This week a group of scientists have published an article which indicates differences between mice and human beings, calling into question the use of these mice in Parkinson’s disease research.
The results could explain way mice do not get Parkinson’s disease, and they may also partly explain why humans do.
In today’s post we will outline the new research, discuss the results, and look at whether Levodopa treatment may (or may not) be a problem.
Much of our understanding of modern biology is derived from the “lower organisms”.
From yeast to snails (there is a post coming shortly on a snail model of Parkinson’s disease – I kid you not) and from flies to mice, a great deal of what we know about basic biology comes from experimentation on these creatures. So much in fact that many of our current ideas about neurodegenerative diseases result from modelling those conditions in these creatures.
Now say what you like about the ethics and morality of this approach, these organisms have been useful until now. And I say ‘until now’ because an interesting research report was released this week which may call into question much of the knowledge we have from the modelling of Parkinson’s disease is these creatures.
You see, here’s the thing: Flies don’t naturally develop Parkinson’s disease.
Nor do mice. Or snails.
Or yeast for that matter.
So we are forcing a very un-natural state upon the biology of these creatures and then studying the response/effect. Which could be giving us strange results that don’t necessarily apply to human beings. And this may explain our long history of failed clinical trials.
We work with the best tools we have, but it those tools are flawed…
What did the new research report find?
This is the study:
Title: Dopamine oxidation mediates mitochondrial and lysosomal dysfunction in Parkinson’s disease Authors: Burbulla LF, Song P, Mazzulli JR, Zampese E, Wong YC, Jeon S, Santos DP, Blanz J, Obermaier CD, Strojny C, Savas JN, Kiskinis E, Zhuang X, Krüger R, Surmeier DJ, Krainc D Journal: Science, 07 Sept 2017 – Early online publication PMID: 28882997
The researchers who conducted this study began by growing dopamine neurons – a type of cell badly affected by Parkinson’s disease – from induced pluripotent stem (IPS) cells.
A recently published research report has caused a bit of a fuss in the media, and I have been contacted by a lot of concerned readers regarding this particular study.
It deals with some chemicals – which can be found in everyday products – that may be having a negative effect on biological processes that are related to Parkinson’s disease – specifically, the normal functioning of the mitochondria (the power stations of each cell).
In today’s post we will discuss the new research, what the chemicals do, and whether the Parkinson’s community should be concerned.
It is something that most of us take completely for granted in the modern world. A product that sits in our bathroom, by the sink or on a shelf, and 2-3 times per day we stick some of it in our mouth and brush it around a bit. Given the well ingrained habit of repetitively ingesting of the stuff, we have little trouble with the idea of switching brands or trying new variations (“Oooh look, this one will make your teeth whiter. Let’s try it”).
I mean, come on – it’s just toothpaste. It’s safe, right?
It probably won’t surprise many of you to learn that the composition of toothpaste has changed quite a bit over the years, but what might amaze you is just how many years are involved with that statement:
The Egyptians recognised the importance of looking after one’s teeth at a very early stage. Apparently they had a lot of trouble with their teeth because their bread had grit in it which wore away their enamel. As far back as 5000BC, they had a form of toothpaste that they used to clean their teeth. It was a mix of powdered ashes of ox hooves, myrrh, powdered and burnt eggshells, and pumice (Source: Wikipedia). The Greeks, followed by the Romans, improved on the recipes (by adding abrasive ingredients such as crushed bones and oyster shells – delightful, huh?), but it wasn’t until after World War I that the modern day pre-mixed toothpastes became popular.
The cavity fighting chemical, Fluoride, was first added to toothpastes in the 1890s, and in 1908 Newell Sill Jenkins (an American dentist) invented the first toothpaste that contained disinfectants. It was called Kolynos (from the Greek words Kolyo nosos (κωλύω νόσος), meaning “disease prevention”).
Following the advent of Kolynos, most toothpaste companies added antiseptic and disinfectant agents to improve the quality and effectiveness of their product. Being offered a tooth cleaning product with magical antibiotic properties seemed to reassure consumers that they were buying something that might actually work. And this led to more and more chemicals being added to toothpaste. Such additions included chemical like triclosan, cetylpyridinium chloride and benzalkonium chloride.
This week a biotech company called Voyager Therapeutics announced the results of their ongoing phase Ib clinical trial. The trial is investigating a gene therapy approach for people with severe Parkinson’s disease.
Gene therapy is a technique that involves inserting new DNA into a cell using a virus. The DNA can help the cell to produce beneficial proteins that go on help to alleviate the motor features of Parkinson’s disease.
In today’s post we will discuss gene therapy, review the new results and consider what they mean for the Parkinson’s community.
On 25th August 2012, the Voyager 1 space craft became the first human-made object to exit our solar system.
After 35 years and 11 billion miles of travel, this explorer has finally left the heliosphere (which encompasses our solar system) and it has crossed into the a region of space called the heliosheath – the boundary area that separates our solar system from interstellar space. Next stop on the journey of Voyager 1 will be the Oort cloud, which it will reach in approximately 300 yearsand it will take the tiny craft about 30,000 years to pass through it.
Where is Voyager actually going? Well, eventually it will pass within 1 light year of a star called AC +79 3888 (also known as Gliese 445), which lies 17.6 light-years from Earth. It will achieve this goal on a Tuesday afternoon in 40,000 years time.
Remarkably, the Gliese 445 star itself is actually coming towards us. Rather rapidly as well. It is approaching with a current velocity of 119 km/sec – nearly 7 times as fast as Voyager 1 is travelling towards it (the current speed of the craft is 38,000 mph (61,000 km/h).
Interesting, but what does any of that have to do with Parkinson’s disease?
Well closer to home, another ‘Voyager’ is also ‘going boldly where no man has gone before’ (sort of).
Dopamine agonist treatments are associated with approximately 90% of hyper-sexuality and compulsive gambling cases that occur in people with Parkinson’s disease.
This issue does not affect everyone being treated with this class of drugs, but it is a problem that keeps popping up, with extremely damaging consequences for the affected people who gamble away their life’s saving or ruin their marriages/family life.
The U.S. Food and Drug Administration (FDA) is yet to issue proper warning for this well recognised side-effect of dopamine agonists, and yet last week they gave clearance for the clinical testing of a new implantable device that will offer continuous delivery of dopamine agonist medication.
In today’s post, we will discuss what dopamine agonists are, the research regarding the impulsive behaviour associated with them, and why the healthcare regulators should acknowledge that there is a problem.
Before we start talking about dopamine agonists, let’s start at the very beginning:
What is dopamine?
By the time a person is sitting in front of a neurologist and being told that they ‘have Parkinson’s disease’, they will have lost half the dopamine producing cells in an area of the brain called the midbrain.
Dopamine is a chemical is the brain that plays a role in many basic functions of the brain, such as motor co-ordination, reward, and memory. It works as a signalling molecule (or a neurotransmitter) – a way for brain cells to communicate with each other. Dopamine is released from brain cells that produce this chemical (not all brain cells do this), and it binds to target cells, initiating biological processes within those cells.
Dopamine being released by one cell and binding to receptors on another. Source: Truelibido
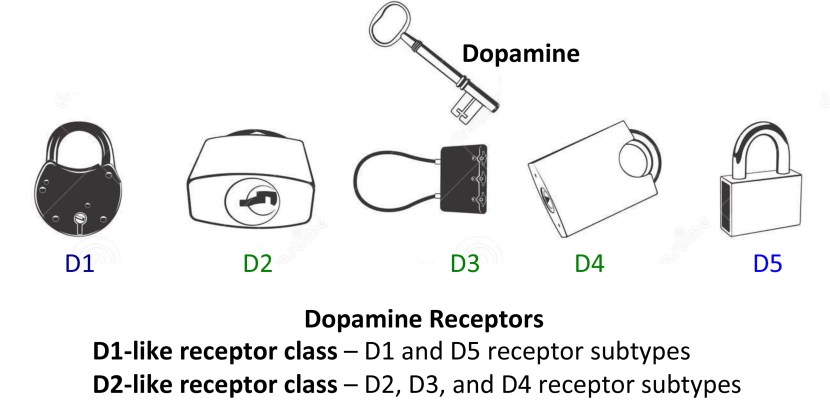
Dopamine binds to target cells via five different receptors – that is to say, dopamine is released from one cell and can bind to one of five different receptors on the target cell (depending on which receptor is present). The receptor is analogous to a lock and dopamine is the key. When dopamine binds to a particular receptor it will allow something to happen in that cell. And this is how information from a dopamine neuron is passed or transmitted on to another cell.
In this post we discuss several recently published research reports suggesting that Parkinson’s disease may be an autoimmune condition. “Autoimmunity” occurs when the defence system of the body starts attacks the body itself.
This new research does not explain what causes of Parkinson’s disease, but it could explain why certain brain cells are being lost in some people with Parkinson’s disease. And such information could point us towards novel therapeutic strategies.
The journal Nature was first published on 4th November 1869, by Alexander MacMillan. It hoped to “provide cultivated readers with an accessible forum for reading about advances in scientific knowledge.” It has subsequently become one of the most prestigious scientific journals in the world, with an online readership of approximately 3 million unique readers per month (almost as much as we have here at the SoPD).
Each Wednesday afternoon, researchers around the world await the weekly outpouring of new research from Nature. And this week a research report was published in Nature that could be big for the world of Parkinson’s disease. Really big!
On the 21st June, this report was published:
Title: T cells from patients with Parkinson’s disease recognize α-synuclein peptides Authors: Sulzer D, Alcalay RN, Garretti F, Cote L, Kanter E, Agin-Liebes J, Liong C, McMurtrey C, Hildebrand WH, Mao X, Dawson VL, Dawson TM, Oseroff C, Pham J, Sidney J, Dillon MB, Carpenter C, Weiskopf D, Phillips E, Mallal S, Peters B, Frazier A, Lindestam Arlehamn CS, Sette A Journal:Nature. 2017 Jun 21. doi: 10.1038/nature22815. PMID: 28636593
In their study, the investigators collected blood samples from 67 people with Parkinson’s disease and from 36 healthy patients (which were used as control samples). They then exposed the blood samples to fragments of proteins found in brain cells, including fragments of alpha synuclein – this is the protein that is so closely associated with Parkinson’s disease (it makes regular appearances on this blog).
What happened next was rather startling: the blood from the Parkinson’s patients had a strong reaction to two specific fragments of alpha synuclein, while the blood from the control subjects hardly reacted at all to these fragments.
In the image below, you will see the fragments listed along the bottom of the graph (protein fragments are labelled with combinations of alphabetical letters). The grey band on the plot indicates the two fragments that elicited a strong reaction from the blood cells – note the number of black dots (indicating PD samples) within the band, compared to the number of white dots (control samples). The numbers on the left side of the graph indicate the number of reacting cells per 100,000 blood cells.
The investigators concluded from this experiment that these alpha synuclein fragments may be acting as antigenic epitopes, which would drive immune responses in people with Parkinson’s disease and they decided to investigate this further.
Personal story: I was at the Dopamine 2016 conference in September last year in lovely Vienna (Austria). Wonderful city, beautiful weather, and an amazing collection of brilliant researchers focused on all things dopamine-related. The conference really highlighted all the new research being done on this chemical.
There was – of course – a lots of research being presented on Parkinson’s disease, given that dopamine plays such an important role in the condition.
And it was all really interesting.
Anyways, I was sitting in one of the lecture presentation session, listening to all these new results being discussed.
And then, a lady from Carnegie Mellon University stood up and (without exaggeration) completely – blew – my – mind!
She is an Assistant Professor in the Department of Biological Sciences at Carnegie Mellon University, where her group investigates the neural circuits underlying the regulation of movement, learning, motivation, and reward.
And the ‘mind blowing‘ research that she presented in Vienna has recently been published in the journal Nature Neuroscience:
In this report, Dr Gittis and her colleagues demonstrated that elevating the activity of one type of cell in an area of the brain called the globus pallidus, could provide long lasting relief from Parkinson’s-like motor features.
Hang on a second. What is the globus pallidus?
The globus pallidus is a structure deep in the brain and before Dr Gittis and her colleagues published their research, we already knew it played an important role in our ability to move.
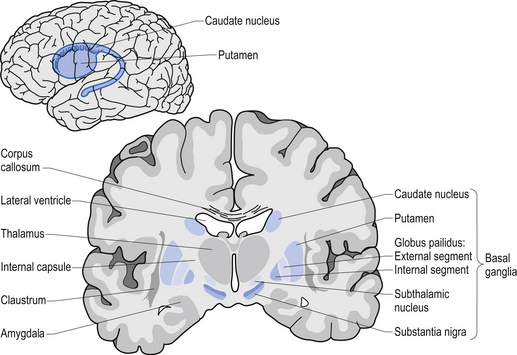
Movement is largely controlled by the activity in a specific group of brain regions, collectively known as the ‘Basal ganglia‘.
The basal ganglia structures (blue) in the human brain. Source: iKnowledge
But while the basal ganglia controls movement, it is not the starting point for the movement process.
The prefrontal cortex is where we do most of our ‘thinking’. It is the part of the brain that makes decisions with regards to many of our actions, particularly voluntary movement. It is involved in what we call ‘executive functions’. It is the green area in the image below.
Now the prefrontal cortex might come up with an idea: ‘the left hand should start to play the piano’. The prefrontal cortex will communicate this idea with the premotor cortex and together they will send a very excited signal down into the basal ganglia for it to be considered. Now in this scenario it might help to think of the cortex as hyperactive, completely out of control toddlers, and the basal ganglia as the parental figure. All of the toddlers are making demands/proposals and sending mixed messages, and it is for the inhibiting basal ganglia to gain control and decide which is the best.
So the basal ganglia receives signals from the cortex, processes that information before sending a signal on to another important participant in the regulation of movement: the thalamus.
A brain scan illustrating the location of the thalamus in the human brain. Source: Wikipedia
The thalamus is a structure deep inside the brain that acts like the central control unit of the brain. Everything coming into the brain from the spinal cord, passes through the thalamus. And everything leaving the brain, passes through the thalamus. It is aware of most everything that is going on and it plays an important role in the regulation of movement. If the cortex is the toddler and the basal ganglia is the parent, then the thalamus is the ultimate policeman.
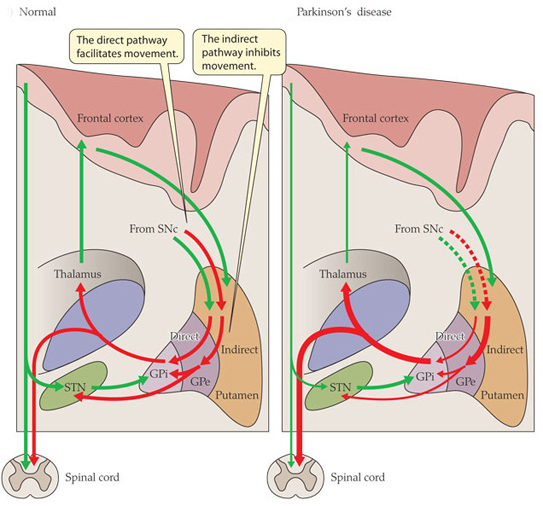
Now to complicate things for you, the processing of movement in the basal ganglia involves a direct pathway and an indirect pathway. In the simplest terms, the direct pathway encourages movement, while the indirect pathway does the opposite: inhibits it.
The thalamus will receive signals from the two pathways and then decide – based on those signals – whether to send an excitatory or inhibitory message to the primary motor cortex, telling it what to do (‘tell the muscles to play the piano’ or ‘don’t start playing the piano’, respectively). The primary motor cortex is the red stripe in the image below.
The primary motor cortex then sends this structured order down the spinal cord (via the corticospinal pathway) and all going well the muscles will do as instructed.
Now, in Parkinson’s disease, the motor features (slowness of movement and resting tremor) are associated with a breakdown in the processing of those direct and an indirect pathways. This breakdown results in a stronger signal coming from the indirect pathway – thus inhibiting/slowing movement. This situation results from the loss of dopamine in the brain.
Excitatory signals (green) and inhibitory signals (red) in the basal ganglia, in both a normal brain and one with Parkinson’s disease. Source: Animal Physiology 3rd Edition
Under normal circumstances, dopamine neurons release dopamine in the basal ganglia that helps to mediate the local environment. It acts as a kind of lubricant for movement, the oil in the machine if you like. It helps to reduce the inhibitory bias of the basal ganglia.
Thus, with the loss of dopamine neurons in Parkinson’s disease, there is an increased amount of activity coming out of the indirect pathway.
And as a result, the thalamus is kept in an overly inhibited state. With the thalamus subdued, the signal to the motor cortex is unable to work properly. And this is the reason why people with Parkinson’s disease have trouble initiating movement.
Now, as you can see from the basic schematic above, the globus pallidus is one of the main conduits of information into the thalamus. Given this pivotal position in the regulation of movement, the globus pallidus has been a region of major research focus for a long time.
It is also one of the sites targeted in ‘deep brain stimulation’ therapy for Parkinson’s disease (the thalamus being another target). Deep brain stimulation (or DBS) involves placing electrodes deep into the brain to help regulate activity.
By regulating the level of activity in the globus pallidus, DBS can control the signal being sent to the thalamus, reducing the level of inhibition, and thus alleviating the motor related features of the Parkinson’s disease.
The dramatic effects (and benefits) of deep brain stimulation can be seen in this video (kindly provided by fellow kiwi Andrew Johnson):
Deep brain stimulation is not perfect, however.
The placing of the electrodes can sometimes be off target, resulting in limited beneficial effects. Plus the tuning of the device can be a bit fiddly in some cases.
A more precise method of controlling the globus pallidus would be ideal.
Ok, so the globus Pallidus region of the brain is important for movement. What did Dr Gittis and her colleagues find in their research?
They used an amazing piece of technology called ‘optogenetics‘ to specifically determine which group of cells in the globus pallidus are involved in the inhibitory signals going to the thalamus.
And their results are VERY interesting.
But what is optogenetics?
Good question.
The short answer: ‘Magic’
The long answer: In 1979, Nobel laureate Francis Crick suggested that one of the major challenge facing the study of the brain was the need to control one type of cell in the brain while leaving others unaltered.
The DNA duo: Francis Crick (left) and James Watson. Source: CNN
Electrical stimulation cannot address this challenge because electrodes stimulate everything in the immediate vicinity without distinction. In addition the signals from electrodes lack precision; they cannot turn on/off neurons as dynamically as we require. The same problems (and more) apply to the use of drugs.
Crick later speculated that the answer might be light.
How on earth would you do that?
Well, in 1971 – eight years before Crick considered the problem – two researchers, Walther Stoeckenius and Dieter Oesterhelt, discovered a protein, bacteriorhodopsin, which acts as an ion pump on the surface of a cell membrane. Amazingly, this protein can briefly become activated by green light.
A rather remarkable property.
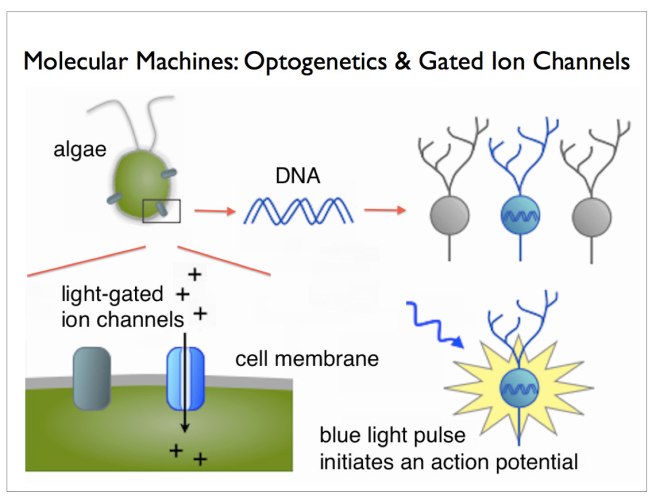
Later, other groups found similar proteins. One such protein, called ‘Channelrhodopsin’, was discovered in green algae (click here to read more on this). When stimulated by particular frequencies of light, these channels open up on the cell surface and allow ions to pass through. If enough channels open, this process can stimulate particular activity in the cell.
Looks like the mad scientist type, right? Well, remember his name, because this guy is fast heading for a Nobel prize.
He’s awesome!
He is the D. H. Chen Professor of Bioengineering and of Psychiatry and Behavioral Sciences at Stanford University. And he is one of the leading researchers in a field that he basically started.
Back in 2005, he and his collaborators published this research report:
Title: Millisecond-timescale, genetically targeted optical control of neural activity Authors: Boyden ES, Zhang F, Bamberg E, Nagel G, Deisseroth K. Journal: Nat Neurosci. 2005 Sep;8(9):1263-8. Epub 2005 Aug 14. PMID:16116447
In this research report, Deisseroth and his colleagues (particularly Ed Boyden, lead author and now a professor of Biological Engineering at the McGovern Institute for Brain Research at MIT) took the short section of DNA that provides the instructions for making Channelrhodopsin from green algae and they put that piece of DNA into neurons.
And when they then shined blue light on the neurons, guess what happened? Yes, the neurons became activated – that is to say, they produced an ‘action potential’, which is one of the way information is passed from one neuron to another.
And the best part of this biological manipulation was that Deisseroth and his colleagues could activate the neurons with absolutely amazing precision! By pulsing light on the cells for just millisecond periods, they could elicit instant action potentials:
Precise control of the firing of a neuron. Source: Frontiers
And of course any surrounding cells that do not have the Channelrhodopsin DNA were not affected by the light, but were activated by the signal coming from the Channelrhodopsin+ cells.
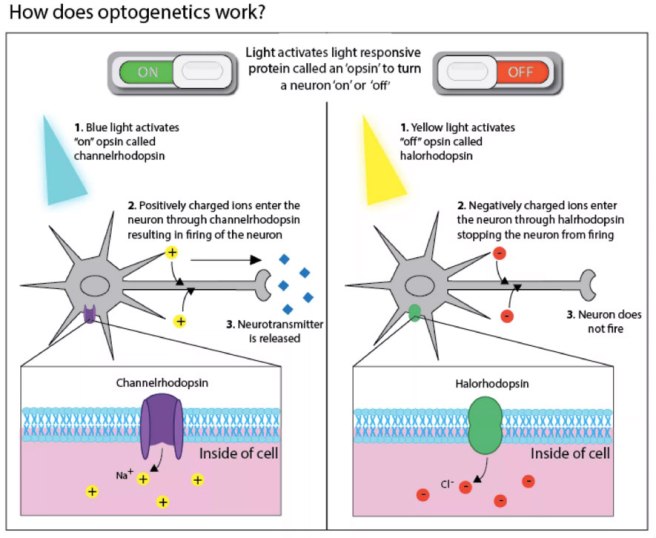
This original research report lead to a gold rush-like search for other proteins that are light activated, and we now have an ever increasing toolbox of new proteins with curious properties. For example, we can now not only turn on neurons, but we also have proteins that can shut their activity down, blocking any action potentials (with proteins called ‘Halorhodopsin’ – click here for more on this). And many of these proteins are activated by different frequencies of light. It is really remarkable biology.
For an excellent first-hand history of the early development of optogenetics (written by Ed Boydon who worked with Diesseroff on the first optogenetics study) – click here.
Two years after the first report of optogenetics, the first research demonstrating the use of this technology in the brain of a live animal was published (Click here and here to read more on this). And these fantastic tools are not just being used in the brain, they are being applied to tissues all over the body (for example, optogenetics can be used to make heart cells beat – click here to read more on this).
This TED talk video of Ed Boyden’s description of optogenetics is worth watching if you want to better understand the technique and to learn more about it:
Ok, so Dr Gittis and her colleagues used optogenetics in their research. What did they find?
Well, from previous research they knew that there were two types of neurons in the globus pallidus that regulate a lot of the activity in this region. The two types were identifiable by two different proteins: Lim homeobox 6 (Lhx6) and Parvalbumin (PV).
The Lhx6 neurons, which do not have any PV protein, are generally concentrated in the medial portion of the globus pallidus (closer to the centre of the brain). These Lhx6 neurons also have strong connections with the striatum and substantia nigra parts of the brain. The PV neurons, on the other hand, are more concentrated in the lateral portions of the globus pallidus (closer to the side of the brain), and they have strong connections with the thalamus (Click here to read this previous research).
In their new research report, Dr Gittis and her colleagues have used optogenetics to determine the functions of these two types of cells in the globus pallidus.
Initially, they stimulated both Lhx6 and PV neurons at the same time to see if they could restore movement in mice that had been treated with a neurotoxin (6-OHDA) that killed all the dopamine neurons. Unfortunately, they saw no rescue of the motor abilities of the mice.
They next shifted their attention to activating the two groups of cells separately to see if one of them was inhibiting the other. And when they stimulated the PV neurons alone, something amazing happened: the mice basically got up and started moving.
But the really mind blowing part: even after they turned off the stimulating light – after the pulse of light stopped – the mice were still able to keep moving around.
And this effect lasted for several hours! (note that the red line – indicating a decrease in immobility – in the image below remains stable after the stimulation of light pulses – blue lines – has stopped. Even between light pulses the mouse doesn’t return to immobility).
Stimulation of the PV neurons. Source: Nature
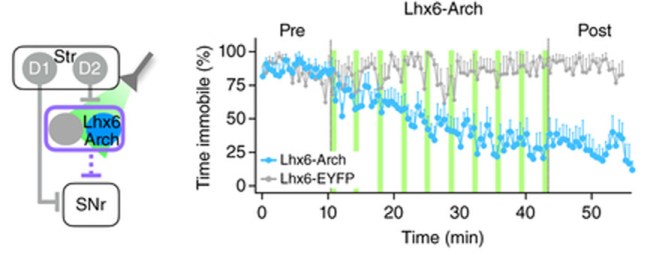
The investigators then tested the reverse experiment: inhibiting the Lhx6 neurons.
And guess what?
They found that by inhibiting the Lhx6 neurons with pulses of light, they could restore movement in the dopamine-depletedmice (and again for hours beyond stimulation – note the blue line in the image below remains even after the light pulses – green lines – have stopped).
Inhibiting of the Lhx6 neurons. Source: Nature
This result blew my mind at the conference in Vienna. And even now as I write this, I am still….well, flabbergasted! (there’s a good word).
In addition to being a very elegant experiment and use of this new optogenetic technology, this study opens new doors for us in the Parkinson’s disease research field regarding our understanding of how movement works and how we can now potentially treat PD.
A company in Ann Arbor (Michigan) called RetroSense Therapeutics announced in March of 2016 that they had treated their first subject in a Phase I/IIa, open-label, dose-escalation clinical study of the safety and tolerability of their lead product, RST-001 in patients with retinitis pigmentosa (Click here for the press release).
Retinitis pigmentosa is an inherited eye disease that causes severe vision impairment due to the progressive degeneration of the rodphotoreceptor cells in the retina. The condition starts with patients experiencing progressive “tunnel vision” and eventual leads to blindness.
RetroSense’s lead product, RST-001 is basically a virus that infects cells with the photosensitivity gene, channelrhodopsin-2, that we discussed above. Several studies have demonstrated the ability of this approach to restore the perception of light and even vision in experimental models of blindness (Click here to read more about this).
The therapy involves injecting RST-001 into the retinas of patients who are blind. The infected cells will then fire when stimulated with blue light coming into the eye, and this information will hopefully be passed on to the brain. All going well, RetroSense plans to enroll 15 blind subjects in its trial, and they will follow them for two years. They hope to release some preliminary data, however, later this year. And a lot of people will be watching this trial and waiting for the results.
So, yes, optogenetics is being tested in humans.
Obviously, however, these are the first tentative steps in this new field. And it may be sometime before the medical regulatory bodies allow researchers to start conducting optogentic trials in the brain, let alone on people with Parkinson’s disease.
What does it all mean?
It is always rather wondrous where new discoveries take us.
A little over 10 years ago, some scientists discovered that by inserting a photosensitivity gene into brain cells they could control the firing of those cells with rapid pulses of light. And now other researchers are using that technology not only to better understand the works of our brains and how we move, but also to help make blind people see again.
Whether this technology will be able to replace therapies like deep brain stimulation with a more precise method of controlling the firing of the globus pallidus, is yet yo be seen. But this amazing new technique in our research toolbox will most certainly help to enhance our understanding of Parkinson’s disease. Taking us one step closer to ridding ourselves of it entirely.
The banner for today’s post was sourced from Scientifica
Last week scientists in Sweden published research demonstrating a method by which the supportive cells of the brain (called astrocytes) can be re-programmed into dopamine neurons… in the brain of a live animal!
It was a really impressive trick and it could have major implications for Parkinson’s disease.
In today’s post is a long read, but in it we will review the research leading up to the study, explain the science behind the impressive feat, and discuss where things go from here.
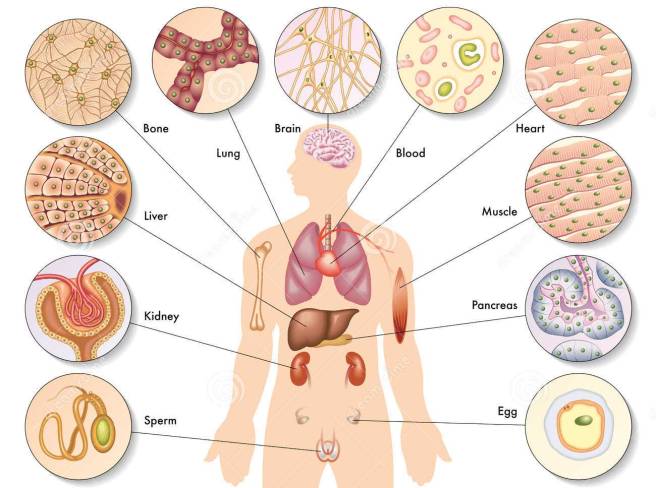
Different types of cells in the body. Source: Dreamstime
In your body at this present moment in time, there is approximately 40 trillion cells (Source).
The vast majority of those cells have developed into mature types of cell and they are undertaking very specific functions. Muscle cells, heart cells, brain cells – all working together in order to keep you vertical and ticking.
Now, once upon a time we believed that the maturation (or the more technical term: differentiation) of a cell was a one-way street. That is to say, once a cell became what it was destined to become, there was no going back. This was biological dogma.
But more importantly, in 2006 he published a research report demonstrating how someone could take a skin cell and re-program it so that was now a stem cell – capable of becoming any kind of cell in the body.
Here’s the study:
Title: Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Authors: Takahashi K, Yamanaka S. Journal: Cell. 2006 Aug 25;126(4):663-76. PMID:16904174 (This article is OPEN ACCESS if you would like to read it)
Shinya Yamanaka‘s team started with the hypothesis that genes which are important to the maintenance of embryonic stem cells (the cells that give rise to all cells in the body) might also be able to cause an embryonic state in mature adult cells. They selected twenty-four genes that had been previously identified as important in embryonic stem cells to test this idea. They used re-engineered retroviruses to deliver these genes to mouse skin cells. The retroviruses were emptied of all their disease causing properties, and could thus function as very efficient biological delivery systems.
The skin cells were engineered so that only cells in which reactivation of the embryonic stem cells-associated gene, Fbx15, would survive the testing process. If Fbx15 was not turned on in the cells, they would die. When the researchers infected the cells with all twenty-four embryonic stem cells genes, remarkably some of the cells survived and began to divide like stem cells.
In order to identify the genes necessary for the reprogramming, the researchers began removing one gene at a time from the pool of twenty-four. Through this process, they were able to narrow down the most effective genes to just four: Oct4, Sox2, cMyc, and Klf4, which became known as the Yamanaka factors.
This new type of cell is called an induced pluripotent stem (IPS) cell – ‘pluripotent’ meaning capable of any fate.
The discovery of IPS cells turned biological dogma on it’s head.
And in acknowledgement of this amazing bit of research, in 2012 Prof Yamanaka and Prof John Gurdon (University of Cambridge) were awarded the Nobel prize for Physiology and Medicine for the discovery that mature cells can be converted back to stem cells.
Prof Gurdon achieved the feat in 1962 when he removed the nucleus of a fertilised frog egg cell and replaced it with the nucleus of a cell taken from a tadpole’s intestine. The modified egg cell then grew into an adult frog! This fascinating research proved that the mature cell still contained the genetic information needed to form all types of cells.
EDITOR’S NOTE: We do not want to be accused of taking anything away from Prof Gurdon’s contribution to this field (which was great!) by not mentioning his efforts here. For the sake of saving time and space, we are focusing on Prof Yamanaka’s research as it is more directly related to today’s post.
This amazing discovery has opened new doors for biological research and provided us with incredible opportunities for therapeutic treatments. For example, we can now take skins cells from a person with Parkinson’s disease and turn those cells into dopamine neurons which can then be tested with various drugs to see which treatment is most effective for that particular person (personalised medicine in it’s purest form).
Some of the option available to Parkinson’s disease. Source: Nature
Imagination is literally the only limiting factor with regards to the possible uses of IPS cell technology.
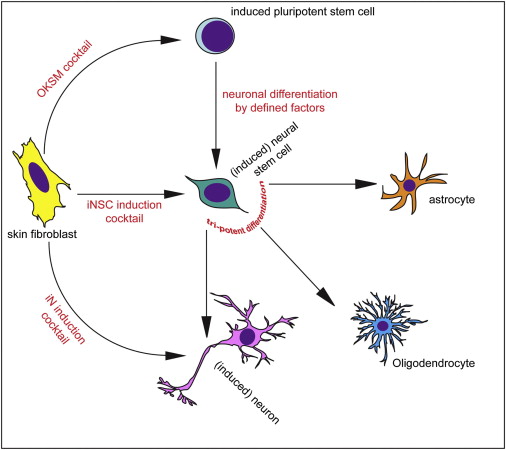
Shortly after Yamanaka’s research was published in 2006, however, the question was asked ‘rather than going back to a primitive state, can we simply change the fate of a mature cell directly?’ For example, turn a skin cell into a neuron.
This question was raised mainly to address the issue of ‘age’ in the modelling disease using IPS cells. Researchers questioned whether an aged mature cell reprogrammed into an immature IPS cell still carried the characteristics of an aged cell (and can be used to model diseases of the aged), or would we have to wait for the new cell to age before we can run experiments on it. Skin biopsies taken from aged people with neurodegenerative conditions may lose the ‘age’ element of the cell and thus an important part of the personalised medicine concept would be lost.
So researchers began trying to ‘re-program’ mature cells. Taking a skin cell and turning it directly into a heart cell or a brain cell.
And this is probably the craziest part of this whole post because they actually did it!
Different methods of inducing skin cells to become something else. Source: Neuron
In 2010, scientists from Stanford University published this report:
Title: Direct conversion of fibroblasts to functional neurons by defined factors Authors: Vierbuchen T, Ostermeier A, Pang ZP, Kokubu Y, Südhof TC, Wernig M. Journal: Nature. 2010 Feb 25;463(7284):1035-41. PMID:20107439
In this study, the researchers demonstrated that the activation of three genes (Ascl1, Brn2 and Myt1l) was sufficient to rapidly and efficiently convert skin cells into functional neurons in cell culture. They called them ‘iN’ cells’ or induced neuron cells. The ‘re-programmed’ skin cells made neurons that produced many neuron-specific proteins, generated action potentials (the electrical signal that transmits a signal across a neuron), and formed functional connection (or synapses) with neighbouring cells. It was a pretty impressive achievement, which they beat one year later by converting mature liver cells into neurons – Click here to read more on this – Wow!
The next step – with regards to our Parkinson’s-related interests – was to convert skin cells directly into dopamine neurons (the cells most severely affected in the condition).
And guess what:
Title: Direct conversion of human fibroblasts to dopaminergic neurons. Authors: Pfisterer U, Kirkeby A, Torper O, Wood J, Nelander J, Dufour A, Björklund A, Lindvall O, Jakobsson J, Parmar M Journal:Proc Natl Acad Sci U S A (2011) 108:10343-10348. PMID: 21646515 (This article is OPEN ACCESS if you would like to read it)
In this study, Swedish researchers confirmed that activation of Ascl1, Brn2, and Myt1l re-programmed human skin cells directly into functional neurons. But then if they added the activation of two additional genes, Lmx1a andFoxA2 (which are both involved in dopamine neuron generation), they could convert skin cells directly into dopamine neurons. And those dopamine neurons displayed all of the correct features of normal dopamine neurons.
With the publication of this research, it suddenly seemed like anything was possible and people began make all kinds of cell types out of skin cells. For a good review on making neurons out of skin cells – Click here.
Given that all of this was possible in a cell culture dish, some researchers started wondering if direct reprogramming was possible in the body. So they tried.
And again, guess what:
Title: In vivo reprogramming of adult pancreatic exocrine cells to beta-cells. Authors: Zhou Q, Brown J, Kanarek A, Rajagopal J, Melton DA. Journal: Nature. 2008 Oct 2;455(7213):627-32. PMID:18754011
Using the activation of three genes (Ngn3, Pdx1 and Mafa), the investigators behind this study re-programmed differentiated pancreatic exocrine cells in adult mice into cells that closely resemble b-cells. And all of this occurred inside the animals, while the animals were wandering around & doing their thing!
Now naturally, researchers in the Parkinson’s disease community began wondering if this could also be achieved in the brain, with dopamine neurons being produced from re-programmed cells.
And (yet again) guess what:
Title: Generation of induced neurons via direct conversion in vivo Authors: Torper O, Pfisterer U, Wolf DA, Pereira M, Lau S, Jakobsson J, Björklund A, Grealish S, Parmar M. Journal: Proc Natl Acad Sci U S A. 2013 Apr 23;110(17):7038-43. PMID:23530235 (This article is OPEN ACCESS if you would like to read it)
In this study, the Swedish scientists (behind the previous direct re-programming of skin cells into dopamine neurons) wanted to determine if they could re-program cells inside the brain. Firstly, they engineered skin cells with the three genes (Ascl1, Brn2a, & Myt1l) under the control of a special chemical – only in the presence of the chemical, the genes would be activated. They next transplanted these skin cells into the brains of mice and began adding the chemical to the drinking water of the mice. At 1 & 3 months after transplantation, the investigators found re-programmed cells inside the brains of the mice.
Next, the researchers improved on their recipe for producing dopamine neurons by adding the activation of two further genes: Otx2 and Lmx1b (also important in the development of dopamine neurons). So they were now activating a lot of genes: Ascl1, Brn2a, Myt1l, Lmx1a, FoxA2, Otx2 and Lmx1b. Unfortunately, when these reprogrammed cells were transplanted into the brain, few of them survived to become mature dopamine neurons.
The investigators then ask themselves ‘do we really need to transplant cells? Can’t we just reprogram cells inside the brain?’ And this is exactly what they did! They injected the viruses that allow for reprogramming directly into the brains of mice. The experiment was designed so that the cargo of the viruses would only become active in the astrocyte cells, not neurons. And when the researchers looked in the brains of these mice 6 weeks later, they found numerous re-programmed neurons, indicating that direct reprogramming is possible in the intact brain.
So what was so special about the research published last week about? Why the media hype?
The research published last week, by another Swedish group, took this whole process one step further: Not only did they re-program astrocytes in the brain to become dopamine neurons, but they also did this on a large enough scale to correct the motor issues in a mouse model of Parkinson’s disease.
Here is the study:
Title: Induction of functional dopamine neurons from human astrocytes in vitro and mouse astrocytes in a Parkinson’s disease model Authors: di Val Cervo PR, Romanov RA, Spigolon G, Masini D, Martín-Montañez E, Toledo EM, La Manno G, Feyder M, Pifl C, Ng YH, Sánchez SP, Linnarsson S, Wernig M, Harkany T, Fisone G, Arenas E. Journal: Nature Biotechnology (2017) doi:10.1038/nbt.3835 PMID:28398344
These researchers began this project 6 years ago with a new cocktail of genes for reprogramming cells to become dopamine neurons. They used the activation of NEUROD1, ASCL1 and LMX1A, and a microRNA miR218 (microRNAs are genes that produce RNA, but not protein – click here for more on this). These genes improved the reprogramming efficiency of human astrocytes to 16% (that is the percentage of astrocytes that were infected with the viruses and went on to became dopamine neurons). The researchers then added some chemicals to the reprogramming process that helps dopamine neurons to develop in normal conditions, and they observed an increase in the level of reprogramming to approx. 30%. And these reprogrammed cells display many of the correct properties of dopamine neurons.
Next the investigators decided to try this conversion inside the brains of mice that had Parkinson’s disease modelled in them (using a neurotoxin). The delivery of the viruses into the brains of these mice resulted in reprogrammed dopamine neurons beginning to appear, and 13 weeks after the viruses were delivered, the researchers observed improvements in the Parkinson’s disease related motor symptoms of the mice. The scientists concluded that with further optimisation, this reprogramming approach may enable clinical therapies for Parkinson’s disease, by the delivery of genes rather than transplanted cells.
How does this reprogramming work?
As we have indicated above, the re-programming utilises re-engineered viruses. They have been emptied of their disease causing elements, allowing us to use them as very efficient biological delivery systems. Importantly, retroviruses infect dividing cells and integrate their ‘cargo’ into the host cell’s DNA.
Retroviral infection and intergration into DNA. Source: Evolution-Biology
The ‘cargo’ in the case of IPS cells, is a copy of the genes that allow reprogramming (such as the Yamanaka genes), which the cell will then start to activate, resulting in the production of protein for those genes. These proteins subsequently go on to activate a variety of genes required for the maintenance of embryonic stem cells (and re-programming of mature cells).
And viruses were also used for the re-programming work in the brain as well.
There is the possibility that one day we will be able to do this without viruses – in 2013, researchers made IPS cells using a specific combination of chemicals (Click here to read more about this) – but at the moment, viruses are the most efficient biological targeting tool we have.
So what does it all mean?
Last week researchers is Sweden published research explaining how they reprogrammed some of the helper cells in the brains of Parkinsonian mice so that they turned into dopamine neurons and helped to alleviate the symptoms the mice were feeling.
This result and the trail of additional results outlined above may one day be looked back upon as the starting point for a whole new way of treating disease and injury to particular organs in the body. Suddenly we have the possibility of re-programming cells in our body to under take a new functions to help combat many of the conditions we suffer.
It is important to appreciate, however, that the application of this technology is still a long way from entering the clinic (a great deal of optimisation is required). But the fact that it is possible and that we can do it, raises hope of more powerful medical therapies for future generations.
As the researchers themselves admit, this technology is still a long way from the clinic. Improving the efficiency of the technique (both the infection of the cells and the reprogramming) will be required as we move down this new road. In addition, we will need to evaluate the long-term consequences of removing support cells (astrocytes) from the carefully balanced system that is the brain. Future innovations, however, may allow us to re-program stronger, more disease-resistant dopamine neurons which could correct the motor symptoms of Parkinson’s disease without being affected by the disease itself (as may be the case in transplanted cells – click here to read more about this).
Watch for a lot more research coming from this topic.
The banner for today’s post was sourced from Greg Dunn (we love his work!)
The chemical dopamine plays a critical role in Parkinson’s disease.
It is also involved with the condition Attention deficit hyperactivity disorder, and recently researchers have been looking at whether there are any links between the two.
In today’s post we will look at what Attention deficit hyperactivity disorder is, how it relates to Parkinson’s disease, and what new research means for the community.
We really have little idea about how Parkinson’s disease actually develops.
It could be kicked off by a virus or environmental factors or genetics…or perhaps a combination of these. We really don’t know, and it could vary from person to person.
There is a lot of speculation, however, as to what additional conditions could make one susceptible to Parkinson’s disease, even those conditions with early developmental onsets, such as autism (which we have previously written about – click here to see that post).
Recently researchers in Germany have asked if there is any connections between Parkinson’s and ADHD?
What is ADHD?
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental condition that begins in childhood and persists into adulthood in 60% of affected individuals.
It is classically characterised in the media by hyperactive children who struggle to concentrate and stay focused on what they are doing. They are often treated with drugs such as Methylphenidate (also known as ritalin). Methylphenidate acts by blocking a protein called the dopamine transporter, which is involved with reabsorbing the chemical dopamine back into the cell after it has performed it’s function.
So are there any connections between ADHD and Parkinson’s disease?
This is an interesting question.
While there have been no reported findings of increased (or decreased) frequency of Parkinson’s disease in people with ADHD (to our knowledge), there are actually several bits of evidence suggesting a connection between the two conditions, such as abnormalities in the substantia nigra:
Title: Structural abnormality of the substantia nigra in children with attention-deficit hyperactivity disorder Authors: Romanos M, Weise D, Schliesser M, Schecklmann M, Löffler J, Warnke A, Gerlach M, Classen J, Mehler-Wex C. Journal: J Psychiatry Neurosci. 2010 Jan;35(1):55-8. PMID:20040247 (This article is OPEN ACCESS if you would like to read it)
The substantia nigra is a structure in the brain where the dopamine neurons reside. In Parkinson’s disease, the dopamine neurons of the substantia nigra start to degenerate – 50% are lost by the time a person is diagnosed with the condition.
In this study, the researchers used a technique called echogenicity to examine the substantia nigra of 22 children with ADHD and 22 healthy controls. Echogenicity is the ‘ability to bounce an echo’. This sort of assessment measures the return of an ultrasound signal that is aimed at a structure.
The researchers found that the ADHD subjects had a larger substantia nigra area than the healthy controls – which apparently indicates dopamine dysfunction. This finding is similar to results that have been observed in Parkinson’s disease (Click here to read more regarding that study).
Another connection between the two conditions was recent research has shown that genetic variations in the PARK2 gene (also known as Parkin) contribute to the genetic susceptibility to ADHD.
Title: Genome-wide analysis of rare copy number variations reveals PARK2 as a candidate gene for attention-deficit/hyperactivity disorder. Authors: Jarick I, Volckmar AL, Pütter C, Pechlivanis S, Nguyen TT, Dauvermann MR, Beck S, Albayrak Ö, Scherag S, Gilsbach S, Cichon S, Hoffmann P, Degenhardt F, Nöthen MM, Schreiber S, Wichmann HE, Jöckel KH, Heinrich J, Tiesler CM, Faraone SV, Walitza S, Sinzig J, Freitag C, Meyer J, Herpertz-Dahlmann B, Lehmkuhl G, Renner TJ, Warnke A, Romanos M, Lesch KP, Reif A, Schimmelmann BG, Hebebrand J, Scherag A, Hinney A. Journal: Mol Psychiatry. 2014 Jan;19(1):115-21. PMID:23164820 (This article is OPEN ACCESS if you would like to read it)
There are about 20 genes that have been associated with Parkinson’s disease, and they are referred to as the PARK genes. Approximately 10-20% of people with Parkinson’s disease have a genetic variation in one or more of these PARK genes (we have discussed these before – click here to read that post). PARK2 is a gene called Parkin. Mutations in Parkin can result in an early-onset form of Parkinson’s disease. The Parkin gene produces a protein which plays an important role in removing old or sick mitochondria (we discussed this in our previous post – click here to read that post).
In this report, the researchers conducted a genetic sequencing study on 489 young subjects with ADHD (average age 11 years old) and 1285 control individuals. They replicated the study with a similar sized population of people affected by ADHD and control subjects, and in both studies they found that certain deletions and replications in the Parkin gene influences susceptibility to ADHD – two of the genetic variations were found in 335 of the ADHD cases and none in 2026 healthy controls (from both sets of studies).
So there are are some interesting possible connections between ADHD and Parkinson’s disease.
And what has the recent research from the German scientists found?
In this study, the researchers have looked at additional genetic variations that have been suggested to infer susceptibility to ADHD.
Title: No genetic association between attention-deficit/hyperactivity disorder (ADHD) and Parkinson’s disease in nine ADHD candidate SNPs Authors: Geissler JM; International Parkinson Disease Genomics Consortium members., Romanos M, Gerlach M, Berg D, Schulte C. Journal: Atten Defic Hyperact Disord. 2017 Feb 7. doi: 10.1007/s12402-017-0219-8. [Epub ahead of print] PMID:28176268
The researchers analysed nine genetic variations in seven genes:
one variant in the gene synaptosomal-associated protein, 25kDa1 (SNAP25)
one variant in the gene dopamine transporter (DAT; also known as SLC6A3)
one variant in the gene dopamine receptor D4 (DRD4)
one variant in the gene serotonin receptor 1B (HTR1B)
three mutations in cadherin 13 (CDH13)
one mutation located within the gene tryptophan hydroxylase 2 (TPH2)
one mutation located within the gene noradrenaline transporter (SLC6A2)
These genetic variations were assessed in 5333 cases of Parkinson’s disease and 12,019 healthy controls. The researchers found no association between any of the genetic variants and Parkinson’s disease. This finding lead the investigators to conclude that these genetic alterations associated with ADHD do not play a substantial role in increasing the risk of developing Parkinson’s disease.
Have ADHD medications ever been tested in Parkinson’s disease?
Yes.
Given the association of both ADHD and Parkinson’s disease with altered dopamine processing in the brain, a clinical trial of ritalin in Parkinson’s disease was set up and run in 2006 (Click here to read more about that trial). The results of the trial were published in 2007:
Title: Effects of methylphenidate on response to oral levodopa: a double-blind clinical trial. Authors: Nutt JG, Carter JH, Carlson NE. Journal: Arch Neurol. 2007 Mar;64(3):319-23. PMID:17353373 (This article is OPEN ACCESS if you would like to read it)
In this study, the researchers recruited 12 people with Parkinson’s disease and examined their response to 0.4 mg/kg of ritalin – given 3 times per day – in conjunction with their normal anti-Parkinsonian medication (L-dopa). They then tested the subjects with either ritalin or a placebo control and failed to find any clinically significant augmentation of L-dopa treatment from the co-administration of ritalin.
What does it all mean?
So summing up: both Attention deficit hyperactivity disorder (ADHD) and Parkinson’s disease are associated with changes in the processing of the brain chemical dopamine. There are loose connections between the two conditions, but nothing definitive.
It will be interesting to follow up some of the individuals affected by ADHD, to determine if they ultimately go on to develop Parkinson’s (particularly those with Parkin mutations/genetic variants). But until then, the connection between these two conditions is speculative at best.
The banner for today’s post was sourced from Youtube
INTERESTING RESEARCH FINDING 1: People with Parkinson’s disease eat more chocolate than people without Parkinson’s.
INTERESTING RESEARCH FINDING 2: This difference is specific to chocolate. There is no difference in the consumption of other forms of sugary treats between the two populations.
Today’s post deals with a topic very dear to me and it’s relationship with Parkinson’s disease.
Everyone likes chocolate, especially at this time of the year. Curious thing is though, people with Parkinson’s seem to like chocolate even more than non-Parkinsonian people.
Why is that? We’re not sure. But some interesting research has been conducted on chocolate and Parkinson’s disease, which we shall review in this post.
But first:
What is chocolate?
Silly question. Fascinating answer.
The word “chocolate” comes from the word xocolātl. This word is from the Aztec language (Nahuatl), and is a combination of the words xococ (meaning ‘sour or bitter’), and ātl (‘water or drink’). This is because for the vast majority of it’s existence, chocolate has been consumed as a drink.
Fermented beverages made from chocolate date back to 1900 BC in Mesoamerica. The Aztecs believed that cacao seeds were a divine gift from the god of wisdom, ‘Quetzalcoatl’. In fact, the seeds were so precious to the Aztecs that they once had so much value that they were used as a form of currency.
Chocolate was introduced to Europe in the 16th century by the Spanish who added sugar or honey to counteract the natural bitterness. Since then, it has had a rather successful rise in popularity.
Chocolate comes from the beans of the Theobroma cacao tree – an evergreen native to the tropical regions of Central and South America. The beans are produced in pods, like these:
Pods of the of Theobroma cacao tree. Source: Wikipedia
Cacao beans are harvested from the pods, and then allowed to ferment over a period two weeks. Two things happen during this process: 1. outside of the pod, the beans are exposed to the warm heat which kills the germinating seed, and 2. natural yeasts – which like the heat – grow and help to develop complex flavours.
After this fermentation period, the beans are then sun-dried, which helps to preserve them for shipping. Next, the beans are roasted, which helps to further develop complex flavours and to remove unpleasant acidic compounds developed in the fermentation process. This is followed by mechanically separating the valuable nibs (interior of the bean) from the useless shells.
The nibs must then be refined, which involves extensive grinding. The raw cocoa liquor is then “conched“. This is the stage where the general characteristic tastes, smells and textures of chocolate are developed. Conching is a lengthy process which drives off the rest of the acidic flavoring compounds. The process also helps coat the ground up cocoa particles with fat to reduce the viscosity of the molten chocolate.
Finally, the conched product is tempered which gives chocolate it’s gloss and affects how it melts in your hands/mouth. Tempering is necessary because cocoa butter can crystallise into at least six different forms (form V being the most desired). Each of these forms have different stability and properties. Form V has the most popular texture and ‘feeling in the mouth’, in addition it does not melt too quickly in the hand.
Why is chocolate soooo good?
No one is entirely sure. Chocolate contains many different chemicals which help in making chocolate tasty and (dare we say it) addictive. Among the most important ingredients are stimulants like phenylethylamine and caffeine (all in very small quantities), which can give you a positive boost.
Importantly, chocolate also contains a feel-good chemical called anandamine, which functions in the brain by binding to cannabinoid receptors (these are the same receptors that chemicals in marijuana bind to). Its name actually comes from ananda, the Sanskrit word for “bliss”. Normally anandamide is broken down quite quickly after it is produced, but some researchers believe that the anandamide in chocolate makes the natural anandamide in our brain persist for longer, giving us a longer-lasting “chocolate high”.
And what is the difference between dark and white chocolate?
Ok, now don’t be upset, but technically speaking white chocolate is not really a chocolate.
It is made without any cocoa powder or solids, containing just cocoa butter mixed with milk and sugar. Without the cocoa powder, chocolate has no colour thus it’s white. In addition, white chocolate doesn’t have many of the ‘happy’ ingredients likes caffeine.
Not actually being a chocolate makes white chocolate very useful, however, in research (as you shall see below). Given that it is missing many of the key components of normal chocolate (eg. cocoa, caffeine, etc), white chocolate can be used as a control substance in studies looking at the effect of chocolate on various conditions.
Are there health benefits of eating chocolate?
Mum always told me that chocolate was bad for me, but recent scientific research has altered this perception. Studies of the Kuna Indians of the San Blas islands of Panama, who consume large amounts of a natural cocoa beverage, have found lower blood pressures, better renal function and decreased cardiovascular mortality relative to mainland Panamanian control populations (Click here to read more on this).
The prevalence of hypertension in Kuna indians who have migrated to urban areas on mainland Panama is significantly higher (10.7% of the population compared with just 2.2% of those still on the islands). This is believed to be partly due to the reduction in cacao intake – Kuna indians on the islands eat 10 times more than their mainland equivalents.
Interesting. But what does all of this have to do with Parkinson’s disease?
Right. Down to business. In 2009, this research report was published:
Title:Chocolate consumption is increased in Parkinson’s disease. Results from a self-questionnaire study. Authors: Wolz M, Kaminsky A, Löhle M, Koch R, Storch A, Reichmann H. Journal: J Neurol. 2009 Mar;256(3):488-92. doi: 10.1007/s00415-009-0118-9. PMID:19277767
These researchers conducted a survey of 274 people with Parkinson’s disease and 234 age-matched controls. They found that people with Parkinson’s disease ate approx. 100g of chocolate per week (on average) compared to just 57.3g for the control subjects.
Using measures of mood (such as the Beck’s Depression Inventory survey), the researchers found that this increased consumption of chocolate was independent of feelings of depression. This interesting observations lead the researchers to conduct this clinical study:
Title:Comparison of chocolate to cacao-free white chocolate in Parkinson’s disease: a single-dose, investigator-blinded, placebo-controlled, crossover trial. Authors: Wolz M, Schleiffer C, Klingelhöfer L, Schneider C, Proft F, Schwanebeck U, Reichmann H, Riederer P, Storch A. Journal: J Neurol. 2012 Nov;259(11):2447-51. doi: 10.1007/s00415-012-6527-1. PMID:22584952
The researchers in this study (the same people who published the survey study above) tested the effects of 200g of (80% cacao) chocolate on Parkinsonian motor scores (as measured by UPDRS). They assessed 26 people with moderate non-fluctuating Parkinson’s disease at both 1 and 3 hours after eating the chocolate. The researchers used white chocolate as the control treatment in the study, and they (the assessors) were blind to which treatment each subject received.
At 1 hour after consumption, the researchers noted a mild decrease in both treatment groups (most statistically in the dark chocolate group) when compared to the measures taken at baseline (that is before the actual study started). Similar results were observed in the measures taken at 3 hours post consumption. The researchers also took blood samples and found no differences in β-phenylethylamine blood levels (we’ll come back to this shortly).
Altogether, while there was an improvement in motor performance after eating chocolate, the results indicated no difference between dark chocolate and white cacao-free chocolate on Parkinson’s motor function.
What is β-phenylethylamine?
β-phenylethylamine is a naturally occurring chemical in the body, which is produced in chocolate during the thermal processing of cocoa (click here for more on this). Functionally, β-phenethylamine is similar to amphetamine in its action, as it leads to the release of dopamine. Interestingly, people with Parkinson’s disease have almost 50% less β-phenethylamine in the fluid surrounding their brains (Click here to read more on this). Thus, in addition to any stimulant effect of caffeine, increasing β-phenethylamine levels by eating chocolate may be causing an increase in dopamine levels in the brains of people with Parkinson’s disease – resulting in better motor scores.
But the researchers in the clinical study of chocolate reviewed above did not register any change in blood levels of β-phenethylamine. Again, perhaps longer term usage is required in order to detect a significant rise.
What does it all mean?
Here at the SoPD, we feel that the effect of chocolate on Parkinson’s disease have not been fully explored. More research is required. And we are not just saying this because everyone likes chocolate.
Firstly, it would be interesting to replicate what has already been done, particularly the survey of chocolate consumption to determine if people with Parkinson’s disease really do eat more chocolate! This is the most interesting observation reported thus far and needs to be replicated. It would be interesting to determine if the difference pre-dates diagnosis – that is to say, do people who develop Parkinson’s disease eat more chocolate when they are younger (before they are diagnosed)? Could chocolate be actually having a negative effect on the development of the disease?
Second, if a longer term analysis of chocolate and Parkinson’s disease indicates an effect, it would be interesting to further investigate individual ingredients. If we are investigating the ingredients of coffee to assess beneficial components for Parkinson’s disease (click here for more on this), the same analysis of chocolate should be conducted.
I’m going to go off now and contemplate some of this with a piece of dark chocolate…
The banner for today’s post was sourced from pngimg.
Exciting new last week from a small biotech company called Voyager Therapeutics which is using gene therapy to treat neurodegenerative disease. Their primary product (VY-AADC01) is focused on Parkinson’s disease and the initial results look very positive.
The press release has indicates that the treatment is well tolerated and has beneficial effects on the subject’s motor functions. This last part is very interesting as the trial is being conducted on people with advanced Parkinson’s disease.
In today’s post, we’ll review the technology and what the results mean.
In Parkinson’s disease, we often talk about the loss of the dopamine neurons in the midbrain as a cardinal feature of the disease. When people are diagnosed with Parkinson’s disease, they have usually lost approximately 50-60% of the dopamine neurons in an area of the brain called the substantia nigra.
The dark pigmented dopamine neurons in the substantia nigra are reduced in the Parkinson’s disease brain (right). Source: Memorangapp
The midbrain is – as the label suggests – in the middle of the brain, just above the brainstem (see image below). The substantia nigra dopamine neurons reside there.
Location of the substantia nigra in the midbrain. Source: Memorylossonline
The dopamine neurons of the substantia nigra generate dopamine and release that chemical in different areas of the brain. The primary regions of that release are areas of the brain called the putamen and the Caudate nucleus. The dopamine neurons of the substantia nigra have long projections (or axons) that extend a long way across the brain to the putamen and caudate nucleus, so that dopamine can be released there.
The projections of the substantia nigra dopamine neurons. Source: MyBrainNotes
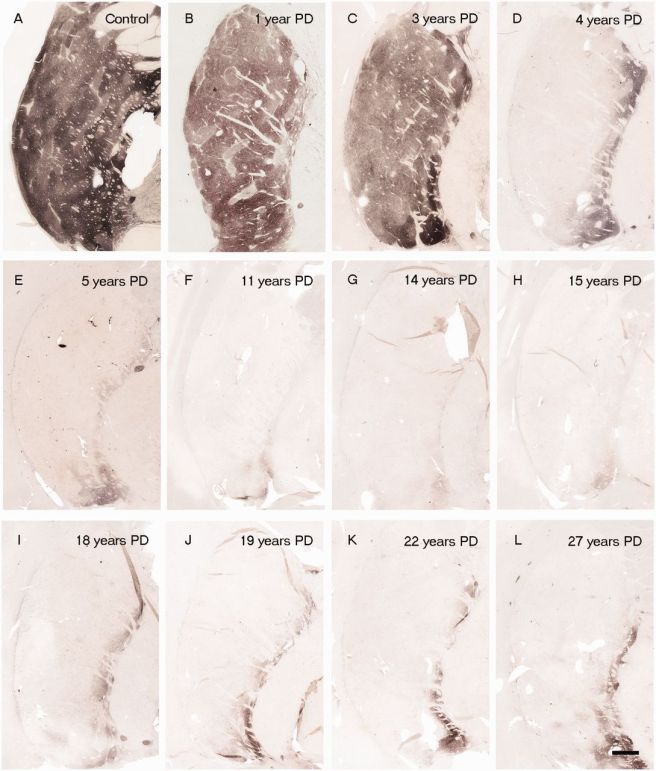
In Parkinson’s disease, these ‘axon’ extensions that project to the putamen and caudate nucleus gradually disappear as the dopamine neurons of the substantia nigra are lost. When one looks at brain sections of the putamen after the axons have been labelled with a dark staining technique, this reduction in axons is very apparent over time, especially when compared to a healthy control brain.
The putamen in Parkinson’s disease (across time). Source: Brain
Previously we have discussed replacing the loss dopamine by transplanting dopamine producing cells into the putamen (click here to read that post), but some researchers now believe that this is not necessary. Instead they have proposed using gene therapy for Parkinson’s disease.
What is gene therapy?
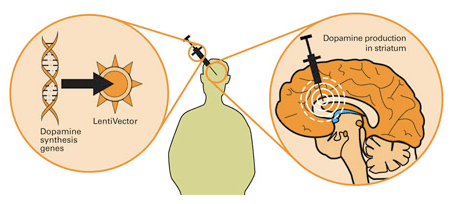
The gene therapy involves inducing cells to produce proteins that they usually do not. This is usually done using genetically modified viruses which have had all the disease causing component removed, allowing us to use the virus as an efficient delivery system. Viruses by their very nature are very good at infecting cells, so if we remove the disease causing components, what is left is a very effective delivery system. Taking this approach one step further, we could next take genes involved with dopamine synthesis and insert them into our empty virus. By then injecting this virus into the brain, we could produce dopamine in any infected cells (it’s slightly more complicated than that, but you get the basic idea).
Gene therapy for Parkinson’s disease. Source: Wiki.Epfl
This approach demonstrated amazing results in preclinical studies in the lab, but the transition to the clinic has not been easy (click here for a good review of the field).
What has been done in the clinic for gene therapy and Parkinson’s disease?
The first clinical attempt at gene therapy for Parkinson’s disease involved injecting a virus containing a gene called glutamic acid decarboxylase (GAD), which is an enzyme involved in the production of a chemical called GABA. The virus was injected into an area of the brain called the subthalamic nucleus, which becomes over-active in Parkinson’s disease. By ectopically producing GAD in the subthalamic nucleus, researchers were able to reduce the level of activity (this is similar to deep brain stimulation in Parkinson’s disease which modulates the activity of the subthalamic nucleus). The clinical trials for GAD produced modest results. The virus was well tolerated, but the clinical effect was limited.
Another clinical trial attempted to cause cells in the putamen to produce a chemical called neurturin (which is very similar to GDNF – we have previously written about GDNF, click here to read that post). The goal of the study was to prove neuroprotection and regeneration to the remaining dopamine neurons, by releasing neurturin in the putamen. Subjects were injected in the putamen with the virus and then the participants were followed for 15 months. Unfortunately,this study failed to demonstrate any meaningful improvement in subjects with Parkinson’s disease.
So what were the results of the trial?
Voyager Therapeutics‘s gene therapy product, VY-AADC01 is an adeno associated virus that carries a gene called Aromatic L-amino acid decarboxylase (or AADC).
AADC is the enzyme that converts L-dopa into dopamine. L-dopa can be naturally produced in the brain from Tyrosine that is absorbed from the blood. It is also the basic component of many treatments for Parkinson’s disease.
By injecting VY-AADC01 into the putamen of people with advanced Parkinson’s disease, Voyager is hoping to alleviate the motor features of the condition by allowing the brain to produce a constant supply of dopamine in the exact location that is missing the dopamine (remember, the putamen is where dopamine is released). This approach will not cure the disease, but it may make life a lot easier for those affected by it.
The phase 1b clinical trial was designed to assess whether the virus had any negative side effects in humans. After the subjects were injected in the brain with VY-AADC01, they were assessed at six and twelve months after the surgery. The results suggest that the virus was well tolerated and resulted in increased AADC enzyme activity, enhanced response to L-dopa treatment, and clinically meaningful improvements in various measures of patients’ motor function (44% improvement in ‘off medication’ measures and 55% improvement in ‘on medication’ measures).
The company currently has 2 groups of subjects injected with the virus (two different concentrations) and they are looking to have a third group injected in early 2017. Phase 2 trials are planned to begin in late 2017.
What does it all mean?
Well, this is a very interesting result and bodes well for other companies taking similar gene therapy approaches (these include Oxford BioMedica and Genepod Therapeutics).
They are also interesting results because the subjects involved in the study all have advanced Parkinson’s disease (the average time since diagnosis in the subject was 10 years). So it is very positive news to see beneficial effects in later stage subjects.
Our ability to delivery of genes to different locations is a symbol of how far we have come with our understanding of biology. The fact that this knowledge is now having a positive impact in the medical world is very exciting. Gene therapy is one treatment approach that we here at SoPD are very excited about and watching very closely.



























































{kind=link}