
By the time a person is sitting in front of a neurologist and being told that they have Parkinson’s disease, they will have lost half the dopamine producing cells in an area of the brain called the midbrain.
On this page we will explain what dopamine is and how it relates to Parkinson’s disease.
Dopamine being released by one cell and binding to another. Source: Truelibido
Dopamine is a chemical is the brain that plays a role in many basic functions of the brain, such as motor co-ordination, reward, and memory. It works as a signalling molecule – a way for brain cells to communicate with each other. Dopamine is released from brain cells that produce this chemical (not all brain cells do this), and it binds to target cells, initiating biological process within those cells.
It does this via five different receptors – that is to say, dopamine is released from one cell and can bind to one of five different receptors on the target cell (depending on which receptor is present). The receptor is analogous to a lock and dopamine is the key. When dopamine binds to a particular receptor it will allow something to happen in that cell. And this is how information from a dopamine neuron is passed or transmitted on to another cell. Hence the reason, dopamine is referred to as a neurotransmitter.
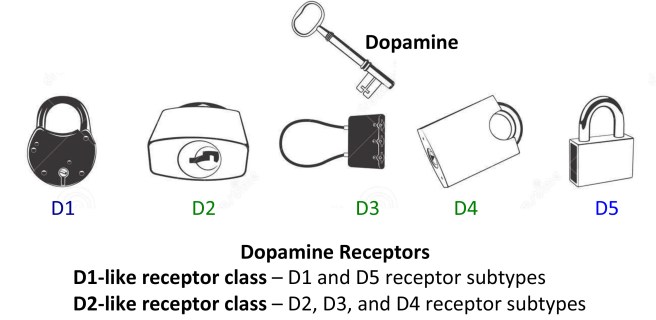
Dopamine acts like a key. Source: JourneywithParkinsons
The five different dopamine receptors can be grouped into two populations, based on the action initiated by the binding of dopamine. Dopamine receptors 1 and 5 are considered D1-like receptors, while Dopamine receptors 2,3 and 4 are considered D2-like receptors. Through these various receptors, dopamine is influential in many different activities of the brain, especially motor co-ordination.
Dopamine in motor co-ordination
When you are planning to move your arm or leg, the process required for actually initiating that action begins in an area of the brain called the motor cortex. It runs across the very top of your brain – from just above your temple to the top of your skull. And the motor cortex is divided into regions that control specific body parts (for example the legs are controlled by the very top of the motor cortex, while mouth and tongue are controlled by regions closer to you temples.
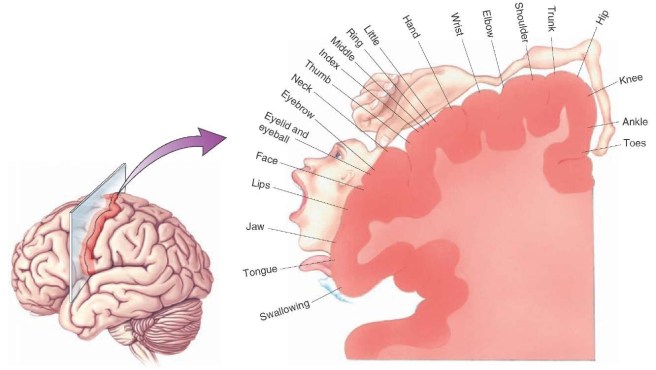
The human motor cortex. Source: What-when-how.com
While the idea of initiating a movement starts in the motor cortex, your ability to actually move is largely controlled by the activity in a specific group of brain regions, collectively known as the ‘Basal ganglia‘.
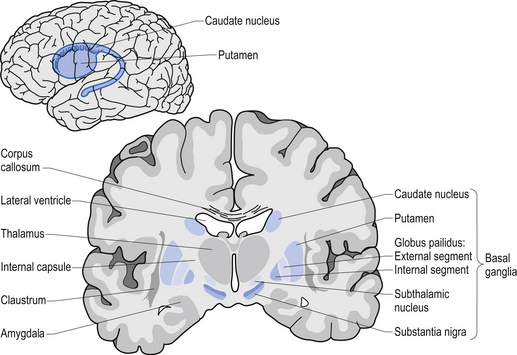
The location of the basal ganglia structures (blue) in the human brain. Source: iKnowledge
The basal ganglia receives signals from the overlying motor cortex, processes that information before sending the signal on down the spinal cord to the muscles that are going to perform the movement.
Think of the motor cortex as excited kids wanting to do something and the basal ganglia as the parental figures deciding if this action is a good idea.
And the most important participant in that basal ganglia ‘regulation’ of movement is a structure called the thalamus.

A brainscan illustrating the location of the thalamus in the human brain. Source: Wikipedia
The thalamus is a structure deep inside the brain that acts like the central control unit of the brain. Everything coming into the brain from the spinal cord, passes through the thalamus. And everything leaving the brain, passes through the thalamus. It is aware of most everything that is going on and it plays an important role in the regulation of movement.
The direct/indirect pathways
The processing of movement in the basal ganglia involves a direct pathway and an indirect pathway. In simple terms, the direct pathway encourages movement, while the indirect pathway does the opposite (inhibits it). The two pathways work together like a carefully choreographed symphony.
The motor features of Parkinson’s disease (slowness of movement and resting tremor) are associated with a breakdown in the processing of those two pathways, which results in a stronger signal coming from the indirect pathway – thus inhibiting/slowing movement.
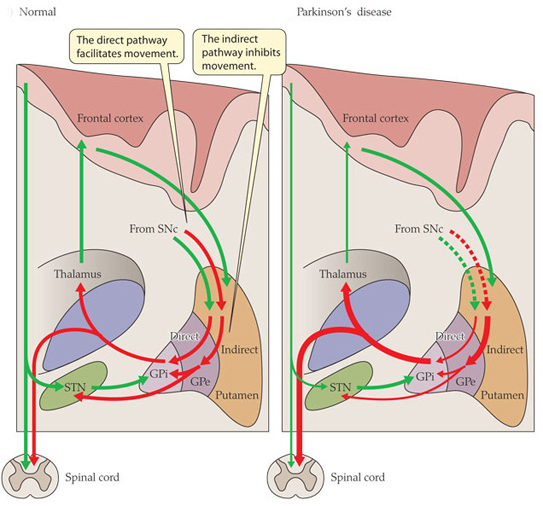
Excitatory signals (green) and inhibitory signals (red) in the basal ganglia, in both a normal brain and one with Parkinson’s disease. Source: Animal Physiology 3rd Edition
Both the direct and indirect pathways finish in the thalamus, but their effects on the thalamus are very different. The direct pathway leaves the thalamus excited and active, while the indirect pathway causes the thalamus to be inhibited.
The thalamus will receive signals from the two pathways and then decide – based on those signals – whether to send an excitatory or inhibitory message to the cortex, telling it what to do (‘get excited and move’ or ‘don’t get excited and do not move’, respectively).
Where does dopamine come into the picture?
In Parkinson’s disease, we often talk about the loss of the dopamine neurons in the midbrain as a cardinal feature of the disease. When people are diagnosed with Parkinson’s disease, they have usually lost approximately 50-60% of the dopamine neurons in an area of the brain called the substantia nigra.
The dark pigmented dopamine neurons in the substantia nigra are reduced in the Parkinson’s disease brain (right). Source:Memorangapp
The midbrain is – as the label suggests – in the middle of the brain, just above the brainstem (see image below). The substantia nigra dopamine neurons reside there.
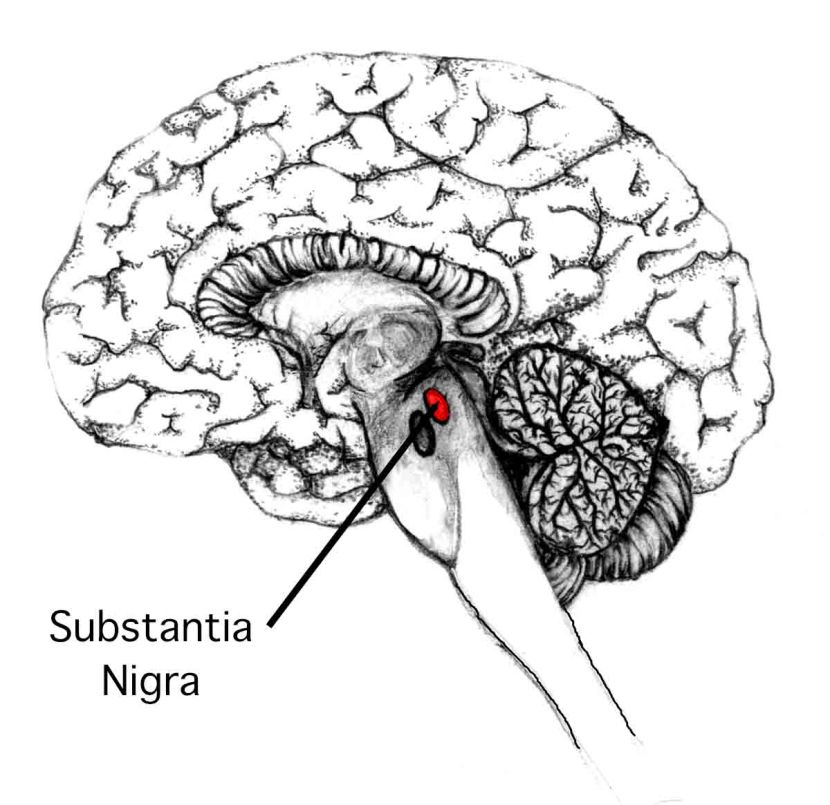
Location of the substantia nigra in the midbrain. Source: Memorylossonline
The dopamine neurons of the substantia nigra generate dopamine and release that chemical in different areas of the brain. The primary regions of that release are areas of the brain called the putamen and the Caudate nucleus. The dopamine neurons of the substantia nigra have long projections (or axons) that extend a long way across the brain to the putamen and caudate nucleus, so that dopamine can be released there.

The projections of the substantia nigra dopamine neurons. Source: MyBrainNotes
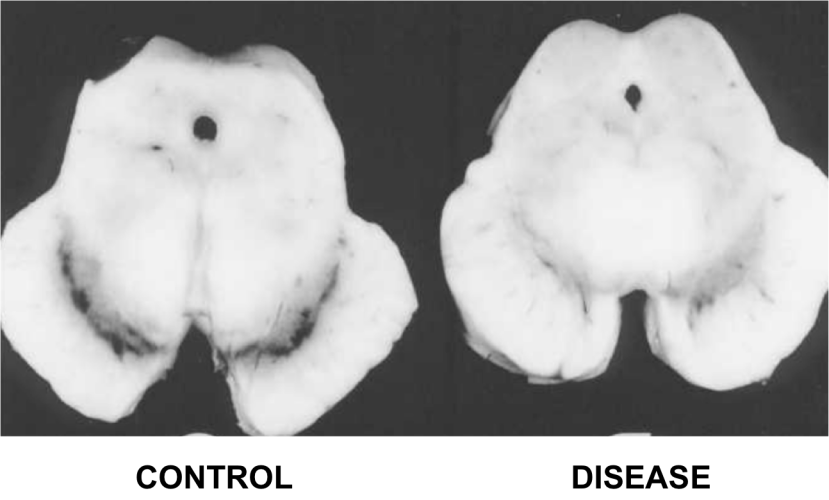
In Parkinson’s disease, these ‘axon’ extensions that project to the putamen and caudate nucleus gradually disappear as the dopamine neurons of the substantia nigra are lost. When one looks at brain sections of the putamen after the axons have been labelled with a dark staining technique, this reduction in axons is very apparent over time, especially when compared to a healthy control brain.

The putamen in Parkinson’s disease (across time). Source: Brain
EDITOR’S NOTE: I WOULD JUST LIKE TO ADD THAT THE IMAGE ABOVE IS NOT REPRESENTATIVE OF EVERYONE WITH PARKINSON’S. THE IMAGE IS BEING USED HERE TO PROVIDE AN EXAMPLE OF THE DOPAMINE FIBRE LOSS OBSERVED IN THE PUTAMEN. THIS PROCESS CAN TAKE LONGER IN SOME INDIVIDUALS THAN THE PERIOD OF TIME INDICATED.
Under normal circumstances the dopamine neurons release dopamine in the basal ganglia that excites the direct pathway and inhibits the indirect pathway. This acts as a kind of lubricant for movement.
With the loss of dopamine neurons in Parkinson’s disease, however, there is an increased amount of activity in the indirect pathway. As a result, the thalamus is kept inhibited. With the thalamus subdued, the overlying motor cortex has trouble getting excited, and thus the motor system is unable to work properly. And this is the reason why people with Parkinson’s disease have trouble initiating movement.
People with Parkinson’s disease will often be tested with a brain scan called a DAT-scan when they are diagnosed. This imaging technique results assesses the amount of dopamine being released in the putamen. It results in a horizontal image of the brain being presented on a computer screen with red (hot) regions that overlap with the location of the putamen in healthy individuals, indicating the normal release of dopamine. In people with Parkinson’s disease, however, there is a significant reduction in the release of dopamine (due to less dopamine neurons being present to generate dopamine), resulting in less red colouring on the computer screen image of the brain. In people with later stage Parkinson’s disease, there is even less colouring on the computer image (see image below).
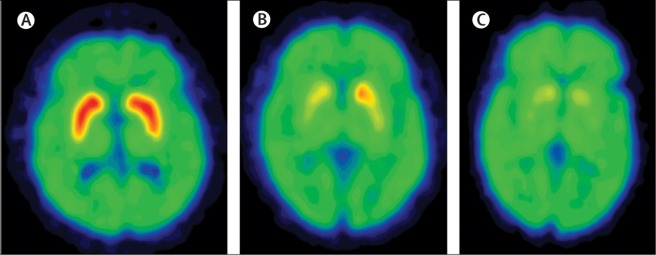
Dopamine transporter (DAT) in normal (A), early Parkinson’s (B) and late stage Parkinsons’ (C) brains. Source: Lancet
The banner for this page is sourced from Wikimedia

{kind=link}