Parkinson’s disease is a neurodegenerative condition. That means that cells in the brain (neurons) are dying. By the time the motor features of Parkinson’s disease (rigidity, slowness of movement, and a resting tremor or shaking of a limb) become apparent to an individual, they will have lost 60-70% of the dopamine neurons in a region of the brain called the midbrain.

Above are slices of human brain, taken from the midbrain of a healthy control subject (left) and an individual who died with Parkinson’s disease. The dopamine cells in the control subject can be seen on both sides of the brain with the eye because they produce a chemical (neuromelanin) that makes them black. These cells are noticeably absent in the Parkinsonian brain. Source: Springer
While there is a lot of research investigating how to stop or slow down the disease, at present, the only realistic way to deal with what has already been lost is to replace it. This could be done with cell transplantation.
Cell transplantation has had a long and colourful history of trial and error with regards to Parkinson’s disease. Importantly, given that there is currently no clinically approved cell transplantation procedure for Parkinson’s disease, the approach must be considered experimental, at best. This has not, however, stop numerous unscrupulous practitioners from advertising their services and preying on desperate individuals. They offer expensive operations, that have little if any peer-reviewed scientific evidence backing them.
Let us repeat: there is currently NO clinically approved cell transplantation procedure for Parkinson’s disease.
The history of cell transplantation in Parkinson’s disease
There has been an enormous amount of cell transplant work conducted in rodent models of Parkinson’s disease – in which the dopamine system is lesioned unilaterally. Many different types of cells have been used, but by far the most successful have been immature dopamine neurons (collected from embryos). The success of that work resulted in numerous clinical trials in the 1990s. Those trials began with a group in Lund (Sweden) who, in 1991, transplanted fetal midbrain tissue into six patients: four with advanced idiopathic Parkinson’s disease and two from the ‘Frozen addicts’ cohort (see the book “The case of the frozen addicts” for an explanation of these two individuals). Similar programmes had been initiated in England, Spain, Mexico, Cuba, France, and Belgium. These were all considered to be relatively successful, except for the fact that they were all open-label/not blinded studies, meaning that everyone involved in the study knew who was getting transplanted.
In the USA, these developments took place amid a major debates about the ban on federal funding for fetal tissue research that had been introduced by the Reagan administration in 1988. The Clinton administration lifted this ban in January, 1993, and this reversal opened the way for the National Institutes of Health (NIH) to provide funding for the two placebo-controlled studies. Those two trials were:
Trial no. 1: The Colorado/Columbia Trial:
A double blind trial in which 40 subjects (with advanced PD) received transplants of fetal midbrain tissue and 34 additional subjects (with advanced PD) had a sham surgery and were considered controls. Critically, neither the subjects nor the practitioners knew who was in which group. No patients in either arm of the study received immunosuppression, meaning that their immune systems were free to attack the injected cells (which would have been considered foreign by the body). The patients were followed up for 1 year after surgery and the success of the trial was judged on the basis of a self-report rating of clinical improvement or deterioration, scored by patients in their own homes and then sent to the investigator. The report of the study was published in the New England Journal of Medicine:
Title: Transplantation of embryonic dopamine neurons for severe Parkinson’s disease.
Authors: Freed CR, Greene PE, Breeze RE, Tsai WY, DuMouchel W, Kao R, Dillon S, Winfield H, Culver S, Trojanowski JQ, Eidelberg D, Fahn S.
Journal: New England Journal of Medicine 2001 Mar 8;344(10):710-9.
PMID: 11236774
Trial no. 2: The Tampa Bay Trial:
34 patients were randomly assigned either to receive a transplant of fetal midbrain tissue or to undergo a sham surgery. All patients received 6 months of immunosuppression after surgery. The primary endpoint for this study was a significant difference between the groups at 24 months after surgery. The report of this study was published in the journal, Annals of Neurology:
Title: A double-blind controlled trial of bilateral fetal nigral transplantation in Parkinson’s disease.
Authors: Olanow CW, Goetz CG, Kordower JH, Stoessl AJ, Sossi V, Brin MF, Shannon KM, Nauert GM, Perl DP, Godbold J, Freeman TB.
Journal: Ann Neurol. 2003 Sep;54(3):403-14.
PMID: 12953276
Both of these clinical studies failed to show any significant improvement at their endpoints. In addition, 15% – 50% of transplanted subjects developed what are called ‘graft induced dyskinesias’ (or GID’s). This is where the subjects display uncontrollable/erratic movement. Interestingly, patients under 60 years of age did show signs of improvement on when assessed both clinically (using the UPDRS-III) and when assessed using brain imaging techniques (increased F-dopa uptake on PET). But the overall negative results left a shadow over the technique for the better part of a decade.
So what is currently happening?
There are new clinical trials currently underway for cell transplantation in Parkinson’s disease. Primary amongst these is the Transeuro being conducted in Europe.

The Transeuro trial. Source: Transeuro
The Transeuro trial is an open label study, involving 40 subjects, transplanted in sites across Europe. They will receive immunosuppression for at least 12 months post surgery, and the end point of the study will be 3 years post surgery, and based on brain imaging of dopamine release from the transplanted cells (PET scans). Based on the previous double blind studies discussed above, only subject under 65 years of age have been enrolled in the study.

The European consortium behind the Transeuro trial. Source: Transeuro
Do the transplants slow down the disease?
The evidence thus far is not clear, but some of the original patients from the 1991 Sweden trial were able to stop/cut back on their L-dopa treatment. Recently, some of the patients who received transplants have pass away and their brains have been examined post-mortem. One very interesting finding is that some of the cells in the transplants (1-5%) have lewy bodies in them. This suggests that the disease is passed on to the healthy transplanted cells in some way.

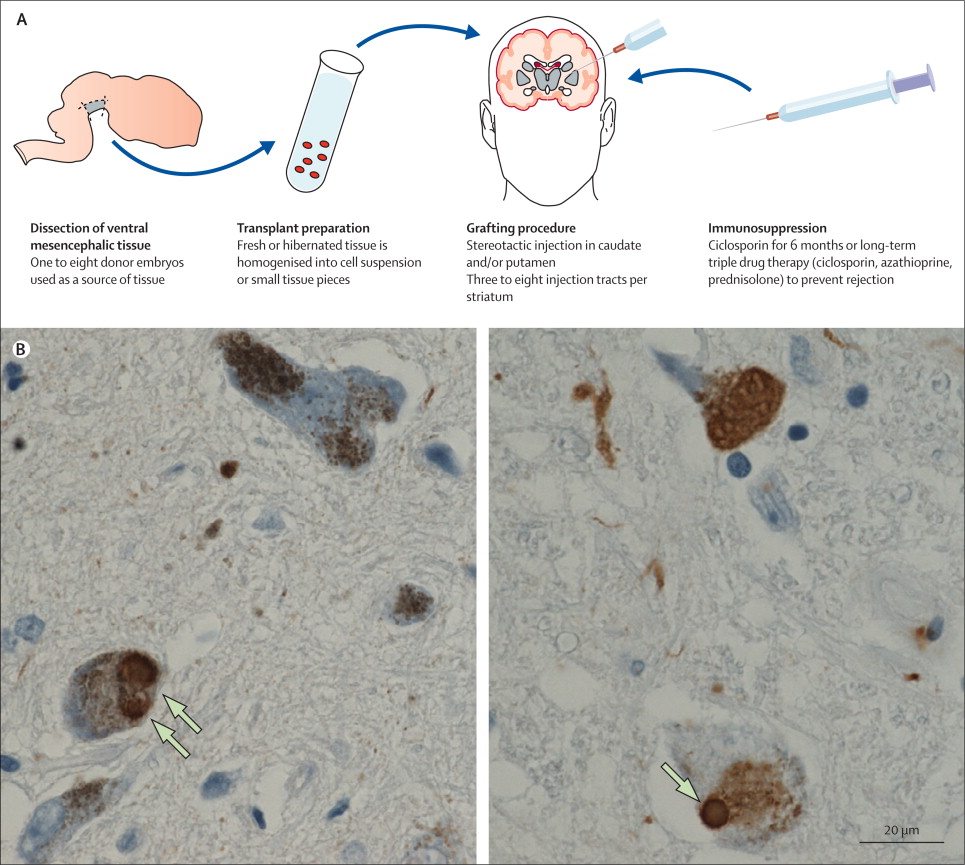
Above are photos of neurons from the post-mortem brains of people with Parkinson’s that received transplants. White arrows in the images above indicate lewy bodies inside transplanted cells. Source: The Lancet
For more information on this, see these articles:
Title: Lewy bodies in grafted neurons in subjects with Parkinson’s disease suggest host-to-graft disease propagation.
Authors: Li JY, Englund E, Holton JL, Soulet D, Hagell P, Lees AJ, Lashley T, Quinn NP, Rehncrona S, Björklund A, Widner H, Revesz T, Lindvall O, Brundin P.
Journal: Nature Medicine. 2008 May;14(5):501-3.
PMID: 18391963
Title: Lewy body pathology in long-term fetal nigral transplants: is Parkinson’s disease transmitted from one neural system to another?
Authors: Kordower JH, Brundin P.
Journal: Neuropsychopharmacology. 2009;3 (1):254.
PMID: 19079079 (this review article is freely available)
Thus it would appear that cell transplantation will not stop the disease. At best it will simply allow us to replace the lost cells and reverse some of the motor related features of the condition. Ideally, this approach would be conducted in concert with additional therapies that slow or halt the disease (such as a vaccine possibly).
What next for cell transplantation?
Given the moral and ethical issues surrounding the use of fetal tissue, research has shifted towards using embryonic stem (ES) cells and turning them into midbrain dopamine neurons. And the results here have been very promising, with recent reports suggesting that ES cells can be converted into dopamine neurons and transplanted into rodent models of Parkinson’s disease with equal efficiency to that of fetal midbrain tissue.

Title: Human ESC-derived dopamine neurons show similar preclinical efficacy and potency to fetal neurons when grafted in a rat model of Parkinson’s disease.
Authors: Grealish S, Diguet E, Kirkeby A, Mattsson B, Heuer A, Bramoulle Y, Van Camp N, Perrier AL, Hantraye P, Björklund A, Parmar M.
Journal: Cell Stem Cell. 2014 Nov 6;15(5):653-65.
PMID: 25517469
The take home message regarding cell transplantation is that at present it represents one of the only ways to replace what has been lost, but as of yet there is not an approved protocol for this approach in humans. As we said above, at best this should be considered experimental, and individuals selling expensive procedures should be avoided. The future looks very bright for this field, however, and we will keep you updated as more information comes to hand.
EDITORIAL NOTE: Happy new year everyone! We look forward to bringing you all the exciting news related to the science of Parkinson’s disease in 2016.