|
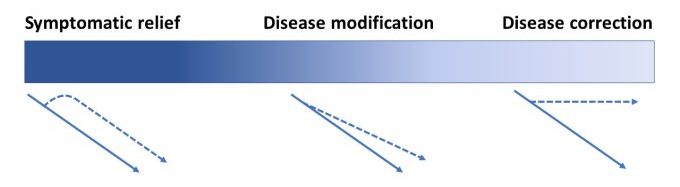
# # # # Semantics matters – particularly regarding our communication on ideas like “disease modification” for neurodegenerative conditions. There is a big difference between “disease eradication” (zero worldwide incidence), “disease correction” (the halting/reversing of progression) and “disease modification” (improving the trajectory of disease). Recently, researchers in Japan have demonstrated “disease modification” in motor neuron disease with a form of vitamin B12. In today’s post, we will review this new research and discuss how it could be relevant to Parkinson’s. # # # # |
 Source: LexFridman
Source: LexFridman
During labourious household chores (think: washing the dishes, hanging laundry, or spending time with my daughter), I am usually listening to an audiobook or podcast. One favourite podcast is that of Dr Lex Fridman – an AI researchers at MIT who interviews interesting individuals and discusses a broad range of topics (from neuroscience to weird stuff like aliens, and the meaning of life often gets dragged in as well).
In episode #158, Lex spoke with Zev Weinstein (15 year old son of Prof Eric Weinstein) and I was really struck with how eloquently this young man spoke about philosophy and science, but also the communication of ideas.
 Source: Youtube
Source: Youtube
And at one point in the discussion, Zev said: “Many underestimate the extent to which language and communication really impacts and shapes the ideas and thoughts that are being communicated, and I think if we are willing to accept imperfect labels to categorize particular people or thoughts, in some sense we are corrupting an abstraction in order to represent it and communicate about it. And I think, as we have discussed, those abstractions are particularly important when everything is on fire” – Zev Weinstein (18.03 minutes into the video). The interview occurred in early 2021 around the events of 6th January, hence the “everything on fire” reference.
But the words on “corrupting an abstraction in order to represent it and communicate about it” resonated with me.
And it got me thinking.
Thinking about what?
By night (when time allows), I maintain this website. But during the day, I am the director of research at a medical research charity called Cure Parkinson’s.
![]()
As an organisation, we are extremely focused. We have a very narrow remit in terms of the type of research we support. Cure Parkinson’s only funds Parkinson’s research that is of a disease-modifying nature. We do not consider basic science or research into symptomatic treatments. We are squarely focused on curative therapies.
And Zev’s comments above got me thinking about some of these words (“curative” and “disease modifying“) and what they actually mean when we use them.
So I started asking myself: What do we really mean by the word “cure”?
It is an emotive word for many. It carries a lot of hope and heightens expectations, and thus needs to be handled with care.
But does “cure” refer to the actual eradication of a disease? If so, that suggests a preventative approach. How does this relate to those already diagnosed and living with the condition?
To be fair, for all our amazing medical progress over the last century (which now involves the editing of DNA and the production of vaccines within months of sequencing novel viruses), humanity has actually only eradicated two diseases (smallpox in humans, and rinderpest in ruminants (that is, hoofed herbivorous grazing mammals)). And both of these were well understood conditions caused by viral infections. There are tremendous efforts focused on other global diseases like polio and malaria, but both are some way from complete eradication (reduction to zero).
Eradication of Parkinson’s would suggest preventing it from ever occurring – a noble goal. And major projects are now underway in identifying those individuals at risk of potentially developing the condition (such as the PPMI-2 project being run by the Michael J Fox Foundation).

But if eradication of a disease before it is diagnosed remains challenging, then what does a ‘cure‘ mean for those in the community already diagnosed? Already dealing with the day-to-day, moment-to-moment trials of the condition?
Does it mean a return to some abstract point in time, ability and well being before PD? If so, are we actually looking for some kind of fountain of youth?
These are some of the thoughts that were bouncing around in my noggin after listening to Zev’s “corrupting an abstraction” comment.
With regards to my employer, the name was originally aspirational. It is a goal, but initially the co-founders were simply wanting to see more research focused on actually changing the course of the disease – which at the time was arguably lacking.
Cure Parkinson’s was started in 2005 by four gentlemen who were frustrated by the lack of research actually focused on actually curing the condition that they shared. They did not want better care or more research into better symptomatic treatments (which was all they could see at the time). They wanted a more concerted effort focused on remedies that would stop the progression of their debilitating situation and possibly improve things.
 The co-founders of Cure Parkinson’s (and their amazing wives)
The co-founders of Cure Parkinson’s (and their amazing wives)
And so they started Cure Parkinson’s and over the last 15+ years, the organisation has continuously championed research focused on finding anything that will slow, stop or reverse Parkinson’s. From GDNF and UDCA to exenatide and ambroxol – they have been a driving force for disease modifying therapies for Parkinson’s.
But even here we run into semantics.
What do we mean by “disease modifying therapies“?
If a treatment simply makes someone healthier and slows down the progression of their chronic condition as a consequence of that improvement in health, could this be defined as ‘disease modifying‘ or ‘curative‘? Particularly if we don’t even know how it may be having its effect?
What do you mean?
Let’s look at an example. We’ll use vitamin B12 :
 Source: Peacefuldumpling
Source: Peacefuldumpling
Vitamin B12 is one of eight B vitamins, and there are four different forms (or vitamers) of B12 :
- Adenosylcobalamin (AdoCbl) – one of the enzymatically active form
- Methylcobalamin (also known as cobalamin) – the other enzymatically active form
- Hydroxycobalamin – not normally present in the human body
- Cyanocobalamin – does not normally occur in nature
vitamin B12 is essential for human life, but we do not produce it ourselves. It must come from our diet, where it is found in animal products, such as meat, dairy and eggs. Adults need around 2.4 micrograms (mcg) of vitamin B12 a day.
It is essential for making red blood cells, the correct functioning of nerves (in the synthesis of myelin), and it is a cofactor in DNA synthesis. To show you how essential vitamin B12 is – five people have been awarded Nobel Prizes for direct and indirect studies related to vitamin B12: George Whipple, George Minot and William Murphy (1934), Alexander R. Todd (1957), and Dorothy Hodgkin (1964).
Ok, so why is vitamin B12 being used as an example here?
Well, earlier this year researchers in Japan published this report:
 Title: Efficacy and Safety of Ultrahigh-Dose Methylcobalamin in Early-Stage Amyotrophic Lateral Sclerosis: A Randomized Clinical Trial.
Title: Efficacy and Safety of Ultrahigh-Dose Methylcobalamin in Early-Stage Amyotrophic Lateral Sclerosis: A Randomized Clinical Trial.
Authors: Oki R, Izumi Y, Fujita K, Miyamoto R, Nodera H, Sato Y,… a lot of additional researchers…, Kuwabara S, Kaji R; Japan Early-Stage Trial of Ultrahigh-Dose Methylcobalamin for ALS (JETALS) Collaborators.
Journal: JAMA Neurol. 2022 May 9. Online ahead of print.
PMID: 35532908
In this study, the investigators conducted a multicenter, placebo-controlled, double-blind, randomized Phase 3 clinical trial evaluating the efficacy and safety of an ultrahigh-dose form of vitamin B12 (methylcobalamin) in 130 people who were less than one year into a diagnosis of ALS.
What is ALS?
Also known as Lou Gehrig’s disease or motor neuron disease, amyotrophic lateral sclerosis (or ALS) is a neurodegenerative condition in which the neurons that control voluntary muscle movement die. The condition affects 2 people in every 100,000 each year, and once diagnosed those individuals have an average survival time of two to four years, but many pass away within 12 months. It is a terribly cruel disease.
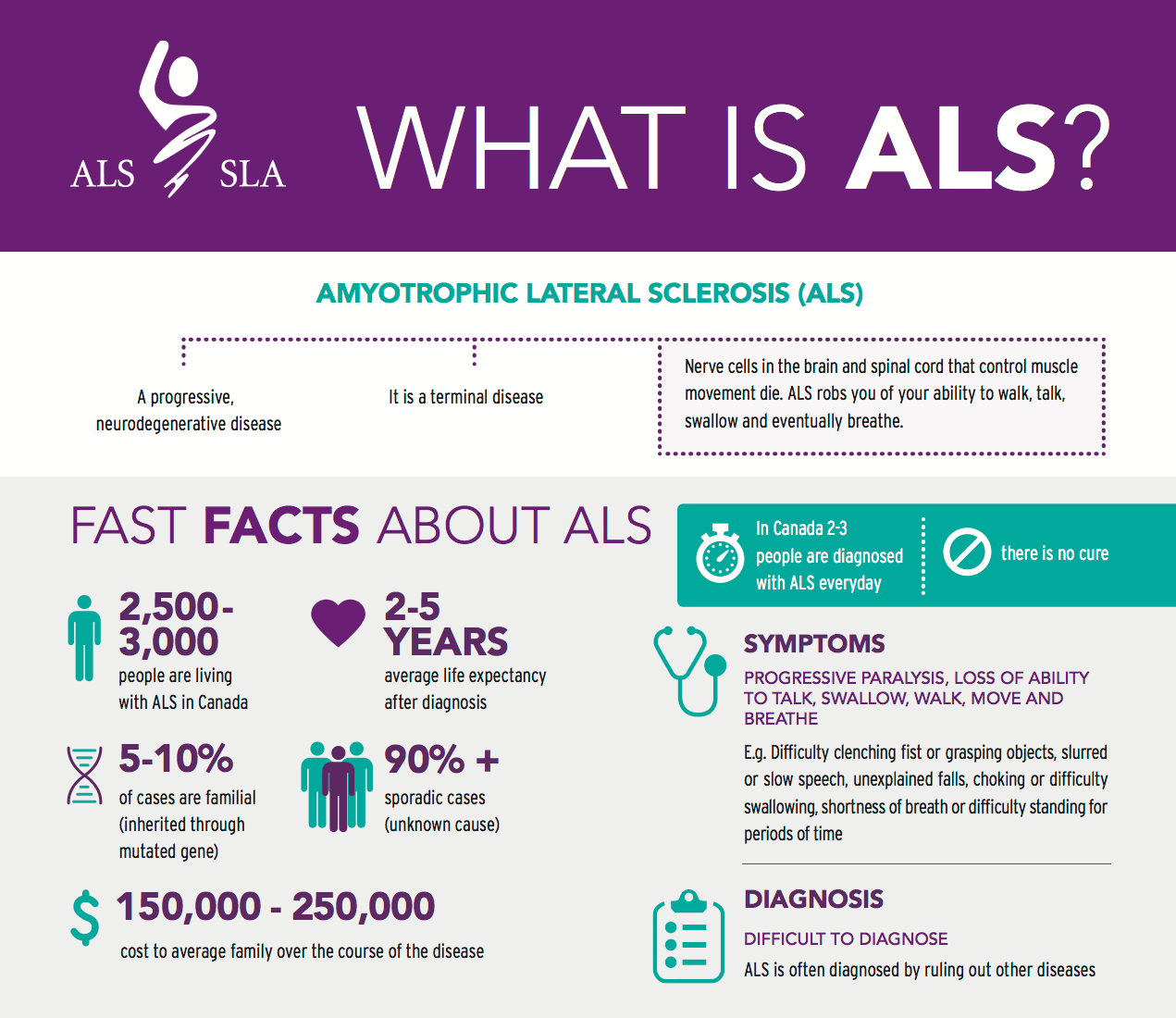 ALS in a nutshell. Source: Walkforals
ALS in a nutshell. Source: Walkforals
The cause of ALS is unknown, but the condition is characterised by the gradual degeneration and loss of motor neurons. Motor neurons are neurons that are involved with instructing the muscles of our body.
The loss of motor neurons in ALS causes a loss of muscle control. There are three stages to ALS (Source):
- A gradual development of muscle weakness, tightness, cramping, or twitching. This stage is also associated with muscle loss (or atrophy).
- Muscle weakness and atrophy progresses towards paralysis.
- Most voluntary muscle activity is lost and the sufferer becomes paralyzed. With this stage eating, speaking, and breathing become compromised.
Dementia is not a common feature of the condition, and as a result most individuals affected by ALS retain their higher cognitive abilities and are fully aware of their progressive loss of muscular function.
Ok. So what did they find in their clinical trial?
The study started out with a 12-week observation period and then participants were randomly assigned to 16-week treatment phase where they were treated with twice weekly intramuscular injections of either ultrahigh-dose methylcobalamin or placebo. There were 65 participants in the treatment group and 64 in the placebo arm. After the 16 week treatment period, everyone in the study was offered an open label extension in which everyone was treated with just ultrahigh-dose methylcobalamin (a form of vitamin B12).
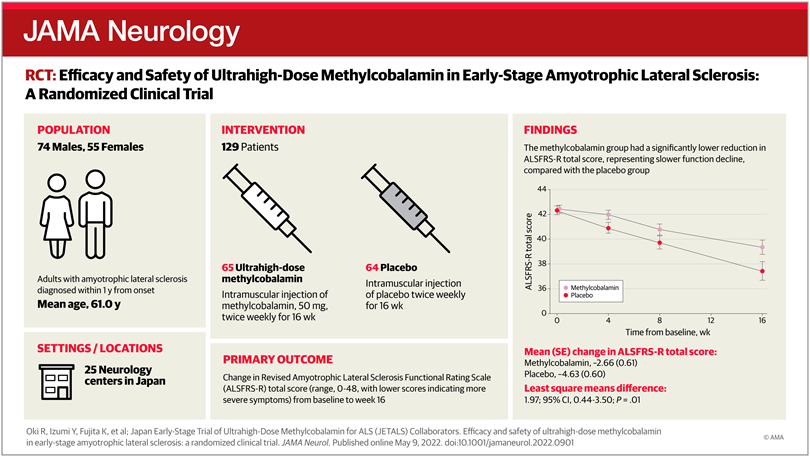
The primary end point of the study (this is the pre-designated measure of efficacy) was the amount of change in the Revised Amyotrophic Lateral Sclerosis Functional Rating Scale (or ALSFRS-R) total score between the start of the treatment phase (baseline) and the end of the treatment phase (week 16). The ALSFRS-R is a clinical rating scale – akin to the MDS-UPDRS used in Parkinson’s research – that measures 12 aspects of physical function, ranging from one’s ability to swallow and use utensils to climbing stairs and breathing. It has a highest score of 48 and a minimum of 0.
After 16 weeks of treatment with either ultrahigh-dose methylcobalamin or placebo, the researchers found a clear and statistically significant difference between the two groups: the ultrahigh-dose methylcobalamin treated group was significantly slower in their progression than the placebo treated group. Almost 2 points better on average:
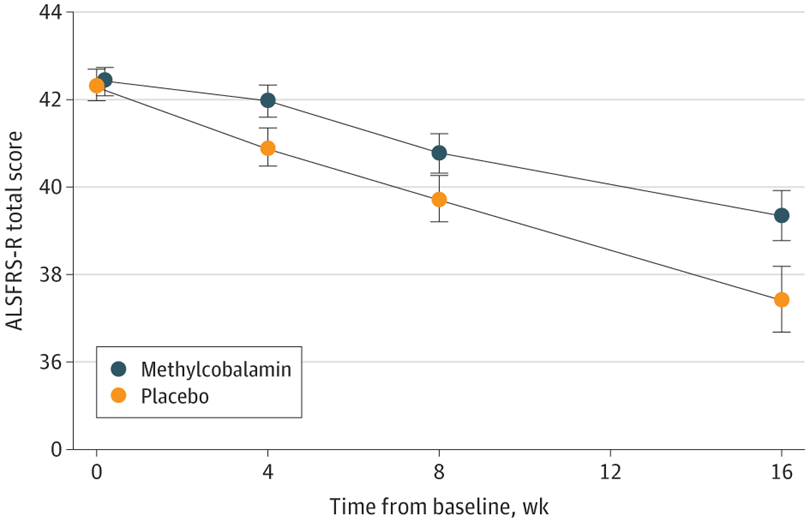
Two points might not sound like a lot, but that shift in trajectory is adding weeks or months to otherwise shortened lives. It’s a big deal to the ALS community.
And this result supported the post hoc findings of a previous trial, which found no difference between ultrahigh-dose methylcobalamin and placebo, but when the investigators had dug deep into the data they found that recently diagnosed individuals did significantly better on ultrahigh-dose methylcobalamin than placebo (Click here to read more about this).
The result of the new Phase 3 study are very exciting news for the ALS community, for whom there are few medical options. And the Japanese pharmaceutical company Eisai – who make this ultrahigh-dose methylcobalamin product and supported the study – are now taking their product to the Japanese medical regulators seeking approval for its clinical use in ALS (Click here to read more about this).
![]()
Interesting, but how is the ultrahigh-dose methylcobalamin product working?
In the write-up of the results, the investigators admit that while the effect is significant, they can only speculate as to the potential mechanism of action that could be driving the positive effect (they speculate on the homocysteine lowering properties of methylcobalamin).
What is homocysteine?
Homocysteine is one of the amino acids that our bodies use to make proteins. Normally, homocysteine levels are low, but high amounts of homocysteine can cause excitotoxicity, oxidative stress, mitochondrial dysfunction, and inflammation.
Vitamin B12 is involved in breaking down homocysteine, so the investigators were wondering if by increasing levels of methylcobalamin they were reducing oxidative stress, mitochondrial dysfunction, inflammation, etc.
Regardless, the treatment appears to be having a beneficial effect and potentially increasing survival time.
But here I come back to the discussion at the top of this post: Is this “disease modification“?
Does it matter? If the patients are surviving longer, do definitions or labels really matter?
It’s a fair point, but I think definitions do matter.
I have worried for a while now that we have recently been lowering the bar for a lot of new therapies coming through for neurodegenerative conditions (yes, I’m looking at you Arukiddingmab).
Perhaps a treatment like high dose vitamin B12 is simply giving people’s body a better footing upon which to fight the disease afflicting it. But I’m not sure this should be called “disease modification“.
Rather than disease modification, maybe it’s just being healthier.
Perhaps we need a broader and better defined set of alternative words to define different stages and goals? Such as response, remission and recovery as they have in oncology.
Response could refer to a partial but sustained reduction/improvement in symptom progression after treatment. Not a temporary symptomatic response as such (like that provided by Levodopa), but a maintained improvement that shifts the needle. The vitamin B12 result in the ALS study above would possibly fall into this response definition.
Has anyone ever looked at Vitamin B12 in Parkinson’s before?
It is important here to appreciate that low B12 levels is rather common, affecting 10% to 20% of people over the age of 60 years (Click here and here to read more about this).
But yes, some associations between Parkinson’s and vitamin B12 have been made. In fact, a meta-analysis of previously published research on this topic was made available a couple of years ago:
 Title: Associations between B Vitamins and Parkinson’s Disease
Title: Associations between B Vitamins and Parkinson’s Disease
Author: Shen L.
Journal: Nutrients. 2015 Aug 27;7(9):7197-208.
PMID: 26343714 (This report is OPEN ACCESS if you would like to read it)
In this study, the investigator pooled data from 10 previous reports and found that people with Parkinson’s on average have lower level of vitamin B12 than control participants. This study also reported that higher dietary intake of vitamin B6 may be associated with a reduced risk of developing Parkinson’s (we will come back to this in a future post).
More recently, further evidence of lower levels of vitamin B12 in recently diagnosed cases of Parkinson’s has been published:
 Title: Vitamin B12 and Homocysteine Levels Predict Different Outcomes in Early Parkinson’s Disease.
Title: Vitamin B12 and Homocysteine Levels Predict Different Outcomes in Early Parkinson’s Disease.
Authors: Christine CW, Auinger P, Joslin A, Yelpaala Y, Green R; Parkinson Study Group-DATATOP Investigators.
Journal: Mov Disord. 2018 May;33(5):762-770.
PMID: 29508904
In this study, the researchers measured vitamin B12 in 680 baseline serum samples and then again in 456 follow-up serum samples several years later. Serum is the liquid component of blood when the cells and clotting factors are removed. The serum was collected from individuals with recently diagnosed untreated Parkinson’s (who were taking part in the DATATOP study).
DATATOP was a double-blind, randomised trial that was set up to test whether treatment with deprenyl (selegiline hydrochloride) and/or the antioxidant, a-tocopherol could slow down Parkinson’s progression. 800 participants were recruited between 1987 and 1988. The study failed to demonstrate any beneficial effects, but as you can see the data collected from this huge study is still generating interesting findings 20+ years on.
At the baseline sampling, 13% of the participants had low B12 levels, and at the follow up assessment the investigators found that those low B12 levels were associated with greater worsening of mobility (the average time between baseline and the follow up was 17 months), when compared to participants with normal low B12 levels.
Interestingly, although the numbers were small and the differences were not significant, there were trends for slower progression (smaller annualised UPDRS changes) in those participants involved in the study whose B12 status improved over the course of the study.
So perhaps there is a case to be made for testing Eisai’s ultrahigh-dose methylcobalamin product in Parkinson’s?
Has Vitamin B12 ever been tested in clinical trials?
There was one study 10 years ago at Emory University that explored vitamin B12 status and response to vitamin B12 supplementation in people with Parkinson’s, but that trial was terminated and I am not aware of any results being put in the public domain (Click here to read more about this trial).
Beyond that I am unaware of any clinical trials of vitamin B12 in Parkinson’s (happy to be corrected on this).
How can I get me some Vitamin B12?
Vitamin B12 is considered to be very safe.
It is naturally found in animal products (such as fish, meat, poultry, eggs, milk, and milk products) and generally not in plant foods.
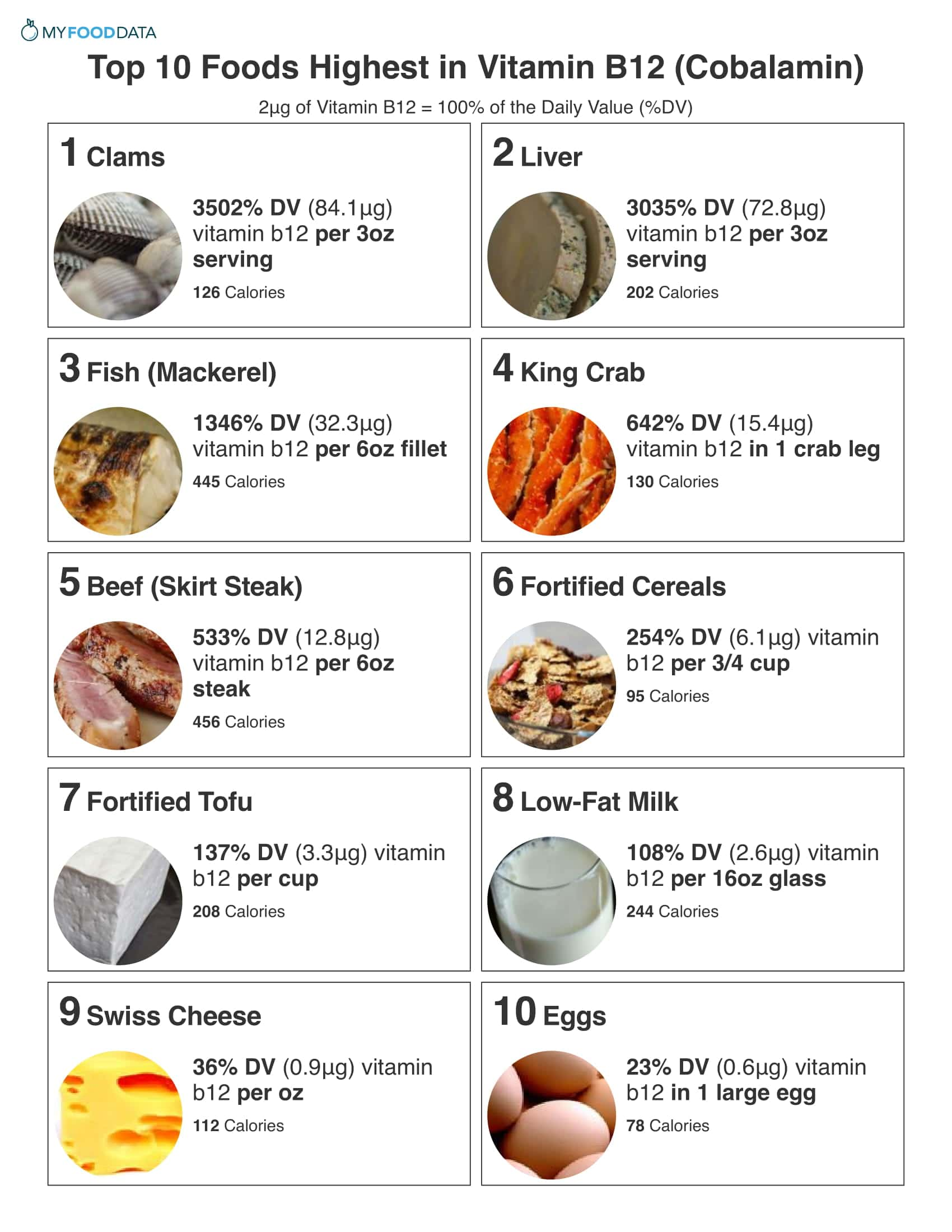 Source: Myfooddata
Source: Myfooddata
So what does it all mean?
Some readers may be frustrated by a fuss over semantics, but the need for this discussion is important. Humans love to game systems (particularly for profit) and I worry that “corrupting an abstraction” is all too easy for ones own ends. Long time readers will be aware that endgame scenarios for “disease modification” in neurodegenerative conditions keep me awake at night (Click here for a previous SoPD post on this topic), and I am regularly coming back to this topic.
All of this said, I am intrigued by the vitamin B12 data. ALS is a dreadful, extremely aggressive condition, and I applaud the achievement of the Japanese researchers. I am particularly excited for them that they are now in potentially in a position to have ultrahigh-dose methylcobalamin as a ‘standard of care’ treatment and they can start exploring combinations of therapies to see if they can achieve additional synergistic benefits.
Perhaps multiple treatments that offer a ‘response’, could lead to a state of ‘remission’ or disease correction? Only time will tell. Fingers crossed for them.
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
EDITOR’S NOTE: The author of this post is an employee of Cure Parkinson’s, so he might be a little bit biased in his views on research and clinical trials supported by the trust. That said, the trust has not requested the production of this post, and the author is sharing it simply because it may be of interest to the Parkinson’s community.
The information provided by the SoPD website is for information and educational purposes only. Under no circumstances should it ever be considered medical or actionable advice. It is provided by research scientists, not medical practitioners. Any actions taken – based on what has been read on the website – are the sole responsibility of the reader. Any actions being contemplated by readers should firstly be discussed with a qualified healthcare professional who is aware of your medical history. While some of the information discussed in this post may cause concern, please speak with your medical physician before attempting any change in an existing treatment regime.
In addition, many of the companies mentioned in this post are publicly traded companies. That said, the material presented on this page should under no circumstances be considered financial advice. Any actions taken by the reader based on reading this material is the sole responsibility of the reader. None of the companies have requested that this material be produced, nor has the author had any contact with any of the companies or associated parties. This post has been produced for educational purposes only.
The banner for today’s post was sourced from Youtube

Next steps: Mayo Clinic researchers are working on a retrospective study to look for a connection between vitamin B12 deficiency and postural instability and cognitive impairment. They plan to complete this study by the end of 2019.
LikeLike