The Federal Drug Administration (FDA) in the USA has approved the first drug in 22 years for treating the neurodegenerative condition of Amyotrophic lateral sclerosis (ALS).
The drug is called Edaravone, and it is only the second drug approved for ALS.
In today’s post we’ll discuss what this announcement could mean for Parkinson’s disease.

Lou Gehrig. Source: NBC
In 1969, Henry Louis “Lou” Gehrig was voted the greatest first baseman of all time by the Baseball Writers’ Association. He played 17 seasons with the New York Yankees, having signed with his hometown team in 1923.
For 56 years, he held the record for the most consecutive games played (2,130), and he was only prevented from continuing that streak when he voluntarily took himself out of the team lineup on the 2nd May, 1939, after his ability to play became hampered by the disease that now often bears his name. A little more than a month later he retired, and a little less than two years later he passed away.
Amyotrophic lateral sclerosis (or ALS), also known as Lou Gehrig’s disease and motor neuron disease, is a neurodegenerative condition in which the neurons that control voluntary muscle movement die. The condition affects 2 people in every 100,000 each year, and those individuals have an average survival time of two to four years.

ALS in a nutshell. Source: Walkforals
In addition to Lou Gehrig, you may have heard of ALS via the ‘Ice bucket challenge‘ (see image in the banner of this post). In August 2014, an online video challenge went viral.
By July 2015, the ice bucket campaign had raised an amazing $115 million for the ALS Association.
Another reason you may have heard of ALS is that theoretical physicist, Prof Stephen Hawking also has the condition:

Source: BBC
He was diagnosed with in a very rare early-onset, slow-progressing form of ALS in 1963 (at age 21) that has gradually left him wheel chair bound.
This is very interesting, but what does it have to do with Parkinson’s disease?
Individuals affected by ALS are generally treated with a drug called Riluzole (brand names Rilutek or Teglutik). Approved in December of 1995 by the FDA, this drug increases survival by approximately two to three months.
Until this last week, Riluzole was the only drug approved for the treatment of ALS.
So what happened this week?
On the 5th May, the FDA announced that they had approved a second drug for the treatment of ALS (Click here for the press release).
It is called Edaravone.
What is Edaravone?
Edaravone is a free radical scavenger – a potent antioxidant – that is marketed as a neurovascular protective agent in Japan by Mitsubishi Tanabe Pharma Corporation.
An antioxidant is simply a molecule that prevents the oxidation of other molecules.
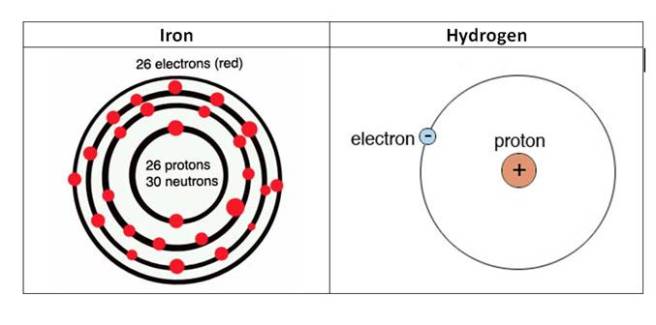
Molecules in your body often go through a process called oxidation – losing an electron and becoming unstable. This chemical reaction leads to the production of what we call free radicals, which can then go on to damage cells.
What is a free radical?
A free radical is simply an unstable molecule – unstable because they are missing electrons. They react quickly with other molecules, trying to capture the needed electron to re-gain stability. Free radicals will literally attack the nearest stable molecule, stealing an electron. This leads to the “attacked” molecule becoming a free radical itself, and thus a chain reaction is started. Inside a living cell this can cause terrible damage, ultimately killing the cell.
Antioxidants are thus the good guys in this situation. They are molecules that neutralize free radicals by donating one of their own electrons. The antioxidant don’t become free radicals by donating an electron because by their very nature they are stable with or without that extra electron.
Thus when we say ‘Edaravone is a free radical scavenger’, we mean it’s really good at scavenging all those unstable molecules and stabilising them.
It is an intravenous drug (injected into the body via a vein) and administrated for 14 days followed by 14 days drug holiday.
So, again what has this got to do with Parkinson’s disease?
Well, it is easier to start a clinical trial of a drug if it is already approved for another disease.
And the good news is: Edaravone has been shown to be neuroprotective in several models of Parkinson’s disease.
In this post, we’ll lay out some of the previous research and try to make an argument justifying the clinical testing of Edaravone in Parkinson’s disease
Ok, so what research has been done so far in models of Parkinson’s disease?
The first study to show neuroprotection in a model of Parkinson’s disease was published in 2008:

Title: Role of reactive nitrogen and reactive oxygen species against MPTP neurotoxicity in mice.
Authors: Yokoyama H, Takagi S, Watanabe Y, Kato H, Araki T.
Journal: J Neural Transm (Vienna). 2008 Jun;115(6):831-42.
PMID: 18235988
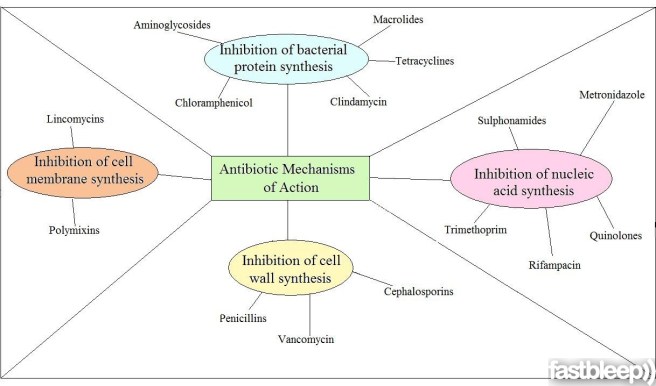
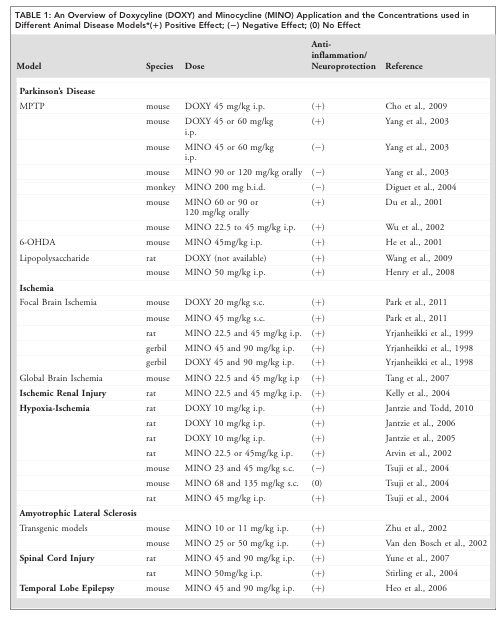
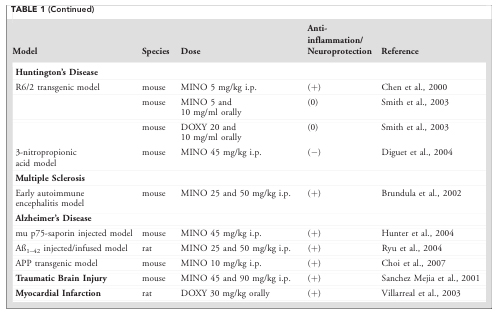
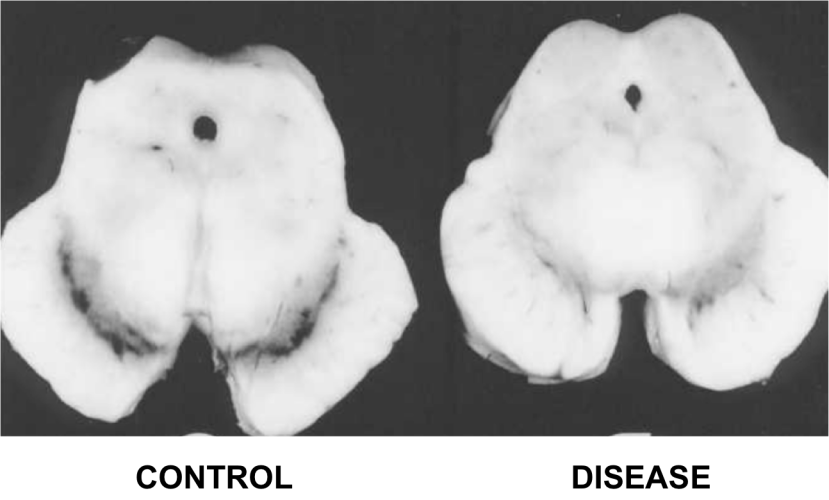
In this first study, the investigators assessed the neuroprotective properties of several drugs in a mouse model of Parkinson’s disease. The drugs included Edaravone (described above), minocycline (antibiotic discussed in a previous post), 7-nitroindazole (neuronal nitric oxide synthase inhibitor), fluvastatin and pitavastatin (both members of the statin drug class).
With regards to Edaravone, the news was not great: the investigators found that Edaravone (up to 30mg/kg) treatment 30 minutes before administering a neurotoxin (MPTP) and then again 90 minutes afterwards had no effect on the survival of the dopamine neurons (compared to a control treatment).
Not a good start for making a case for clinical trials!
This research report, however, was quickly followed by another from an independent group in Japan:

Title: Neuroprotective effects of edaravone-administration on 6-OHDA-treated dopaminergic neurons.
Authors: Yuan WJ, Yasuhara T, Shingo T, Muraoka K, Agari T, Kameda M, Uozumi T, Tajiri N, Morimoto T, Jing M, Baba T, Wang F, Leung H, Matsui T, Miyoshi Y, Date I.
Journal: BMC Neurosci. 2008 Aug 1;9:75.
PMID: 18671880 (This article is OPEN ACCESS if you would like to read it)
These researchers did find a neuroprotective effect using Edaravone (both in cell culture and in a rodent model of Parkinson’s disease), but they used a much higher dose than the previous study (up to 250 mg/kg in this study). This increase in dose resulted in a graded increase in neuroprotection – interestingly, these researchers also found that 30mg/kg of Edaravone had limited neuroprotective effects, while 250mg/kg exhibited robust dopamine cell survival and rescued the behavioural/motor features of the model even when given 24 hours after the neurotoxin.
The investigators concluded that “Edaravone might be a hopeful therapeutic option for PD, although several critical issues remain to be solved, including high therapeutic dosage of Edaravone for the safe clinical application in the future”
This results was followed by several additional studies investigating edaravone in models of Parkinson’s disease (Click here, here and here to read more on this). Of particular interest in all of those follow up studies was a report in which Edaravone treatment resulted in neuroprotective in genetic model of Parkinson’s disease:

Title: Edaravone prevents neurotoxicity of mutant L166P DJ-1 in Parkinson’s disease.
Authors: Li B, Yu D, Xu Z.
Journal: J Mol Neurosci. 2013 Oct;51(2):539-49.
PMID: 23657982
DJ-1 is a gene that has been associated Parkinson’s disease since 2003. The gene is sometimes referred to as PARK7 (there are now more than 20 Parkinson’s associated genomic regions, which each have a number and are referred to as the PARK genes). Genetic mutations in the DJ-1 gene can result in an autosomal recessive (meaning two copies of the mutated gene are required), early-onset form of Parkinson disease. For a very good review of DJ-1 in the context of Parkinson’s disease, please click here.
The exact function of DJ-1 is not well understood, though it does appear to play a role in helping cells deal with ‘oxidative stress’ – the over-production of those free radicals we were talking about above. Now given that edaravone is a potent antioxidant (reversing the effects of oxidative stress), the researchers conducting this study decided to test Edaravone in cells with genetic mutations in the DJ-1 gene.
Their results indicated that Edaravone was able to significantly reduce oxidative stress in the cells and improve the functioning of the mitochondria – the power stations in each cell, where cells derive their energy. Furthermore, Edaravone was found to reduce the amount of cell death in the DJ-1 mutant cells.
More recently, researchers have begun digging deeper into the mechanisms involved in the neuroprotective effects of Edaravone:

Title: Edaravone leads to proteome changes indicative of neuronal cell protection in response to oxidative stress.
Authors: Jami MS, Salehi-Najafabadi Z, Ahmadinejad F, Hoedt E, Chaleshtori MH, Ghatrehsamani M, Neubert TA, Larsen JP, Møller SG.
Journal: Neurochem Int. 2015 Nov;90:134-41.
PMID: 26232623 (This article is OPEN ACCESS if you would like to read it)
The investigators who conducted this report began by performing a comparative two-dimensional gel electrophoresis analyses of cells exposed to oxidative stress with and without treatment of Edaravone.
Um, what is “comparative two-dimensional gel electrophoresis analyses”?
Good question.
Two-dimensional gel electrophoresis analyses allows researchers to determine particular proteins within a given solution. Mixtures of proteins are injected into a slab of gel and they are then separated according to two properties (mass and acidity) across two dimensions (left-right side of the gel and top-bottom of the gel).
A two-dimensional gel electrophoresis result may look something like this:

Two-dimensional gel electrophoresis. Source: Nature
As you can see, individual proteins have been pointed out on the image of this slab of gel.
In comparative two-dimensional gel electrophoresis, two samples of solution are analysed by comparing two slabs of gel that have been injected with protein mix solution from two groups of cells treated exactly the same except for one variable. Each solution gets its own slab of gel, and the differences between the gel product will highlight which proteins are present in one condition versus the other (based on the variable being tested).
In this experiment, the variable was Edaravone.
And when the researchers compared the proteins of Edaravone treated cells with those of cells not treated with Edaravone, they found that the neuroprotective effect of Edaravone was being caused by an increase in a protein called Peroxiredoxin-2.
Now this was a really interesting finding.
You see, Peroxiredoxin proteins are a family (there are 6 members) of antioxidant enzymes. And of particular interest with regards to Parkinson’s disease is the close relationship between DJ-1 (the Parkinson’s associated protein discussed above) and peroxiredoxin proteins (Click here, here, here and here to read more about this).
In addition, there are also 169 research reports dealing with the peroxiredoxin proteins and Parkinson’s disease (Click here to see a list of those reports).
So, what do you think about a clinical trial for Edaravone in Parkinson’s disease?
Are you convinced?
Regardless, it an interesting drug huh?
Are there any downsides to the drug?
One slight issue with the drug is that it is injected via a vein. Alternative systems of delivery, however, are being explored.A biotech company in the Netherlands, called Treeway is developing an oral formulation of edaravone (called TW001) and is currently in clinical development.
Edaravone was first approved for clinical use in Japan on May 23, 2001. With almost 17 years of Edaravone clinical use, a few adverse events including acute renal failure have been noted, thus precautions should be taken with individuals who have a history of renal problems. The most common side effects associated with the drug, however, are: fatigue, nausea, and some mild anxiety.
Click here for a good overview of the clinical history of Edaravone.
So what does it all mean?
The announcement from the FDA this week regarding the approval of Edaravone as a new treatment for ALS represents a small victory for the ALS community, but it may also have a significant impact on other neurodegenerative conditions, such as Parkinson’s disease.
Edaravone is a potent antioxidant agent, which has been shown to have neuroprotective effects in various models of Parkinson’s disease and other neurodegenerative conditions. It could be interesting to now test the drug clinically for Parkinson’s disease. Many of the preclinical research reports indicate that the earlier Edaravone treatment starts, the better the outcomes, so any initial clinical trials should focus on recently diagnosed subjects (perhaps even those with DJ-1 mutations).
The take home message of this post is: given that Edaravone has now been approved for clinical use by the FDA, it may be advantageous for the Parkinson’s community to have a good look at whether this drug could be repurposed for Parkinson’s disease.
It’s just a thought.
The banner for today’s post was sourced from Forbes







 Hello, this is me – Eirwen Malin. I’m not prepared to own up to quite how many years I worked in the
Hello, this is me – Eirwen Malin. I’m not prepared to own up to quite how many years I worked in the 

























































 For today’s post, we have teamed up with Prof Frank Church from the
For today’s post, we have teamed up with Prof Frank Church from the