A new study has found traumatic brain injury with loss of consciousness is associated with the risk of Parkinson’s disease, but (interestingly) not Alzheimer’s disease. In this post we will review the study and its findings, before considering the implications of the results.
There has been a lot of talk on the interweb and various media outlets recently about the long term consequences of head injuries associated with physical sports like boxing, rugby, ice hockey and American football (click here for more on this).
Of particular concern is when individuals lose consciousness at the time of the head injury, which has been associated with worse outcomes than simply suffering a bang on the head.
A group of American researchers recently decided to assess whether there was any association between traumatic head injury with loss of consciousness and the increased risk for Alzheimer’s disease.
What they found may have profound implications for Parkinson’s disease.
Title: Association of Traumatic Brain Injury With Late-Life Neurodegenerative Conditions and Neuropathologic Findings. Authors: Crane PK, Gibbons LE, Dams-O’Connor K, Trittschuh E, Leverenz JB, Keene CD, Sonnen J, Montine TJ, Bennett DA, Leurgans S, Schneider JA, Larson EB. Journal: JAMA Neurol. 2016 Jul 11. doi: 10.1001/jamaneurol.2016.1948. PMID:27400367 (This study is OPEN ACCESS if you would like to read it)
The researchers collected the results of 3 large studies, collectively involving 7130 participants who had head injury data (2879 men and 4251 women; average age of 79.9 years). Of these 845 had suffered traumatic brain injuries with loss of consciousness for at least 1 hour. Interestingly, the researchers found no statistically significant association between traumatic brain injuries with loss of consciousness and risk of Alzheimer’s disease.
Next they looked at Parkinson’s disease and found that people who suffered traumatic brain injuries with loss of consciousness of more than 1 hour had a statistically significant increase in developing Parkinson’s disease (2-3 times more than normal controls).
Of the 7130 participants in the study, postmortem autopsy analysis reports were available for 1589 of the subjects. The researchers looked for the neuropathological hallmarks of Parkinson’s disease, called Lewy bodies, and they found no correlation between people who suffered traumatic brain injuries with loss of consciousness of less than 1 hour and the presence of Lewy bodies. When they looked in the brains of people who suffered traumatic brain injuries with loss of consciousness of more than 1 hour, they did find a correlation. And importantly these neuropathological events were not associated with genetic mutations.
So what does it all mean?
The results indicate that traumatic brain injuries with loss of consciousness of more than 1 hour could significantly increase a person’s risk of Parkinson’s disease. The crucial detail in the results is the ‘loss of consciousness of more than 1 hour’. Traumatic head injury can often result in disruption to the blood-brain-barrier (the protective film surrounding the brain), which may result in certain pathogens entering the brain. So the more severe the injury, perhaps the longer the barrier is disrupted. Why this event may relate solely to Parkinson’s disease and not Alzheimer’s disease, however, remains to be determined.
It would be interesting to assess how this finding relates to the greater Parkinson’s community. That is to say, determine how many of the people with Parkinson’s disease have a head injury with loss of consciousness in their past medical records?
Reading this study, one cannot help thinking of the recent passing of Boxing great Muhammad Ali. Ali died this year having spent the last third of his life living with Parkinson’s disease. Many boxing careers have probably involved one or two severe head injuries with loss of consciousness, so why are there not more cases of Parkinson’s disease in the boxing community? Many retired boxers suffer from what is called Dementia pugilistica – a neurodegenerative condition with Alzheimer’s-like dementia. Some estimates suggest that 15-20% of boxers may be affected, with symptoms usually starting 12-16 years after the start of a career in boxing. Some very famous boxers have been diagnosed with this condition, including world champions Floyd Patterson, Joe Louis, Sugar Ray Robinson and boxer/coach Freddie Roach.
The difference between the results of today’s study and dementia pugilistica may lie in the repeated nature of the injuries in boxers and the length of time individuals were unconscious. It will be interesting to see what becomes of this research.
The banner for today’s post was sourced from the Huffington Post
This week an interesting new study dealing with the biology of Alzheimer’s was published in the journal Science Translational Medicine. It has drawn a lot of attention as it may be turning our understanding of Alzheimer’s disease on it’s head. If the results are independently replicated and verified, it could potentially have major implications for Parkinson’s disease.
For the last 30 years, a protein called beta-amyloid has been considered one of the bad boys of the most common neurodegenerative condition, Alzheimer’s disease.
What is Alzheimer’s disease?
Alzheimer’s disease is a progressive neurodegenerative condition that can occur in middle or old age. It involves a generalized degeneration of the brain, not localised to specific regions like Parkinson’s disease.
What happens in the Alzheimer’s brain?
In the brain, in addition to cellular loss, Alzheimer’s is characterised by the presence of two features:
Neurofibrillary tangles
Amyloid plaques
The tangles are aggregations of a protein called ‘Tau’ (we’ll comeback to Tau in a future post). These tangles reside within neurons initially, but as the disease progresses the tangles can be found in the space between cells – believed to be the last remains of a dying cell.
A normal brain vs an Alzheimer’s affected brain. Source: MMCNeuro
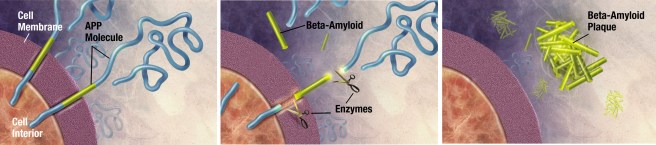
Amyloid plaques are clusters of proteins that sit between cells. A key component of the plaque is beta amyloid. Beta-amyloid is a piece of a larger protein that sits in the outer wall of nerve cells where it has certain functions. In certain circumstances, specific enzymes can cut it off and it floats away.
Beta-amyloid is a very “sticky” protein and for a long time it has been believed that free floating beta-amyloid proteins begin sticking together, gradually building up into the large amyloid plaques. And these large plaques were considered to be involved in the neurodegenerative process of Alzheimer’s disease.
So what was discovered this week?
This week a study was published that suggests a new (and positive) function for beta amyloid:
Title: Amyloid-β peptide protects against microbial infection in mouse and worm models of Alzheimer’s disease. Authors: Kumar DK, Choi SH, Washicosky KJ, Eimer WA, Tucker S, Ghofrani J, Lefkowitz A, McColl G, Goldstein LE, Tanzi RE, Moir RD. Journal: Sci Transl Med. 2016 May 25;8(340):340ra72. PMID:27225182
The researchers took three types of mice:
genetically normal mice
mice with no beta amyloid
mice producing a lot of beta amyloid
They infected all of the mice with the microbe that causes meningitis, and they found that the mice producing a lot of beta amyloid lived significantly longer than other groups of mice. They then repeated the experiment in a species of microscopic worm – called C.elegans – and found similar results. These findings suggested that beta amyloid was having a positive effect in the brain.
But then they noticed something strange.
The mice producing a lot of beta amyloid usually do not develop a lot of protein aggregation until old age, but when the researchers looked in the brains of the mice they infected with meningitis, they found significant levels of aggregation in the mice producing a lot of beta amyloid but at a young age..
This led the researchers to conduct some cell culture experiments in which they watched what was happening to the bacteria and beta amyloid. They found that the beta amyloid was sticking to the bacteria and this was leading to the formation of protein aggregates.
The results of these experiments suggested to the researchers an intriguing possibility that beta amyloid may be playing a protective in the brain – acting as an immune system for the brain – against infection.
Thus the aggregations we see in the brains of people with Alzheimer’s may not be the cause of the cell death associated with the disease, but rather evidence of the ‘brain’s immune system’ trying to fight back against unknown infectious agents. The researcher’s of the study were quick to point out that this antimicrobial action of beta amyloid is simply a new function of the protein, and it may have nothing to do with the disease itself. But it will be interesting to see where this research goes next.
What has this got to do with Parkinson’s disease?
Parkinson’s disease is only definitive diagnosed at the postmortem stage. This is done by microscopic examination of the brain. In the brains of people with Parkinson’s disease, there are protein aggregates calls Lewy bodies. These are densely packed clusters of a protein called ‘alpha synuclein‘.
The brown spot is a Lewy body inside of a brain cell. Source: Cure Dementia
If the results of the study presented above are correct and beta amyloid is a protective protein in the brain against infection, could it not be that alpha synuclein may be playing a similar role? It is a fascinating idea that it will be interesting to test.
What are the implications of the study?
Currently, there are numerous clinical trials for Alzheimer’s disease, involving treatments that act against beta amyloid. If the study presented above is correct, and beta amyloid has a role in protecting the brain, these new treatments in clinical trial may actually be weakening the brain’s ability to fight infection.
Similarly, if alpha synuclein is found to exhibit ‘protective’ properties like beta amyloid, then the alpha synuclein vaccine clinical trials currently underway (in which the body’s immune system is primed to remove free floating alpha synuclein, in an attempt to stop the disease from spreading) may need to be reconsidered. At a minimum, investigations into whether alpha synuclein has antimicrobial properties need to be conducted.
If I were to tell you that there exists a miraculous elixir derived from the saliva of a monster and it may aid us in the treatment of Parkinson’s disease, would you think me mad?
In 1974, a small study was published in the Journal of Chronic Diseases that presented a rather startling set of results:
In the study, Lipman and colleagues conducted some routine glucose tolerance tests on a group of 56 people with Parkinson’s Disease (7 additional subjects with Parkinson’s were excluded because they had been previously diagnosed with diabetes).
After being asked to fast overnight, the subjects were then given 100g of glucose and blood samples were collected from them every hour for 3 hours. When the glucose levels in the blood were measured and compared with the results of 5 previous studies conducted on normal healthy adults of the same age (one of those studies involved 7000 participants), it was found that the people with Parkinson’s disease in the Lipman study had a much higher average level of glucose in their blood than all of the other 5 studies looking at healthy individuals.
Shockingly, almost half (46.4%) of the participants in the Lipman study actually fulfilled the criteria for a diagnosis of diabetes.
More recent survey data has revealed that diabetes is established in between 8–30% of people with Parkinson’s disease (click here for more on this) – obviously this is in excess of the approximately 6% prevalence rate in the general public (Source: DiabetesUK).
What is diabetes?
‘Diabetes mellitus’ is what we commonly refer to as diabetes. It is basically a group of metabolic diseases that share a common feature: high blood sugar (glucose) levels for a prolonged period.
Diabetic patient doing glucose level blood test using ultra mini glucometer and small drop of blood from finger and test strips isolated on a white background. Device shows 115 mg/dL which is normal
Type 1, which involves the pancreas being unable to generate enough insulin. This is usually an early onset condition (during childhood) and is controlled with daily injections of insulin.
Type 2, which begins with cells failing to respond to insulin. This is a late/adult onset version of diabetes that is caused by excess weight and lack of exercise.
Type 3, occurs during 2-10% of all pregnancies, and is transient except in 5-10% of cases.
What is this stuff called insulin?
Insulin is a hormone – that our body makes – which allows us to use sugar (glucose) from the food that you eat. Glucose is a great source of energy. After eating, our body is releases insulin which then attaches to cells and signals to those cells to absorb the sugar from our bloodstream. Without insulin, our cells have a hard time absorbing glucose. Think of insulin as a “key” which unlocks cells to allow sugar to enter the cell.
Ok, so how is it all connected to Parkinson’s disease?
The short answer is ‘we currently don’t know’.
There have, however, been numerous studies now that suggest an association between diabetes and Parkinson’s disease. The first of these studies was:
Title: Prospective cohort study of type 2 diabetes and the risk of Parkinson’s disease. Authors: Driver JA, Smith A, Buring JE, Gaziano JM, Kurth T, Logroscino G. Journal: Diabetes Care. 2008 Oct;31(10):2003-5. PMID:18599528
In this study, 21,841 male doctors (participants in the Physicians’ Health Study) were followed over 23 years. The researchers found that people with diabetes had an increased risk of developing Parkinson’s disease risk. Interestingly they reported that the highest Parkinson’s disease risk was seen in individuals with short-duration, older-onset diabetes.
In another study:
Title: Diabetes and risk of Parkinson’s disease. Authors: Xu Q, Park Y, Huang X, Hollenbeck A, Blair A, Schatzkin A, Chen H. Journal: Diabetes Care. 2011 Apr;34(4):910-5. doi: 10.2337/dc10-1922. Epub 2011 Mar 4. PMID:21378214
This study came from another long term study, which was following 288,662 participants of the National Institutes of Health-AARP Diet and Health Study. The researchers found that the risk of Parkinson’s disease was approximately 40% higher among diabetic patients than among participants without diabetes. In this study, however, the analysis showed that the risk was largely limited to individuals who had diabetes for more than 10 years.
A third study:
Title: Diabetes and the risk of developing Parkinson’s disease in Denmark. Authors: Schernhammer E, Hansen J, Rugbjerg K, Wermuth L, Ritz B. Title: Diabetes Care. 2011 May;34(5):1102-8. PMID:21411503
Using data from the nationwide Danish Hospital Register hospital records, the researchers found that having diabetes was associated with a 36% increased risk of developing Parkinson’s disease. Interestingly, they reported that the risk was stronger in women and patients with early-onset Parkinson’s disease (eg. diagnosed before the age of 60 years).
EDITORIAL NOTE HERE: It is important to understand that these studies do not suggest that having diabetes will naturally lead to Parkinson’s disease. They are simply pointing out that diabetics have an increased risk of developing the condition. We present this data here for informative purposes and to make people aware.
It is of interest to note that there is also an association between diabetes and Alzheimer’s disease (click here and here for more on this). Thus Parkinson’s disease is not the only neurodegenerative condition associated with diabetes.
Is the association between Parkinson’s disease and diabetes genetic?
At present, the answer is no.
The connection between diabetes and Parkinson’s disease does not appear to be genetic, as genome wide sequencing studies have found no common mutations or associations between the two conditions (click here for more on this).
Named after the Gila River Basin of New Mexico and Arizona, where these lizards are found found, the saliva of the Gila monster was found to have some rather amazing properties with regards to the management of type 2 diabetes. This was due largely to a protein extracted from the saliva, called exendin-4. Scientists have made a synthetic version of exendin-4 which they have called Exenatide.
When tested in a three year clinical trial, Exenatide was found to return people with type 2 diabetes to healthy sustained glucose levels and progressive weight loss.
Exenatide is a glucagon-like peptide-1 (GLP-1) agonist. These types of drugs work by mimicking the functions of the natural hormones in your body that help to lower blood sugar levels after meals. They do this by aiding the release of insulin from the pancreas, blocking a hormone that causes the liver to release its stored sugar into the bloodstream, and slowing glucose absorption into the bloodstream.
Great, but what has this got to do with Parkinson’s disease?!?
Exenatide has also been found to have impressive results in both animal models of Parkinson’s disease and in an open-label clinical trial.
The first study to report a positive effect of Exenatide in a Parkinson’s disease model was:
Title: Peptide hormone exendin-4 stimulates subventricular zone neurogenesis in the adult rodent brain and induces recovery in an animal model of Parkinson’s disease. Authors: Bertilsson G, Patrone C, Zachrisson O, Andersson A, Dannaeus K, Heidrich J, Kortesmaa J, Mercer A, Nielsen E, Rönnholm H, Wikström L. Journal: J Neurosci Res. 2008 Feb 1;86(2):326-38. PMID:17803225
In this study, the scientists found that exendin-4 (aka Exenatide) improved both behavioural motor ability and protected dopamine neurons in a rodent model of Parkinson’s disease (and the drug was given 5 weeks after the animals developed the motor features). How these results were achieved – the biology behind the results – is unclear, but the effect was interesting enough to encourage other groups to also test Exenatide and they found similar results:
Title: Glucagon-like peptide 1 receptor stimulation reverses key deficits in distinct rodent models of Parkinson’s disease. Authors: Harkavyi A, Abuirmeileh A, Lever R, Kingsbury AE, Biggs CS, Whitton PS. Journal: J Neuroinflammation. 2008 May 21;5:19. doi: 10.1186/1742-2094-5-19. PMID:18492290 (This study is OPEN ACCESS if you would like to read it)
The scientists in this study tested exendin-4 (aka Exenatide) on two different rodent models of Parkinson’s disease and they found similar results to the previous study. The drug was given 1 week after the animals developed the motor features, but still positive effects were observed.
These (and other) initial results led to the initiation of a clinical trial. Given that Exenatide is already approved for use with diabetes, testing the drug in Parkinson’s disease was a relatively straightforward process (funded by the Cure Parkinson’s Trust).
Title: Exenatide and the treatment of patients with Parkinson’s disease. Authors: Aviles-Olmos I, Dickson J, Kefalopoulou Z, Djamshidian A, Ell P, Soderlund T, Whitton P, Wyse R, Isaacs T, Lees A, Limousin P, Foltynie T. Journal: J Clin Invest. 2013 Jun;123(6):2730-6. PMID:23728174 (This study is OPEN ACCESS if you would like to read it)
The researchers running the clinical study gave Exenatide to a group of 21 patients with moderate Parkinson’s disease and evaluated their progress over a 14 month period (comparing them to 24 control subjects with Parkinson’s disease). Exenatide was well tolerated by the participants, although there was some weight loss reported amongst many of the subjects (one subject could not complete the study due to weight loss). Importantly, Exenatide-treated patients demonstrated improvements in their clinician assessed PD ratings, while the control patients continued to decline.
Importantly, in a two year follow up study – this was 12 months after the patients stopped receiving Exenatide – the researchers found that patients previously exposed to Exenatide demonstrated a significant improvement (based on a blind assessment) in their motor features when compared to the control subjects involved in the study.
The results of this initial clinical study are intriguing and exciting, but it is important to remember that the study was open-label: the subjects knew that they were receiving the drug. This means that we can not discount the placebo effect causing some of the beneficial effects reported.
We look forward to reading the results of that trial.
And Exenatide is not the only diabetes drug being tested
Pioglitazone is another licensed diabetes drug that is now being tested in Parkinson’s disease. It reduces insulin resistance by increasing the sensitivity of cells to insulin. Pioglitazone has been shown to offer protection in animal models of Parkinson’s disease (click here and here for more on this). And the drug is currently being tested in a clinical trial.
We look forward to reading these results as well.
Summing up
As with melanoma and red hair, there appears to be a curious connection between diabetes and Parkinson’s disease. Large longitudinal studies point to people with diabetes as having a higher risk of Parkinson’s disease than non-diabetic individuals. Why this is remains unclear, but some of the drugs used for treating diabetes may provide novel therapeutic options in the treatment of Parkinson’s disease. We will continue to follow this research and report results as they come to hand.
And you didn’t believe me about the monster saliva!
There was an interesting new study published yesterday:
Title: Human DNA methylomes of neurodegenerative diseases show common epigenomic patterns. Author: Sanchez-Mut JV, Heyn H, Vidal E, Moran S, Sayols S, Delgado-Morales R, Schultz MD, Ansoleaga B, Garcia-Esparcia P, Pons-Espinal M, de Lagran MM, Dopazo J, Rabano A, Avila J, Dierssen M, Lott I, Ferrer I, Ecker JR, Esteller M. Journal: Transl Psychiatry. 2016 Jan 19;6:e718. doi: 10.1038/tp.2015.214. PMID:26784972 – this article is OPEN ACCESS if you would like to read it.
The researchers were curious to look for common genetic markers between the major neurodegenerative disease. It is often forgotten that the different neurodegenerative conditions, such as Alzheimer’s disease and Parkinson’s disease, share some common pathological features (the characteristic signs of the diseases in the brain).
For example, when you look at the brains of people with Alzheimer’s disease, approximately 50% of them will also have the alpha-synuclein-containing ‘Lewy bodies’ in their brains, which are more commonly associated with Parkinson’s disease. Likewise, Beta-amyloid plaques and neurotangles, which are characteristic features of Alzheimer’s disease are commonly found in Parkinson’s disease brains (click here and click here for more on this topic).
To find these shared genetic markers, the researcher extracted DNA from the prefrontal cortex (Brodmann area 9) of the brains of people with Alzheimer’s disease, dementia with Lewy bodies, Parkinson’s disease and Alzheimer-like neurodegenerative profile associated with Down’s syndrome samples (more than 75 percent of people with Down Syndrome aged 65 and older develop Alzheimer’s disease – click here for more on this).
Importantly, the researchers were looking at DNA methylation, which is a commonly used tool that allows a cell to fix genes in the “off” position. That is to say, the gene can not be activated. Thus the researchers were looking for regions of DNA that have to closed down.
They found that a very defined set of genes are turned off in these neurodegenerative disorders, suggesting that these condition might have similar underlying mechanisms or processes that subsequently develop into different clinical entities. These newly identified regions of DNA methylation will be further investigated with the goal that one day they may be used as biomarkers in diagnosis and also as potential new targets for the regenerative therapies.
She was admitted by her husband to the Institution for the Mentally Ill and for Epileptics in Frankfurt, Germany on the 25th November, 1901. Her husband complained that she suffering memory loss and having delusions.
The attending doctor was Dr Alois Alzheimer.
Over the next year, Alois continued to examine Auguste – and what he began calling the “Disease of Forgetfulness” – until he left the institute to take up a position in Munich. He made regular visits back to Frankfurt, however, to follow up on Auguste.
Auguste dies on the 8th April, 1906. She had become completely demented and had existed in a vegatative state. When he examined the brain, Alois found the hall marks of what we today call ‘Alzheimer’s disease’ (namely neurofibrillary tangles and plaques).
Now, almost 110 years later, Alzheimer’s disease is the most common neurodegenerative condition – Parkinson’s disease is the second most common. Alzheimer’s affects 850,000 people in the UK alone (Source: Alzheimer’s Society). Huge efforts have been made in researching this condition and last week some interesting new data was published about the disease that may also have implications for Parkinson’s disease.
Title: Evidence for human transmission of amyloid-β pathology and cerebral amyloid angiopathy. Authors: Jaunmuktane Z, Mead S, Ellis M, Wadsworth JD, Nicoll AJ, Kenny J, Launchbury F, Linehan J, Richard-Loendt A, Walker AS, Rudge P, Collinge J, Brandner S. Journal: Nature. 2015 Sep 10;525(7568):247-50. PMID:26354483
Published in the prestigious science journal, Nature, the article found signs of Alzheimer’s disease in the autopsied brains of people who had died from Creutzfeldt-Jakob disease (CJD) – the prion induced neurodegenerative condition.
What’s a prion?
Good question! A prion is a small infectious particle – usually composed of an abnormally-folded version of a normal bodily protein – that causes progressive neurodegenerative conditions. The first prion discovered in mammals was Prion protein (PRP): this is the prion that causes CJD.
PrP is considered the only known prion in mammals, but recently other proteins have exhibited prion-like behaviour. One such protein is Amyloid-β protein – the protein that is found clustered in clumps in the brains of people with Alzheimer’s disease.
The brains that were analysed in the study from the journal Nature were collected at death from people who had received human growth-hormone earlier in their lives. The growth-hormone had been extracted from human cadavers and it was injected into people with growth problems (this was a common practise during the 1950s to mid 1980s). Unfortunately, some of the growth-hormone appears to have been contaminated with PrP (possibly one of the cadavers used had undiagnosed CJD) and numerous people were injected with it (65 cases in Britain alone). Many of these individuals have been followed and we have learned a great deal from them regarding CJD. Some of these individuals have also donated their brains to science and it was some of these brains that were analysed in the study being discussed here.
What the authors of the study were expecting to see when they analysed these brains was lots of clusters of PrP. What the authors were not expecting to see was the clustering of Amyloid-β protein in these brains.
Amyloid-β protein (brown) in a section of brain tissue. Source: Nature
Of the eight brains (from people who received PrP infected growth-hormone) the authors analysed, six of them had clustering of Amyloid-β protein present in the brain (in four of those cases it was wide-spread). These brains came from people aged between aged 36–51 years – in such cases it is very rare to see large accumulations of Amyloid-β protein. The researchers also analysed the DNA of the individuals involved in the study and found that none of them were genetically susceptible to Alzheimer’s disease.
The researchers then compared these six brain with the brains of people who died from CJD caused by other means – 119 brains in total and none of them had Amyloid-β protein present in the brain. From these and other experiments, the authors suggested that this was the first human evidence of transmission of Alzheimer’s related pathology.
It is very important to note several details in the study:
1. None of the people whose brains were used in the study exhibited the clinical signs of Alzheimer’s.
2. None of the brains with Amyloid-β pathology had what is called ‘hyperphosphorylated tau neurofibrillary tangles’ – SImilar clumps of Amyloid-β protein, tau neurofibrillary tangles are another characteristic feature of Alzheimer’s disease brains. Their absence is curious.
3. The authors can not dismiss the possibility that the Amyloid-β was not present in the growth-hormone solution. In this case, the Amyloid-β accumulation in the brains could have been caused by some other unknown agent that was present in the injected solution.
A rare editorial note here: The Science of PD is disappointed with the way that this study has been handled by the wider media. While the results are interesting and the authors can be congratulated on their work, a correct interpretation of the results requires further study. This study has simply demonstrated was that Amyloid-β protein may be transmissible in a similar fashion to PrP.
So why are we discussing this Alzheimer’s research here at the Science of Parkinson’s Disease?
Well, for a long time now Parkinson’s researchers have suspected that similar mechanisms may underlying what is happening in PD. That is to say, a prion-like protein may be transmitted between cells in the body (possibly from the gut to the brain – see previous posts) allowing the disease to progress. One protein in particular, Alpha Synuclein, which is present in Lewy bodies – the neurological features associated with Parkinson’s disease, has been implicated in this regards. Recent evidence from lab-based studies suggest that this is possible in cell cultures and in rodents, but whether it is possible in humans is yet to be determined.
NOTE: Since publishing this post, we contacted the authors of the study regarding the presence of Alpha Synuclein and they told us that they were currently conducted a large study investigating what other proteins are also present. Thus far they have not seen any Alpha Synuclein accumulation. Interesting….

















{kind=link}