
|
# # # # Novel treatments for Parkinson’s are being proposed on a regular basis, and I really like the way many are based on some pretty left field ideas (light buckets, I’m thinking of you here). Thinking outside the box is important to innovation and progress. And some of those unconventional approaches are backed not only by historical precedent, but also scientific research. Recently, researchers at Stanford University have presented just such an idea: It involves vibrating gloves. In today’s post, we will explore what research has been conducted on vibrating hands in Parkinson’s, and discuss what comes next. # # # # |
 Jean-Martin Charcot. Source: Wikipedia
Jean-Martin Charcot. Source: Wikipedia
There are few figures in the history of neurology as revered as Jean-Martin Charcot.
Widely considered the ‘Father of neurology’ and the ‘Napoleon of the neuroses‘, the importance of Charcot’s contribution to modern medicine is definitely not up for debate. One only needs to read the names of the students that he taught at the Salpêtrière Hospital (in Paris) to appreciate that everyone who became someone in the field of neurology passed through his classes.
Those names include Sigmund Freud (the founder of psychoanalysis), Joseph Babinski, Pierre Janet, Pierre Marie, Albert Londe, Charles-Joseph Bouchard, Georges Gilles de la Tourette (he of Tourette syndrome), Alfred Binet (inventor of the first intelligence test), and Albert Pitres.
The mere fact that these students of Charcot all have Wikipedia pages should speak volumes to his impact on the field. Heck, even the great William James – one of the founding fathers of Psychology – travelled all the way from America just to sit in on Charcot’s classes.
Charcot was one of the most sought-after instructors in all of Europe, and he is immortalised in a painting by André Brouillet:

“Une leçon clinique à la Salpêtrière“ by André Brouillet (Source: Wikipedia)
Cool. But what does monsieur Charcot have to do with Parkinson’s?
Oh, nothing.
Except that he is credited with naming the condition.
Between 1868 and 1881, Charcot focused much of his attention on the condition that would become “Parkinson’s disease”. He rejected the label that James Parkinson’s had given the condition (‘Paralysis Agitans’), suggesting that the former was misleading in that patients were not markedly weak and do not necessarily have tremor (Charcot, 1872). Rather than Paralysis Agitans, Charcot suggested that Maladie de Parkinson (or “Parkinson’s disease”) would be a more appropriate name, bestowing credit to the man who first described the condition.
Charcot was also one of the first doctors to propose an actual therapy for Parkinson’s.
It was called vibratory therapy, and it basically involved shaking the affected individual.

Vibratory therapy. Source: NCBI
I’m sorry – what?!? How was that considered a therapy?
Charcot had noticed that people with Parkinson’s experienced a reduction in their resting levels of tremor during and after taking a horse-pulled carriage ride. He speculated that the vibrations of the experience may have been the beneficial factor. A vibratory helmet which shook the head (and brain) was later developed, but again it is not clear how successful these first steps at a remedy were.
That sounds ridiculous. Why on Earth would vibrating someone work?
Well, vibration therapy may not actually be as ridiculous as it sounds and recently serious research has been conducted on this idea.
Que?!? What do you mean?
This is Prof Peter Tass:
 Source: Fz-juelich
Source: Fz-juelich
He is a Professor of Neurosurgery at Stanford University. His research area of interest is the development of neuromodulation techniques for understanding and treating neurologic conditions, like Parkinson’s.
And he has been exploring the idea of coordinated reset stimulation.
Coordinated what? Does this have anything to do with deep brain stimulation?
Not quite.
Deep brain stimulation (also known as DBS) is a method of treating Parkinson’s that involves the delivery of electrical charges to structures deep inside the brain, to help modulate the neural activity of that area. For example, the subthalamic nucleus is a region of the brain that becomes very excited in Parkinson’s, and the cells in that region start firing at an increased rate. This over activation of the structure results in dysfunction in other parts of the brain – ultimately disrupting normal movement.

Source: Ucdmc
Deep brain stimulation of this area involves electrodes being placed in the subthalamic nucleus and programming them to release tiny electrical pulses that will help regulate the firing of the surrounding cells. By modulating the firing of those cells, deep brain stimulation reduces the inhibition in the motor-related regions of the brain, which allows individuals with Parkinson’s to move more freely (Click here to read a previous SoPD post on the topic of DBS).
Coordinated reset stimulation, on the other hand, is taking a somewhat different approach.
Rather than trying to modulate brain activity, coordinated reset stimulation was developed to cause an “unlearning” of pathologically persistent activity, and it was hoped that this would allow for a therapeutic effect.
What does that mean? Unlearning?!?
Everyone has pre-existing neural pathways in their brains that help to deliver information to specialized structures. When we learn to ride a bike, neural pathways become specialized to that task as we learn how to do it. And the strength of the signaling of neurons influences the ultimate output activity.
But during the development of a condition like Parkinson’s, some of these pre-existing pathways will take on new activity as the brain tries to adapt to its changing circumstances. For example, the neural activity in the subthalamic nucleus (mentioned above) becomes more hyperactive.
These new patterns of activity could be considered “learned” at the level of the individual neuron.
Some of these newly acquired activities may not be very helpful though (again, think of the subthalamic nucleus gradually becoming more hyperactive in Parkinson’s, which slowly causes more inhibition in the motor regions of the brain). So a method of “un-learning” (at the level of the individual neuron) could be useful for treating the pathologically gained activity – shifting the state of the “learned” activity from pathological back to normal physiological levels.
 Source: Futuremedicine
Source: Futuremedicine
In this paradigm, coordinated reset stimulation seeks to desynchronize neural activity, causing an “un-learning” of the pathological activity. By disrupting the ‘learned’ (or synchronized) activity associated with pathological neural firing, there is the chance for a different (a less pathological and more normal physiological) state of neural activity to be initiated. Think of it as a resetting of the activity passing along some of the neural pathways in the brain.
Interesting. Does it work?
Back in 2012, Prof Tass and collaborators published this report supporting the idea in a primate model of Parkinson’s:
 Title: Coordinated reset has sustained aftereffects in Parkinsonian monkeys.
Title: Coordinated reset has sustained aftereffects in Parkinsonian monkeys.
Authors: Tass PA, Qin L, Hauptmann C, Dovero S, Bezard E, Boraud T, Meissner WG.
Journal: Ann Neurol. 2012 Nov;72(5):816-20.
PMID: 23280797
In this study, the researchers tested a deep brain stimulation therapy in non-human primates that had been given experimental Parkinson’s (via a neurotoxin). They employed a standard deep brain stimulation protocol (DBS), and they compared this with a coordinated reset stimulation pattern.
The result was very interesting.
They found that the standard DBS approach resulted in an immediate positive response, but as soon as they turned off the stimulation, the animals were once again inhibited in their movement.
With the coordinated reset stimulation, however, the researchers found that it resulted in both an immediate positive response equal to that of standard DBS, but curiously the effect of the coordinated reset stimulation lasted longer than standard DBS.
Much longer.
Even after they turned off the stimulation, the coordinated reset stimulation protocol resulted in maintained benefits to movement.
In fact, just 2 hours of per day the coordinated reset stimulation protocol for 5 consecutive days had resulted in a sustained aftereffects on motor function for up to 30 days after stimulation was stopped in these animals.
Wow! Has this been tested in humans?
Yes it has. This pilot study was conducted in 2014:
 Title: Coordinated reset neuromodulation for Parkinson’s disease: proof-of-concept study.
Title: Coordinated reset neuromodulation for Parkinson’s disease: proof-of-concept study.
Authors: Adamchic I, Hauptmann C, Barnikol UB, Pawelczyk N, Popovych O, Barnikol TT, Silchenko A, Volkmann J, Deuschl G, Meissner WG, Maarouf M, Sturm V, Freund HJ, Tass PA.
Journal: Mov Disord. 2014 Nov;29(13):1679-84.
PMID: 24976001 (This report is OPEN ACCESS if you would like to read it)
In this study, the investigators applied coordinated reset neuromodulation to the subthalamic nucleus of six individuals with Parkinson’s who had electrodes implanted as part of their deep brain stimulation treatment. All six of the participants responded well to coordinated reset neuromodulation, with an average 58% improvement in UPDRS motor scores by the end of the third day of stimulation.
And the effect was maintained after stimulation was terminated (into the evening of the third day at least).
Very interesting. So this coordinated reset stimulation stuff requires DBS?
So,… this is where the whole story takes a rather interesting turn.
What do you mean?
Well, Prof Tass and colleagues have found that they can replace electrical stimulation of the subthalamic nucleus (delivered through implanted electrodes) with weak vibration of the fingertips.
Wait. What?!?
Prof Tass and colleagues have developed mechanical stimulators mounted in the finger tips of gloves. And these enable the stimulation of specific areas of the brain without the need to implant electrodes:
 Source: Frontiers
Source: Frontiers
But how?!? How does that work?
To answer this question we need to understand what the somatosensory system is.
The somato… tomato-what?
The somatosensory system is the part of the brain and body that produces the perception of touch (as well as temperature, body position, and pain). In the human brain, the somatosensory cortex (which processes sensory information) is located just behind the motor cortex (which is involved with the initiation of most of our movement). In the image below, the somatosensory cortex is represented by the blue area, while the motor cortex is represented by the orange area:
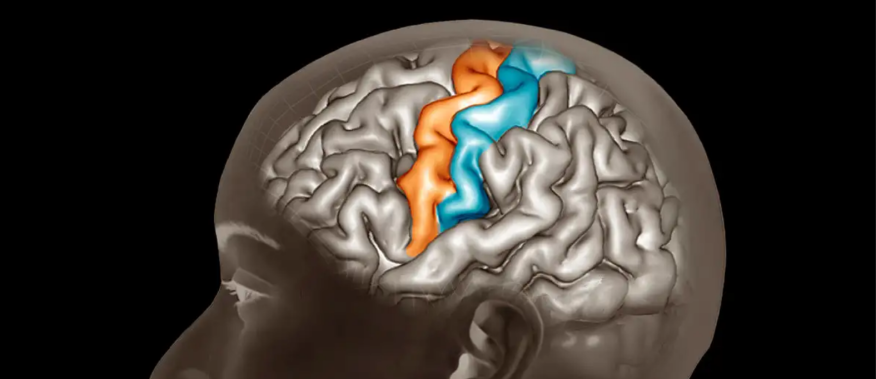 Source: Newscientist
Source: Newscientist
Somatosensory inputs are known to play a key role in cortical organization and skill acquisition. The somatosensory cortex is a very busy area of the brain when we learn new physical skills (like learning to ride a bike).
Ok, but what does this have to do with vibrating gloves?
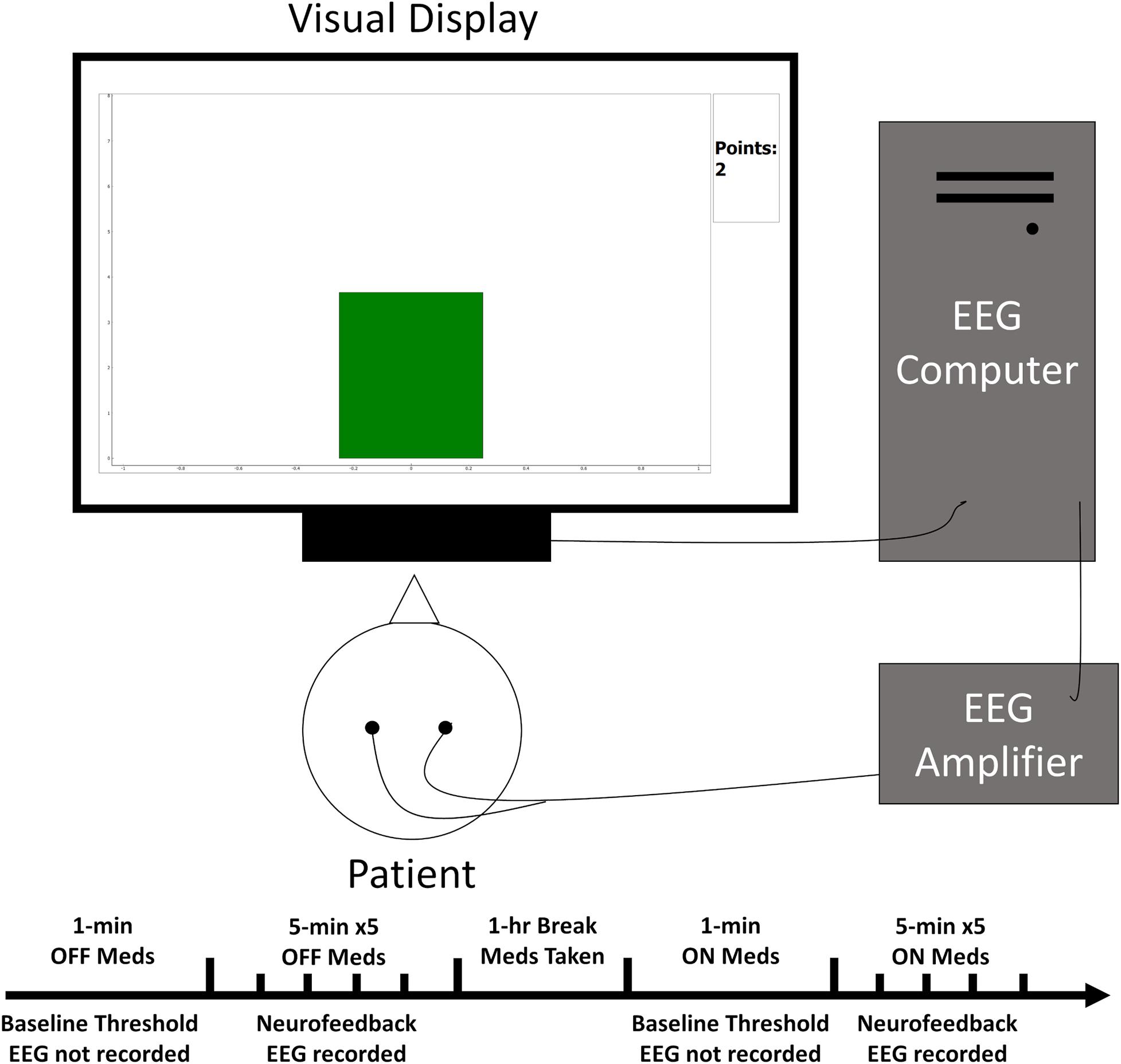
Well, researchers start by monitoring and monitor the synchronized activity of cortical neurons. They do this by placing electrodes to the top of people’s head and making recordings of the electroencephalographic (EEG) signals coming from their somatosensory cortex:
 Source: Frontiers
Source: Frontiers
Next they put the vibrating gloves on the fingers of the individual and start applying stimulation to the finger tips in the form of vibrations. The investigators can then monitor how the stimulation alters neural activity. Specific forms of this “vibrotactile coordinated reset” stimulation as it is called, can result in alterations to the neural activity being observed in the somatosensory cortex:
 Source: Stanford
Source: Stanford
And the researchers can alter the stimulation pattern of the finger tips so as to identify those that help to cause the coordinated reset (or unlearning) that we discussed above. They can compare those patterns with just “random noise” stimulation, which offers the possibility of a placebo like treatment for clinical trial situations.
Different research groups have also shown that vibrotactile stimulation can result in altered neuronal activity of the primary somatosensory cortex. For example, when vibration has been applied to the wrist it has been shown to increase neuronal activity in the sensorimotor cortex of resting individuals (Click here to read more about this). This result indicates that the vibratory stimulation treatment alone can cause activation of the sensorimotor cortex.
Ok, but how does changing activity in the somatosensory cortex (which processes sensory information) then change motor behaviour?
The researchers suggest that this stimulation-related activity in the somatosensory cortex may propagate across to the neighbouring motor areas via corticocortical connections. You will recall from the image above (and now directly below) that the somatosensory cortex is located just behind the motor cortex:
Source: Newscientist
Stimulation of the somatosensory cortex has been shown to result in responses from motor cortical neurons – this was first reported in 1994 (Click here to read more about this).
This all sounds amazing. But does it actually work?
Well, they have tested the gloves on individuals had Parkinson’s, and the results were very interesting.
In the first study, five people with idiopathic Parkinson’s received this finger tip-based vibration coordinated reset fingertip stimulation for 4 hours per day for 3 consecutive days. The participants were tested in terms of gait (walking) and bradykinesia (slowness of movement) before stimulation (on day 1), during stimulation (days 1‐3), and off‐treatment (day 3, 1 and 4 weeks after stimulation was completed – click here to read more about the details of this study).
The results were published in this report:
 Title: Coordinated reset vibrotactile stimulation shows prolonged improvement in Parkinson’s disease.
Title: Coordinated reset vibrotactile stimulation shows prolonged improvement in Parkinson’s disease.
Authors: Syrkin-Nikolau J, Neuville R, O’Day J, Anidi C, Miller Koop M, Martin T, Tass PA, Bronte-Stewart H.
Journal: Mov Disord. 2018 Jan;33(1):179-180.
PMID: 29150859 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers found that the finger tip vibration treatment was safe and well tolerated, but more importantly it resulted in both immediate “and cumulative improvements in quantitative measures of gait impairment and bradykinesia“.
That is to say, there was an improvement in walking and speed of movement both while the stimulation was on and when the stimulation was off (4 weeks after the treatment was stopped).
Sounds amazing. What did the researchers do next?
Next they conducted a set of longer feasibility studies, assessing the treatment in 3 individuals for more than 6 months, and 6 additional individuals for 3 months.
The results of those studies have also been published:
 Title: Coordinated Reset Vibrotactile Stimulation Induces Sustained Cumulative Benefits in Parkinson’s Disease.
Title: Coordinated Reset Vibrotactile Stimulation Induces Sustained Cumulative Benefits in Parkinson’s Disease.
Authors: Pfeifer KJ, Kromer JA, Cook AJ, Hornbeck T, Lim EA, Mortimer BJP, Fogarty AS, Han SS, Dhall R, Halpern CH, Tass PA.
Journal: Front Physiol. 2021 Apr 6;12:624317.
PMID: 33889086 (This report is OPEN ACCESS if you would like to read it)
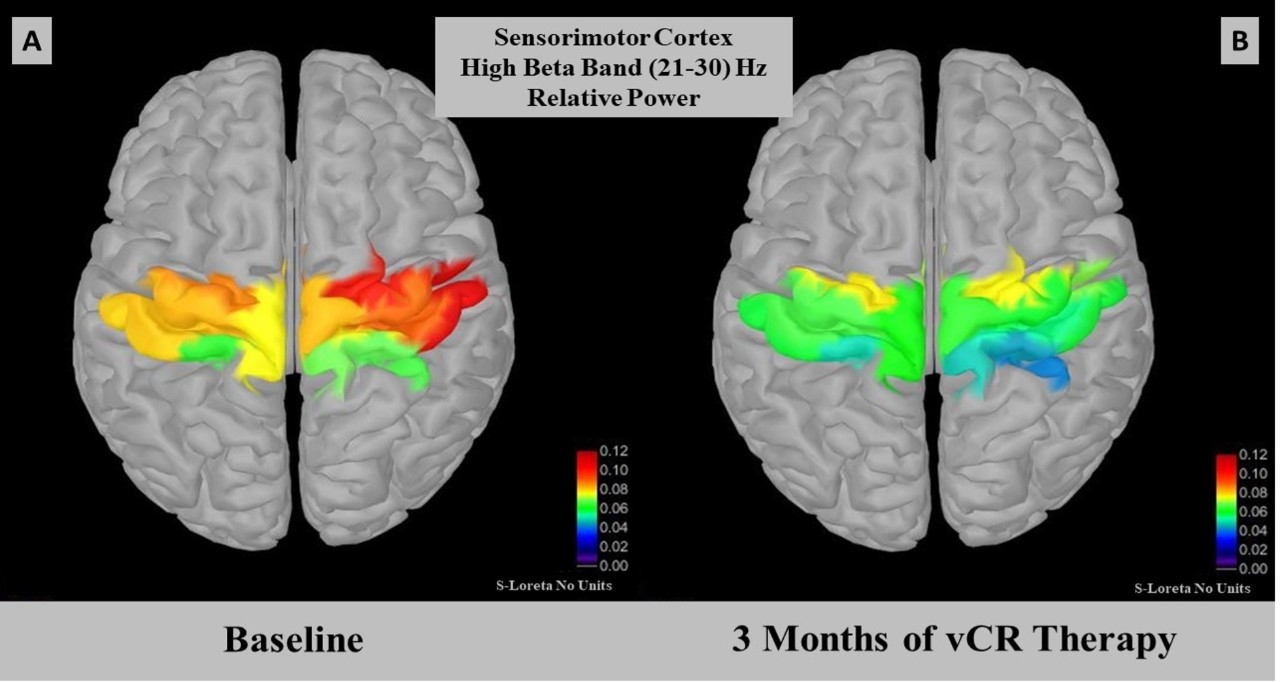
In this study, the researchers conducted two feasibility studies that examined the effect of two types of vibration coordinated reset fingertip stimulation through their gloves on Parkinson’s motor symptoms.
In both studies, the vibration coordinated reset fingertip stimulation treatments “were well tolerated, produced no side effects, and delivered sustained cumulative improvement of motor performance, which is congruent with our computational findings“. Interestingly, these studies also involved measuring the effects of the stimulation while the participants were on and off their Parkinson’s medications. With these encouraging results, the investigators are now hoping “to properly plan a proof-of-concept study“.
Where can I find out more information about this new technology?
On the 1st November (2022), Prof Tass gave this presentation at the Stanford 2022 Reunion’s President’s Welcome:
And for those readers looking for some hard science on all of this research (and a better explanation than my rant here), this video by Prof Tass provides a lot more detail:
Prof Michael Okun has also written a very good piece regarding this research on his website as well for those interested (Click here to read that).
What are the future plans for this research?
A biotech company called Synergic Medical Technology has been set up in Eugene, Oregon in 2019 to further develop this new technology.
![]() In 2021, the company registered a clinical trial to test the gloves in 36 people with Parkinson’s over 14 months (Click here to read more about this trial). That trial has subsequently been terminated, with a statement that “Stanford terminated the study with no reason given” attached to the clinical trial page (posted December 27, 2022).
In 2021, the company registered a clinical trial to test the gloves in 36 people with Parkinson’s over 14 months (Click here to read more about this trial). That trial has subsequently been terminated, with a statement that “Stanford terminated the study with no reason given” attached to the clinical trial page (posted December 27, 2022).
There is no information on the Synergic Medical Technologies website regarding this termination.
But three new clinical trials have been registered:
The first will involve 10 participants and evaluate the effects of Vibrotactile Coordinated Reset stimulation on early stage Parkinson’s symptoms. The primary endpoint of this study will be change in MDS-UPDRS III (motor) score from baseline to 24 months (Click here to read more about this study).
The second study will also involve 10 participants, and it will assess Vibrotactile Coordinated Reset as a treatment of advanced Parkinson’s. And again the primary endpoint of this study will be change in MDS-UPDRS III (motor) score from baseline to 24 months (Click here to read more about this study)
And the third study will involve 10 participants who are post surgical treatment (not DBS) for Parkinson’s, evaluating the effects of Vibrotactile Coordinated Reset stimulation on Parkinson’s symptoms, with the primary endpoint of this study will be change in MDS-UPDRS III (motor) score from baseline to 24 months (Click here to read more about this study).
There has been a lot of media attention focused on the “vibrating gloves”, such as:
And even Stanford University has posted videos, suggesting this new technology is a “game changer”:
And Stanford appears to have been exploring potential commercial deals for the technology. Back in late 2021, an article in the Stanford Medicine Magazine indicated that there were efforts afoot to find industry partners:
“For now, the glove treatment is available only to Parkinson’s patients participating in a clinical trial of the device that started Aug. 1. Tass is also working with an industry partner to gain U.S. Food and Drug Administration clearance for the treatment, which he hopes to have by summer 2023″. (Source)
And more recently (December 2022), a Forbes article suggested that Sergey Brin’s philanthropic team was “talking to a potential partner to help Tass get his invention to market faster” (Click here to read more on this).
What is your opinion on this research?
I have had a lot of requests for an opinion on this new technology. And long time readers will know that I am always very reluctant to give my personal thoughts on new research.
But if you put a gun to my head and demand it of me on this one occasion, my thoughts are these:
- I congratulate Prof Tass and colleagues for getting their research and this new technology to where it currently is. I can imagine that there has probably been some skepticism from the established deep brain stimulation community and bringing a novel idea like this to the clinic would have been a tremendous challenge. They have done well.
- I am also pleased to see some members of the Parkinson’s community reporting benefits from using the device. Readers should be made aware, however, that there are only a very small number of people who have actually tried the device. If they have experienced improvements then that could be good news for the wider Parkinson’s community, but more testing of it in much larger cohorts is required before we can make any real conclusions.
- Independent replication is required. If you do a Pubmed search for “Coordinated Reset Stimulation“, Prof Tass and his team are involved with 24 of the 30 papers listed – and most of the others involved modelling or reviews rather than actual experimentation. It would be useful to get independent replication of the vibration coordinated reset fingertip stimulation treatment on Parkinson’s symptoms. There are a number of other devices commercially available, but the research supporting them is extremely limited – and any claims beyond symptomatic benefit should be treated with caution. We need to see large carefully controlled clinical trials, rather than testimonials, which brings me to:
- The media needs to be really careful with their management of expectation. New technologies and research discoveries are exciting, but everyone gets tired of phrases like “game changer” and “breakthrough“. Until a new treatment is carefully and thoroughly tested and adopted, such language is not helpful and should not be part of the conversation.
- A lot more research is needed. The effects reported so far are from a very small cohort of individuals and limited to motor symptoms. I would be very curious to know what is happening with other symptoms (such as non-motor features like sleep) – are there any benefits there?
So what does it all mean?
Therapeutic rewiring of the brain is an appealing idea for treating neurodegenerative conditions like Parkinson’s. And there have been attempts at stimulating it via the use of neurotrophic proteins like GDNF (Click here to read more about this). Inducing a state of “unlearning” through stimulation is a novel concept in this area. It is amazing to consider that we could unlearn symptoms by manipulating the firing of neurons – particularly if this can be achieved via non invasive approaches like peripheral stimulation.
I am drawn towards left field, out-of-the-box ideas (heck, the wackier the better) as long as they are supported by historical precedent and hard research (that can be independently replicated). It is only through the exploration of new territory and experimentation with new ideas that we truly progress. Everything else is iterative and more evolution than real advancement.
I look forward to following the next steps in the development of Prof Tass’ vibration coordinated reset fingertip stimulation treatment, and I hope that it will encourage others to test their own unconventional ideas.
Here’s to the unorthodox or independent-minded mavericks.
ADDENDUM #1: 4th January 2023
Synergic Medical Technologies (the company developing this glove-based technology) announced today that they have received of a “Breakthrough Device Designation” from the US Food and Drug Administration for their VT Touch vibrotactile stimulation gloves
for treating pathological beta oscillations in Parkinson’s.
The company also stated that they are “working with a university medical center to start a randomized clinical trial to test the effectiveness of the VT Touch glove with Parkinson’s patients. We hope to report on progress with this clinical trial in the near future” (Click here to read more about this).
ADDENDUM #2: 15th March 2023
Sharon Krischer has posted the following video on Youtube, where Prof Tass provides another great overview of this new research:
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
EDITOR’S NOTE: The author of this post is an employee of Cure Parkinson’s, so he might be a little bit biased in his views on research and clinical trials supported by the trust. That said, the trust has not requested the production of this post, and the author is sharing it simply because it may be of interest to the Parkinson’s community.
The information provided by the SoPD website is for information and educational purposes only. Under no circumstances should it ever be considered medical or actionable advice. It is provided by research scientists, not medical practitioners. Any actions taken – based on what has been read on the website – are the sole responsibility of the reader. Any actions being contemplated by readers should firstly be discussed with a qualified healthcare professional who is aware of your medical history. While some of the information discussed in this post may cause concern, please speak with your medical physician before attempting any change in an existing treatment regime.
In addition, many of the companies mentioned in this post are publicly traded companies. That said, the material presented on this page should under no circumstances be considered financial advice. Any actions taken by the reader based on reading this material is the sole responsibility of the reader. None of the companies have requested that this material be produced, nor has the author had any contact with any of the companies or associated parties. This post has been produced for educational purposes only.
The banner for today’s post was sourced from Stanmed and the clevelandclinic.

Very interesting. On occasion at 2.45, 3.15, 4.18 or whatever in the morning and I can’t get back to sleep because my leg is in tremor mode, I am driven to shake or perhaps shiver my leg deliberately and as forcefully as I can. Sort of like the forced shivering that comes after swimming in cold water. Sometimes, when I stop, the relaxation is sufficient to give me enough peace to drop off to sleep.
LikeLike
For a successful DIY implementation goto youtube search for pdbuzzboard: https://www.youtube.com/watch?v=1PfsVjnPAuQ
Regards
Viele Grüße Arnd
LikeLike
There is now also a DIY glove version from the same person: https://www.youtube.com/watch?v=Otokrrb2WSU
LikeLike