios BioPharmaceutical (Asklepios is closely tied with Brain Neurotherapy Bio‘s GDNF gene therapy study), and Bial‘s purchase of Lysosomal Therapeutics – Click here to read more about this – SoPD post in the works).
Ideally, Roche will now be able to put the required resources in place to really drive inzomelid and other NLRP3 inhibitors forward for conditions like Parkinson’s. Hopefully we will learn more about their plans in 2021 (if not before). And one can only wonder if 2020 has a few more acquisition surprises left before we see the back of it.
Few signs here that Pharma is giving up on neurodegeneration.
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
The banner for today’s post was sourced from Inflazome

Here is a short interview with Professor Luke O’Neill regarding Roche buying Inflazome (1st 6 minutes of audio clip). He says this is the “best validated target of inflammation I’ve ever seen in 30 years.” So I’m cautiously hopeful.
https://www.newstalk.com/news/irish-firm-co-founded-prof-luke-oneill-bought-healthcare-giant-e380m-1079371
LikeLike
Can diet help this kind of inflammation?
LikeLike
Hi Pat,
Thanks for the interesting question. Arthritis is an inflammatory condition and researchers have done a lot of work on diet there. The Arthritis Foundation offers a lot of accessible information about diet and inflammation (https://www.arthritis.org/health-wellness/healthy-living/nutrition/anti-inflammatory/anti-inflammatory-diet). The Mayo clinic also has useful information (https://www.mayoclinic.org/healthy-lifestyle/nutrition-and-healthy-eating/in-depth/how-to-use-food-to-help-your-body-fight-inflammation/art-20457586).
I hope this helps,
Simon
LikeLike
Thank you!
LikeLike
It looks like a phase IIb trial of Inzomelid (IZD174) in CAPS was started on Sept 22, 2020.
https://adisinsight.springer.com/drugs/800055306https://www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2020-000489-40
LikeLike
And the trial was ended prematurely on Oct 13, 2020
https://www.clinicaltrialsregister.eu/ctr-search/trial/2020-000489-40/GB
LikeLike
Based on Luke O’Neill’s interviews below, it looks like 6 massive clinical trials at a cost of over 1B Euros are being planned by Roche. Apparently Inzomelid and Somalix will be tested to see how they work for Alzheimer’s, Parkinson’s, Colitis, Asthma, and other diseases.
See the 11:00 mark in the following:
Also, see the 17:15 mark in:
http://www.peoplebehindthescience.com/dr-luke-oneill/
And for more background, Luke O’Neill’s talk on NLRP3 and Metabolic Reprogramming below is worth a look.
LikeLike
Short video by Matt Cooper re Inflazome
LikeLike