On the 26-31st March, the 14th International Conference on Alzheimer’s and Parkinson’s Diseases (or ADPD meeting) was held in Lisbon, Portugal.
For 5 days – between 8:30am and 7:30pm each day – over 4000 researchers were able to attend lectures of new results and ideas, in any of 8 different auditoriums. Alternatively, they could wander among hundreds of research posters.
It was a marathon effort, however, for all attendees. And a great deal of new results were shared.
In today’s post, we will discussed what was presented at the 2019 ADPD meeting and what was actually learnt.
Lisbon is a city, midway down the western coast of the Iberian Peninsula.
It is home to a little over 500,000 people (3 million in the wider metropolitan area), and it serves as the capital city for the Portuguese people.
The Castelo de Sao Jorge, rises above Lisbon. Source: Wikipedia
Interestingly, it is the 2nd oldest European capital city (after Athens), and has had a rich and fascinating history given its strategic location. But on the 1st November 1755, 20% of the population were killed and 85% of the city’s structures were destroyed by a terrible earthquake and subsequent tsunami, which resulted in the vast majority of the city being rebuilt.
The ‘new city’ is laid out in bairros de Lisboa (neighbourhoods of Lisbon) across a hilly landscape, providing views of the River Tagus at every vantage point. And while walking the steep cobblestoned streets is delightful, there is a system of vintage public trams that can take a lot of the leg work out of the effort.
This week the ‘Michael J. Fox Foundation for Parkinson’s Research’ and ‘The Silverstein Foundation for Parkinson’s with GBA’ announced that they are collaboratively awarding nearly US$3 million in research grants to fund studies investigating an enzyme called beta glucocerebrosidase (or GCase).
Why is this enzyme important to Parkinson’s?
In today’s post, we will discuss what GCase does, how it is associated with Parkinson’s, and review what some of these projects will be exploring.
He is a General Partner of Global Private Equity at OrbiMed – the world’s largest fully dedicated healthcare fund manager. During his time at OrbiMed, the company has invested in healthcare companies that have been involved with over 60 FDA approved products.
In February 2017 – at just 49 years of age – Jonathan was diagnosed with Parkinson’s.
Rather than simply accepting this diagnosis, however, Mr Silverstein decided to apply the skills that he has built over a long and successful career in funding biotech technology, and in March 2017, he and his wife, Natalie, set up the Silverstein Foundation for Parkinson’s with GBA.
The foundation has just one mission: “to actively pursue and invest in cutting edge research with the goal of discovering new therapies for the treatment of Parkinson’s Disease in GBA mutation carriers”
And it seeks to address this by achieving three goals:
to find a way to halt the progression of Parkinson’s with GBA.
to identify regenerative approaches to replace the damaged/lost cells
The monitoring and assessment of the symptoms/features of Parkinson’s is a big deal in the research community at the moment.
There is currently a mad hunt for ‘biomarkers’ – reliably measurable physical characteristics – that could help not only with the assessment of individuals living with the condition, but could also aid in the running of clinical trials by providing additional measures of efficacy/benefit.
Recently an interesting perspective was written by some of the leading researchers in this field.
In today’s post, we review what the perspective outlined, and we will discuss other aspects of the biomarker research that need to be considered by the wider Parkinson’s community.
Scientific journals will often invite the research leaders in a particular field of investigation to write a brief journal article that deals with unique view of a common problem.
Articles of this nature are called ‘Perspectives‘.
And recently a very interesting perspective was published in the journal Science on the topic of biomarkers for Parkinson’s.
Title: Finding useful biomarkers for Parkinson’s disease Authors: Chen-Plotkin AS, Albin R,….a lot of additional authors…, Zhang J Journal: Science Translational Medicine, 15 Aug 2018, 10 (454), eaam6003. PMID: N/A
This perspective included a rather long list of a ‘who’s-who’ of Parkinson’s researchers – both academic and industry. Even members of the Michael J Fox Foundation and Verily/Google Life Sciences were included.
The perspective sought to highlight ‘the “ecosystem” of shared biofluid sample biorepositories and data sets will focus biomarker efforts in Parkinson’s‘. It is a very enlightening read, one that begs for reader responses. But sadly the article is behind a ‘pay wall’, and so many in the Parkinson’s community won’t be able to provide any thoughts or feedback.
Shame.
But not to worry, we can discuss the matter here. And the best place to start that discussion is with the obvious first question:
What is a biomarker?
A biomarker is an objectively measurable physical characteristic associated with a condition. It is a biological component of a condition that correlates with that condition in some way. For example, the DaTscan brain imaging technique provides a ‘biomarker’ for Parkinson’s by measuring the amount of dopamine re-absorption in the brain. By labelling the dopamine neurons with a radioactive marker, we can quantify the levels of dopamine activity in a person.
Last year – two years after actor Robin Williams died – his wife Susan Schneider Williams wrote an essay entitled The terrorist inside my husband’s head, published in the journal Neurology.
It is a heartfelt/heartbreaking insight into the actor’s final years. It also highlights the plight of many who are diagnosed with Parkinson’s disease, but experience an array of additional symptoms that leave them feeling that something else is actually wrong.
Today’s post is all about Dementia with Lewy bodies (or DLB). In particular, we will review the latest refinements and recommendations of the Dementia with Lewy Bodies Consortium, regarding the clinical and pathologic diagnosis of DLB.
On the 28th May of 2014, the actor Robin Williams was diagnosed with Parkinson’s disease.
At the time, he had a slight tremor in his left hand, a slow shuffling gait and mask-like face – some of the classical features of Parkinson’s disease.
According to his wife, the diagnosis gave the symptoms Robin had been experiencing a name. And this brought her a sense of relief and comfort. Now they could do something about the problem. Better to know what you are dealing with rather than be left unsure and asking questions.
But Mr Williams sensed that something else was wrong, and he was left unsure and asking questions. While filming the movie Night at the Museum 3, Williams experienced panic attacks and regularly forgot his lines. He kept asking the doctors “Do I have Alzheimer’s? Dementia? Am I schizophrenic?”
Williams took his own life on the 11th August 2014, and the world mourned the tragic loss of a uniquely talented performer.
We live in an increasingly interconnected technological world.
One can chose to embrace it or ignore it, but I don’t think anyone can do anything to stop it – the masses seem to desire it.
The benefits of all this technology are many, however, for people with Parkinson’s disease. In today’s post we will look at some of the ways wearable technology can be used to improve the lives of people with Parkinson’s disease.
The great Albert Einstein once said that he feared “the day that technology will surpass our human interaction. The world will have a generation of idiots”.
While there are certainly many examples of this situation playing out in our modern society today, the quote misses the mark with regards to the application and benefits of such technology.
For example, people with Parkinson’s disease can now communicate with people in the Parkinson’s community (like ourselves) from anywhere the world. They can reach out and share not only their experiences, but also what treatments and remedies have worked for them.
And then there are the other less obvious applications of an interconnected world:
A schematic illustrating the limited monitoring of Parkinson’s. Source: Riggare
On her fantastic blog, engineer and ‘proud mother’ Sara Riggare posted the image above to illustrate the ridiculous current situation regarding the monitoring of Parkinson’s disease. In 2014, she spent 8,765 hours in self care, applying her own knowledge and experience to managing her Parkinson’s disease (8,765 being the number of hours in a year) and had just 1 hour with her physician.
The schematic perfectly illustrates perfectly how little monitoring people with Parkinson’s receive in the standard healthcare system.
People like Sara, however, are taking matters into their own hands. She has become an enthusiastic proponent of ‘self tracking’:
Self tracking represents a fantastic opportunity not only for people with Parkinson’s disease to track their progress, but also for researchers to build up large databases of information relating to the disease from which new theories/hypotheses/treatment approaches could be generated.
And this is possible on a global scale, only because we are a generation of idiots living in a fully interconnected world.
Recently the technology company Apple announced that it is working on new devices to help track Parkinson’s disease (Click here and here for more on this). The company already offers ResearchKit – a platform available on their iphone.
Apple, however, is actually coming to this party rather late. The Michael J Fox foundation and computer giant Intel formed a partnership back in 2014 to look at wearable technology (Click here to read more about this).
And there are already dozens of applications that can be used on smart phones and tablets. We have previously discussed one such app from a company called uMotif – Click here to read that post.
In addition, there are other smart phone apps available that readers could try (such as MyTherapyApp) and you can even support new applications as they are being developed (such as Progress Recorder).
What if I don’t have time for entering all the details on the smart phone app?
Not a problem.
Why not just wear a recording sensor? The same way you may wear a piece of jewellery. Simple, easy approach and you can just forget that it is even there.
Would you like an interesting example?
This is Utkarsh Tandon.
He’s a 17 years old student at Cupertino High School. He is also the Founder and CEO of OneRing, an intelligent tool for monitoring Parkinson’s
Yes, you read that correctly – he is just 17 years old. Smart kid, we’ll be watching him.
Why is this technology important?
Until recently out understanding of Parkinson’s has relied entirely on what occurs in the lab and clinic based settings. Now information is being collected 24 hours a day. From sleep quality apps to measuring tremor, all of this technology has several very positive features from the view point of research scientists:
Objective monitoring – rather than subjective measures (eg. clinician’s opinion or subject survey) definitive, replicatable data can be generated.
Continuous monitoring – rather than brief periods of monitoring in an artificial research clinic environment, data can be collected in real world settings on a continuous basis
Data accessibility – rather than pencil and paper collection of results, data can be collected electronically and converted to different formats.
Participant engagement – this included benefits such as getting the community involved with the research, getting feedback about the technology throughout the study, and being able to provide subjects with performance reports on a regular basis.
Is wearable tech only for measuring Parkinson’s disease?
No.
Recently it has also started to aid people with the condition. The best example of this is the story that has most recently captured the attention of the Parkinson’s community here in the UK:
Emma Lawton was diagnosed with Parkinson’s disease at just 29 years of age. Working with Haiyan Zhang (Director of Innovation at Microsoft Research) and colleagues, a bracelet was created that counteracted the tremor in Emma’s wrist.
It’s a good story.
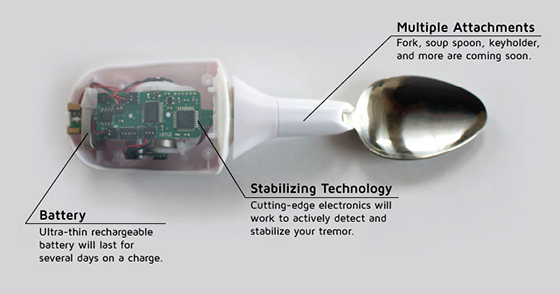
Other tech is helping to make life easier for people with Parkinson’s disease – just have a look at what LiftWare is doing.
The point of this post was to make readers aware of some of the technological resources that are available to them in this modern age. Using these tools, we can quickly collect a vast amount of information regarding all aspects of life for people with Parkinson’s disease. And it also offers folks the opportunity to get involved with research indirectly (if they have a fear of university hospitals!).
There is also another element to all of this recording of information about Parkinson’s disease that is not immediately apparent: we are potentially (and hopefully) the last generations of human being that will be affected by Parkinson’s disease. If current research efforts allow us to block or dramatically slow the condition in the near future, there may not be a disease for our descendants to worry about. While this is a very worthy goal, there is also a responsibility on the current generation to record, document and learn as much as we can about the condition so that those future generations will have information at hand regarding a forgotten medical condition.
Some folks are already doing this in their own creative ways. For example, we recommend all readers subscribe to PD365 – a fantastic project in which David Sangster and Emma Lawton (her of the bracelet described above) will be making one short video each day about life with Parkinson’s disease. Raising awareness about the condition and providing intimate insight into basic daily life with PD.
Here is Emma’s first video:
And here is David’s first video:
And this idea is really important.
Consider the great fire of London in 1666. It is estimated that the fire destroyed the homes of 70,000 of the City’s 80,000 inhabitants (Source: Wikipedia), and yet our best sources of information regarding the events of that catastrophe are limited to just a few books like the diary of Samuel Pepys.
This may seem like a silly example, but the premise stands. Given all of the technology we have available today, it would be a great failure for our generation not to be able to provide a thorough source of information regarding this disease.
That said, have a think about getting involved.
The banner for today’s post was sourced from Raconteur
The diagnosis of Parkinson’s disease can only be definitively achieved at the postmortem stage.
There is currently no diagnostic test for this task and we are reliant on the training and skills of the neurologists making the diagnosis. Brain imaging techniques (such as DAT-scans) are great, but they can only aid physicians in their final decision.
And those decisions are not always right.
In 1992, a study looking at the brains of 100 subjects who had died with Parkinson’s disease, found that 24% of the casesdid not fulfill the pathological requirements for the diagnosis of Parkinson’s disease. That study was:
Title: Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. Authors: Hughes AJ, Daniel SE, Kilford L, Lees AJ. Journal: Journal of Neurol Neurosurg Psychiatry. 1992 Mar;55(3):181-4. PMID:1564476
Unfortunately, despite years of research, it would appear that there is still a large degree of error in the clinical diagnosis of Parkinson’s disease. A study published in 2014 in the journal Neurology that suggested that there is currently a 15% rate of misdiagnosis. That study was:
Title: Low clinical diagnostic accuracy of early vs advanced Parkinson disease: clinicopathologic study. Authors: Adler CH, Beach TG, Hentz JG, Shill HA, Caviness JN, Driver-Dunckley E, Sabbagh MN, Sue LI, Jacobson SA, Belden CM, Dugger BN. Journal: Neurology. 2014 Jul 29;83(5):406-12. PMID:24975862
It has to be said that clinicians face a very difficult task in diagnosing Parkinson’s disease. The variety of features (symptoms) that patients present with in the clinic, and the lack of diagnostic tools, leave neurologists making a judgement based largely on clinical observations.
But this degree of error ultimately has a huge impact on clinical studies and trials: if 10-20% of the participants are not Parkinsonian, are we really going to observe an accurate result?
Better diagnostic tests/tools are critically required.
In November last year, a study was published in the journal Immunology Letters which may help in this regard:
Title: Potential utility of autoantibodies as blood-based biomarkers for early detection and diagnosis of Parkinson’s disease. Authors: DeMarshall CA, Han M, Nagele EP, Sarkar A, Acharya NK, Godsey G, Goldwaser EL, Kosciuk M, Thayasivam U, Belinka B, Nagele RG; Parkinson’s Study Group Investigators. Journal: Immunol Letters, 168(1), 80-8. PMID:26386375 (this article is OPEN access if you would like to read it)
The researchers took 398 subjects, including 103 early-stage Parkinson’s disease subjects and they collected blood samples from them. They then screened the blood for 9,486 different autoantibodies that could be useful as biomarkers for Parkinson’s disease.
Antibodies are produced by our immune system to determine what is ‘self’ and not ‘self’. They are the foundation of our defenses against the big, bad germ/bacteria world. Autoantibodies are antibodies produced by our immune system that are directed against our own tissues. They target ‘self’.
And yeah, that is bad. Autoantibodies are associated with autoimmune diseases such as Lupus.
We are not sure why we produce autoantibodies. The causes of their production vary greatly and are not well understood. In Parkinson’s disease, however, autoantibodies may be produced as a result of the cell death in the brain. Some of the debris resulting from the dying cells will make its way into the bloodstream, to be removed from the body. Whilst in the blood, some of that debris could trigger the immune system, thus resulting in the production of autoantibodies.
De Marshall et al (the researchers who conducted this study) were hoping to take advantage of this autoantibody production and use them as biomarkers to not only differentiate between people with and without Parkinson’s disease, but also to differentiate between different stages of Parkinson’s disease (see the figure below).
Attempting to differentiate between different stages of Parkinson’s disease. Source: Immuno Letters
The researchers found that using the top 50 autoantibodies that they associated with Parkinson’s disease, they could successfully differentiate between people with and without Parkinson’s disease with 90% prediction accuracy in a blind analysis (they actually found that just the top 4 autoantibodies were enough).
Interestingly, the researchers then compared the early Parkinson’s group with a mild-moderate Parkinson’s group and they found that they could differentiate between the two groups with an overall accuracy of 97.5%!
These are very exciting results and we will be following this work with interest – not only from the standpoint of biomarkers, but also the role of autoantibodies in Parkinson’s disease.

 Lisbon. Source: stmed
Lisbon. Source: stmed The Castelo de Sao Jorge, rises above Lisbon. Source: Wikipedia
The Castelo de Sao Jorge, rises above Lisbon. Source: Wikipedia Source: Portugaltravelguide
Source: Portugaltravelguide