Plain English information about the research being conducted on Parkinson's
Tag: The Science of Parkinson’s disease
Information about Parkinson’s disease provided by scientists doing the research. Weekly news updates on what is happening in science related to Parkinson’s disease, and the opportunity to ask questions and get answers.
For many people diagnosed with Parkinson’s disease, one of the scariest prospects of the condition that they face is the possibility of developing dyskinesias.
Dyskinesias are involuntary movements that can develop after long term use of the primary treatment of Parkinson’s disease: Levodopa
In todays post I discuss one experimental strategy for dealing with this debilitating aspect of Parkinson’s disease.
There is a normal course of events with Parkinson’s disease (and yes, I am grossly generalising here).
First comes the shock of the diagnosis.
This is generally followed by the roller coaster of various emotions (including disbelief, sadness, anger, denial).
Then comes the period during which one will try to familiarise oneself with the condition (reading books, searching online, joining Facebook groups), and this usually leads to awareness of some of the realities of the condition.
One of those realities (especially for people with early onset Parkinson’s disease) are dyskinesias.
What are dyskinesias?
Dyskinesias (from Greek: dys – abnormal; and kinēsis – motion, movement) are simply a category of movement disorders that are characterised by involuntary muscle movements. And they are certainly not specific to Parkinson’s disease.
As I have suggested in the summary at the top, they are associated in Parkinson’s disease with long-term use of Levodopa (also known as Sinemet or Madopar).
The image above presents a ‘before treatment’ (left) and ‘after treatment’ (right) brain scan image from a recent research report of a clinical study that looked at the use of Acetylcysteine (also known as N-acetylcysteine or simply NAC) in Parkinson’s disease.
DaTscan brain imaging technique allows us to look at the level of dopamine processing in an individual’s brain. Red areas representing a lot; blue areas – not so much. The image above represents a rather remarkable result and it certainly grabbed our attention here at the SoPD HQ (I have never seen anything like it!).
In today’s post, we will review the science behind this NAC and discuss what is happening with ongoing clinical trials.
Acetylcysteine (N-acetylcysteine or NAC – commercially named Mucomyst) is a prodrug – that is a compound that undergoes a transformation when ingested by the body and then begins exhibiting pharmacological effects. Acetylcysteine serves as a prodrug to a protein called L-cysteine, and – just as L-dopa is an intermediate in the production of dopamine – L-cysteine is an intermediate in the production of another protein called glutathione.
Take home message: Acetylcysteine allows for increased production of Glutathione.
Glutathione (pronounced “gloota-thigh-own”) is a tripeptide (a string of three amino acids connected by peptide bonds) containing the amino acids glycine, glutamic acid, and cysteine. It is produced naturally in nearly all cells. In the brain, glutathione is concentrated in the helper cells (called astrocytes) and also in the branches of neurons, but not in the actual cell body of the neuron.
One of the most common observations that people make when they attend a Parkinson’s disease support group meeting is the huge variety of symptoms between sufferers.
Some people affected by this condition are more tremor dominant, while others have more pronounced gait (or walking) issues. In addition, some people have an early onset version, while others has a very later onset. What could explain this wide range of features?
A group of Stanford researchers have recently proposed an interesting new idea regarding our understanding of genetics that could partly explain some of this variability. In todays post I speculate on whether their idea could be applied to Parkinson’s disease.
Earlier this year an interesting study was published in the prestigious journal Nature on the topic of the genetics of height (yes height. Trust me, I’m going somewhere with this):
Title: Rare and low-frequency coding variants alter human adult height Authors: Marouli E, Graff M, Medina-Gomez C, Lo KS, Wood AR, Kjaer TR, Fine RS, Lu Y, Schurmann C,………at least 200 additional authors have been deleted here in order to save some space…….EPIC-InterAct Consortium; CHD Exome+ Consortium; ExomeBP Consortium; T2D-Genes Consortium; GoT2D Genes Consortium; Global Lipids Genetics Consortium; ReproGen Consortium; MAGIC Investigators, Rotter JI, Boehnke M, Kathiresan S, McCarthy MI, Willer CJ, Stefansson K, Borecki IB, Liu DJ, North KE, Heard-Costa NL, Pers TH, Lindgren CM, Oxvig C, Kutalik Z, Rivadeneira F, Loos RJ, Frayling TM, Hirschhorn JN, Deloukas P, Lettre G. Journal: Nature. 2017 Feb 9;542(7640):186-190. PMID:28146470
In this study, the researchers – who are part of the GIANT consortium – were analysing DNA collected from over 700,000 people and trying to determine what genetic differences could influence height.
Firstly, it is easy to accurately measure. Second, the researchers believed that if we can master the complex genetics of something simple like height maybe what we learn will give us a blueprint for how we should study more complex medical disorders that have thus far eluded our complete understanding.
On the 27th June, 1997, a research report was published in the prestigious scientific journal ‘Science’ that would change the world of Parkinson’s disease research forever.
And I am not exaggerating here.
The discovery that genetic variations in a gene called alpha synuclein could increase the risk of developing Parkinson’s disease opened up whole new areas of research and eventually led to ongoing clinical trials of potential therapeutic applications.
Todays post recounts the events surrounding the discovery, what has happened since, and we will discuss where things are heading in the future.
In world events, President Bill Clinton was entering his second term, Madeleine Albright became the first female Secretary of State for the USA, Tony Blair became the prime minister of the UK, and Great Britain handed back Hong Kong to China.
In the world of entertainment, author J. K. Rowling’s debut novel “Harry Potter and the Philosopher’s Stone” was published by Bloomsbury, and Teletubbies, South Park, Ally McBeal, and Cold Feet (it’s a British thing) all appeared on TV for the first time, amusing and entertaining the various age groups associated with them.
Musically, rock band Blur released their popular hit song ‘Song 2‘ (released 7th April), “Bitter Sweet Symphony” by the Verve entered the UK charts at number 2 in June, and rapper Notorious B.I.G. was killed in a drive by shooting. Oh, and let’s not forget that “Tubthumping” (also known as “I Get Knocked Down”) by Chumbawamba was driving everybody nuts for its ubiquitous presence.
And at the cinemas, no one seemed to care about anything except a silly movie called Titanic.
In this post we discuss several recently published research reports suggesting that Parkinson’s disease may be an autoimmune condition. “Autoimmunity” occurs when the defence system of the body starts attacks the body itself.
This new research does not explain what causes of Parkinson’s disease, but it could explain why certain brain cells are being lost in some people with Parkinson’s disease. And such information could point us towards novel therapeutic strategies.
The journal Nature was first published on 4th November 1869, by Alexander MacMillan. It hoped to “provide cultivated readers with an accessible forum for reading about advances in scientific knowledge.” It has subsequently become one of the most prestigious scientific journals in the world, with an online readership of approximately 3 million unique readers per month (almost as much as we have here at the SoPD).
Each Wednesday afternoon, researchers around the world await the weekly outpouring of new research from Nature. And this week a research report was published in Nature that could be big for the world of Parkinson’s disease. Really big!
On the 21st June, this report was published:
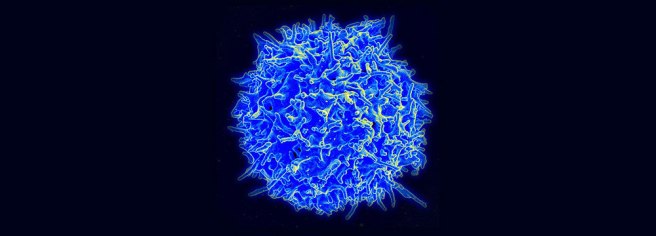
Title: T cells from patients with Parkinson’s disease recognize α-synuclein peptides Authors: Sulzer D, Alcalay RN, Garretti F, Cote L, Kanter E, Agin-Liebes J, Liong C, McMurtrey C, Hildebrand WH, Mao X, Dawson VL, Dawson TM, Oseroff C, Pham J, Sidney J, Dillon MB, Carpenter C, Weiskopf D, Phillips E, Mallal S, Peters B, Frazier A, Lindestam Arlehamn CS, Sette A Journal:Nature. 2017 Jun 21. doi: 10.1038/nature22815. PMID: 28636593
In their study, the investigators collected blood samples from 67 people with Parkinson’s disease and from 36 healthy patients (which were used as control samples). They then exposed the blood samples to fragments of proteins found in brain cells, including fragments of alpha synuclein – this is the protein that is so closely associated with Parkinson’s disease (it makes regular appearances on this blog).
What happened next was rather startling: the blood from the Parkinson’s patients had a strong reaction to two specific fragments of alpha synuclein, while the blood from the control subjects hardly reacted at all to these fragments.
In the image below, you will see the fragments listed along the bottom of the graph (protein fragments are labelled with combinations of alphabetical letters). The grey band on the plot indicates the two fragments that elicited a strong reaction from the blood cells – note the number of black dots (indicating PD samples) within the band, compared to the number of white dots (control samples). The numbers on the left side of the graph indicate the number of reacting cells per 100,000 blood cells.
The investigators concluded from this experiment that these alpha synuclein fragments may be acting as antigenic epitopes, which would drive immune responses in people with Parkinson’s disease and they decided to investigate this further.
The first thing I asked Dr Lysimachos Zografos when we met was: “Are you crazy?”
Understand that I did not mean the question in a negative or offensive manner. I asked it in the same way people ask if Elon Musk is crazy for starting a company with the goal of ‘colonising Mars’.
In 2014, Lysimachos left a nice job in academic research to start a small biotech firm that would use flies to screen for drugsthat could be used to treat Parkinson’s disease. An interesting idea, right? But a rather incredible undertaking when you consider the enormous resources of the competition: big pharmaceutical companies. No matter which way you look at this, it has the makings of a real David versus Goliath story.
But also understand this: when I asked him that question, there was a strong element of jealousy in my voice.
Incorporated in October 2014, this University of Edinburgh spin-out company has already had an interesting story. Here at the SoPD, we have been following their activities with interest for some time, and decided to write this post to make readers aware of them.
New research was published last week that suggests people with a high body mass index (or BMI) have a reduced risk of developing Parkinson’s disease.
Really? How does that work?
In todays post we will discuss what body mass index is, review the results of the study and consider what this means for our understanding of Parkinson’s disease.
Humans being come in all sorts of different shapes and sizes.
Tall, short, skinny, obese….
The interesting aspect about some of these differences is the way they can make us vulnerable to certain diseases. For example, we have previously discussed how people with red hair have are 4 times more likely to develop Parkinson’s disease than dark haired people (Click here to read that post, and here for a follow up post).
And now we have new research suggesting that your body mass may also influence your risk of developing Parkinson’s disease.
What do you mean by body mass?
Your body mass is simply your weight.
It can be used to determine your approximate level of health by applying it to the body mass index.
The body mass index (or BMI) – also known as the Quetelet index – is a measure that is derived from the weight and height of an individual. Body mass index can be calculated according to the following formula:
That is simply your weight in kilograms divided by your height in metres squared.
For example, if you were a ridiculously tall (2.08 metres – 6 foot 8) Parkinson’s research scientist with bad hair and an approximate weight of 105kg (230 pounds), your BMI score would be 24.2 (time to put the laptop down and go for some walks). This was calculated by dividing 105 by 4.3 (2.08 x 2.08meters).
So what is the new research about BMI and Parkinson’s disease?
This is Dr Alastair Noyce:
He leads the PredictPD study (a really interesting longitudinal study to identify people at risk of Parkinson’s disease), which is based out of University College London. He is the lead author of the study.
And this is Prof Nick Wood:
He is the Galton Professor of Genetics, and the neuroscience programme director for Biomedical Research Centre at University College London. He has been at the forefront of many of the discoveries associated with the genetics of Parkinson’s disease, and he is the senior author of the study.
And this is the study:
Title: Estimating the causal influence of body mass index on risk of Parkinson disease: A Mendelian randomisation study. Authors: Noyce AJ, Kia DA, Hemani G, Nicolas A, Price TR, De Pablo-Fernandez E, Haycock PC, Lewis PA, Foltynie T, Davey Smith G; International Parkinson Disease Genomics Consortium, Schrag A, Lees AJ, Hardy J, Singleton A, Nalls MA, Pearce N, Lawlor DA, Wood NW. Journal: PLoS Med. 2017 Jun 13;14(6):e1002314. PMID:28609445 (This article is OPEN ACCESS if you would like to read it)
The researchers who published this study were interested in determining whether BMI and the future risk of Parkinson’s disease had any association (as you will see below there has previously been some disagreement about this). They began by collected data from the GIANT (Genetic Investigation of Anthropometric Traits) study. The GIANT study was a huge consortium that was set up identify regions or variations within DNA that could impact body size and shape (such as height and measures of obesity). They didn’t find very many, but the dataset represents an enormous resource for researchers to use (information about 2,554,637 genetic variants from 339,224 individuals of European descent).
They next collected all of the most recent data about genetic variations associated with Parkinson’s disease (7,782,514 genetic variants from 13,708 cases of Parkinson’s disease and 95,282 individuals acting as controls, pooled from 15 independent datasets of individuals of European descent).
Using these two sets of data, the researchers were able to determine any relationship between genetic variants and BMI, and any relationship between those same genetic variants and Parkinson’s disease. Using this approach, they could then determine an estimated change in the risk of Parkinson’s disease per unit change in BMI score.
And when they conducted that analysis, the researchers found genetic variants expected to increase ones BMI score higher by 5 were actually associated with an 18 percent lower risk of Parkinson’s disease. That is to say, higher BMI scores were associated with a lower risk of developing Parkinson’s disease – the odds ratio was 0.82 (1 being no difference) and the range of the odds was 0.69–0.98.
So does this mean I’m allowed to get fat? You know, to prevent Parkinson’s?
No. This would not be advisable.
One of the major limitations of this study (and many studies like it) is that individuals who have a higher BMI score have an increased risk of other diseases (heart disease, etc) which could result in an earlier death. They may die before they were eventually going to develop Parkinson’s disease. This ‘early death’ effect could result in individuals with a lower BMI being over-represented in the group of people diagnosed with Parkinson disease. This is called a “frailty effect”. In an attempt to reduce the possibility of a frailty effect in this study, the researchers conducted a further analysis (called ‘Frailty simulations’) to assess whether any associations they found were affected by mortality selection. This analysis suggested that the frailty effect could at least partially account for the association. That is to say, high BMI people dying earlier could partly explain the reduced frequency of Parkinson’s disease in that group.
In addition, there could also be subgroups within the low or high BMI population that could be affecting the data. The datasets used in the study lack of information about additional possible confounding variables. Confounding variables are factors that could influence the outcome of a study that haven’t been controlled for. In this study, for example, there was no information about smoking or coffee drinking, which have both been found to reduce risk of developing Parkinson’s disease. Perhaps a subset of cases in the high BMI group were serious smokers and coffee drinkers?
So, don’t go changing to a high cholesterol diet just yet.
How does this result compare to previous research on BMI and Parkinson’s disease?
It is fair to say that there has been a lack of consensus in this field of research.
There is certainly evidence to support the results of this new research report. Earlier this year, for example, researchers in Korea reported that brain imaging of 400 people recently diagnosed with Parkinson’s disease suggested a lower BMI might be closely associated with low density of dopaminergic neurons in the midbrain, a region badly affected in Parkinson’s disease (Click here to read more about that study).
But there is also some research that suggests that there no association between BMI and Parkinson’s disease, including this study which analysed data from multiple studies:
Title: Body Mass Index and Risk of Parkinson’s Disease: A Dose-Response Meta-Analysis of Prospective Studies. Authors: Wang YL, Wang YT, Li JF, Zhang YZ, Yin HL, Han B. Journal: PLoS One. 2015 Jun 29;10(6):e0131778. PMID:26121579 (This article is OPEN ACCESS if you would like to read it)
This study analysed data from 10 different studies and found no association between BMI and risk of developing Parkinson’s disease.
And then there have been studies which have found the opposite effect of the new study – that is lower BMI scores are associated with a lower risk of developing Parkinson’s disease (Click here and here to read more about those studies).
These previous studies, however, have all been observational studies. The beauty of this new research report is that they applied genetic analysis to the question, which has helped them to better define and characterise their population of interest. It will be interesting to see if future studies taking a similar approach can provide some kind of consensus here.
What about BMI after someone is diagnosed with Parkinson’s disease?
Here the picture becomes a little bit clearer.
Weight loss can be a common feature of Parkinson’s disease:
Title: Association Between Change in Body Mass Index, Unified Parkinson’s Disease Rating Scale Scores, and Survival Among Persons With Parkinson Disease: Secondary Analysis of Longitudinal Data From NINDS Exploratory Trials in Parkinson Disease Long-term Study 1. Authors: Wills AM, Pérez A, Wang J, Su X, Morgan J, Rajan SS, Leehey MA, Pontone GM, Chou KL, Umeh C, Mari Z, Boyd J; NINDS Exploratory Trials in Parkinson Disease (NET-PD) Investigators. Journal: JAMA Neurol. 2016 Mar;73(3):321-8. PMID:26751506 (This article is OPEN ACCESS if you would like to read it)
In this study, 1673 people with Parkinson’s disease were recruited and followed over 3-6 years. Of these participants, 158 (9.4%) experienced weight loss (or a decrease in BMI), while 233 (13.9%) experienced weight gain (an increase in BMI). The weight loss group demonstrated an increase in the Unified Parkinson’s Disease Rating Scale (UPDRS) motor score (which indicates a worsening of Parkinsonian features), while the weight gain group actually exhibited a subtle decrease in their motor scores (an improvement in Parkinson’s features).
And this association between wait loss and worsening disease state is supported in a second study:
Title: Weight loss and impact on quality of life in Parkinson’s disease. Authors: Akbar U, He Y, Dai Y, Hack N, Malaty I, McFarland NR, Hess C, Schmidt P, Wu S, Okun MS. Journal: PLoS One. 2015 May 4;10(5):e0124541. PMID:25938478 (This article is OPEN ACCESS if you would like to read it)
In this study of 1718 people with Parkinson’s disease, the researchers found that more rapid weight loss was associated with higher number of co-morbidities (other medical complications), older age, higher L-dopa usage, and decreased health-related quality of life.
Thus weight loss is something for everyone to keep an eye on.
IMPORTANT NOTE: Weight loss can become apparent with an increase in dykinesias, but this is generally due to increased activity levels increasing levels of metabolism.
What does it all mean?
Using very large datasets, researchers in London have recently found that higher BMI scores are associated with a lower risk of developing Parkinson’s disease. This result is very interesting, even if much of the effect could be accounted for by the early mortality problem in the high BMI group.
Exactly how high BMI could infer neuroprotection or reduced chance of incurring the condition is still to be determined, and understanding the mechanisms of this effect could provide new understanding about the disease. It is ill advised, however, to consider that increasing ones BMI as a practical strategy for reducing the risk of developing Parkinson’s disease.
For the vast majority of the general population, science is consumed via mass media head lines and carefully edited summaries of the research.
The result of this simplified end product is an ignorance of the process that researchers need to deal with in order to get their research in the public domain.
As part of our efforts to educate the general public about the scientific research of Parkinson’s disease, it is necessary to also make them aware of that process, the issues associated with it, and how it is changing over time.
In todays post, we will look at how new research reports are being made available to the public domain before they are published.
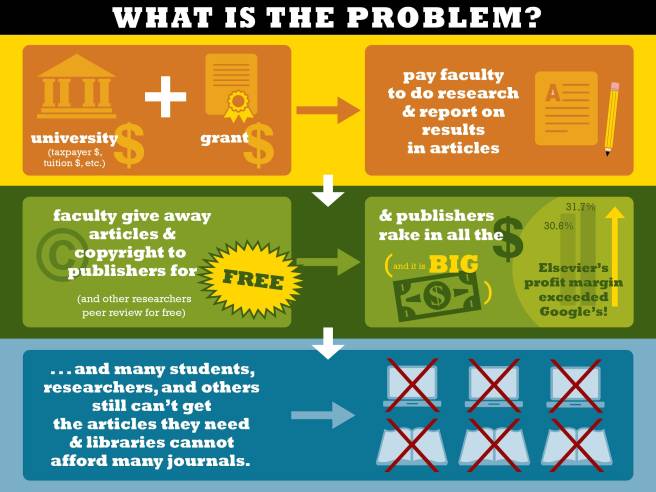
Getting research into the public domain. Source: STAT
Every morning here at the SoPD, we look at what new research has entered the public domain over night and try to highlight some of the Parkinson’s disease relevant bits on our Twitter account (@ScienceofPD).
To the frustration of many of our followers, however, much of that research sits behind the pay-to-view walls of big publishing houses. One is allowed to read the abstract of the research report in most cases, but not the full report.
Given that charity money and tax payer dollars are paying for much of the research being conducted, and for the publication fee (approx. $1500 per report on average) to get the report into the journal, there is little debate as to the lack of public good in such a system. To make matter worse, many of the scientists doing the research can not access the published research reports, because their universities and research institutes can not afford the hefty access fees for all of the journals.
To be fair, the large publishing houses have recognised that this is not a sustainable business model, and they have put forward the development of open-access web-based science journals, such as Nature communications, Scientific reports, and Cell reports. But the fees for publishing in these journals can in some cases be higher than the closed access publications.
This is crazy. What can we do about it?
Well, there have been efforts for some time to improve the situation.
Projects like the Public Library of Science (or PLOS) have been very popular and are now becoming a real force on the scientific publishing landscape (they recently celebrated their 10 year anniversary and during that time they have published more than 165,000 research articles). But they too have costs associated with maintaining their service and publications fees can still be significant.
Is there an easier way of making this research available?
Looks like the mad scientist type right? Don’t be fooled. He’s awesome! Prof Ginsparg is a professor of Physics and Computing & Information Science at Cornell University.
Back in 1991, he started a repository of pre-print publications in the field of physics. The repository was named arXiv.org, and it allowed physics researchers to share and comment on each others research reports before they were actually published.
The site slowly became an overnight sensation.
The number of manuscripts deposited at arXiv passed the half-million mark on October 3, 2008, the million manuscript mark by the end of 2014 (with a submission rate of more than 8,000 manuscripts per month). The site currently has 1,257,315 manuscripts that are freely available to access. A future nobel prize winning bit of research is probably in there!
Now, by their very nature, and in a very general sense, biomedical researchers are a jealous bunch.
For many years they looked on with envy at the hive of activity going on at arXiv and wished that they had something like it themselves. And now they do! In November 2013, Cold Spring Harbor Laboratory in New York launched BioRxiv.
And the website is very quickly becoming a popular destination: by April 21, 2017, >10,000 manuscript had been posted, at a current rate of over 800 manuscripts per month (Source).
Recently they got a huge nod of financial support from the Chan Zuckerberg Initiative – a foundation set up by Facebook founder Mark Zuckerberg and his wife Priscilla Chan to “advance human potential and promote equality in areas such as health, education, scientific research and energy” (Wikipedia).
In April of this year, the Chan Zuckerberg Initiative announced a partnership with Cold Spring Harbor Laboratory to help support the site (Click here to see the press release).
So what is bioRxiv?
bioRxiv is a free OPEN ACCESS service that allows researchers to submit draft copies of scientific papers — called preprints — for their colleagues to read and comment on before they are actually published in peer-reviewed scientific journals.
Here are two videos explaining the idea:
Sounds great right?
To demonstrate how the bioRxiv process works, we have selected an interesting manuscript from the database that we would like to review here on the SoPD.
This is the article:
Title: In Vivo Phenotyping Of Parkinson-Specific Stem Cells Reveals Increased a-Synuclein Levels But No Spreading Authors: Hemmer K, Smits LM, Bolognin S, Schwamborn JC Database: BioRxiv DOI:https://doi.org/10.1101/140178 PMID: N/A (You can access the manuscript by clicking here)
In this study (which was posted on bioRxiv on the 19th May, 2017), the researchers have acquired skin cells from an 81 year old female with Parkinson’s disease who carries a mutation (G2019S) in the LRRK2 gene.
Mutations in the Leucine-rich repeat kinase 2 (or Lrrk2) gene are associated with an increased risk of developing Parkinson’s disease. The most common mutation of LRRK2 gene is G2019S, which is present in 5–6% of all familial cases of Parkinson’s disease, and is also present in 1–2% of all sporadic cases. We have previously discussed Lrrk2 (Click here to read that post).
The structure of Lrrk2 and where various mutations lie. Source:Intech
The skin cells were transformed using a bit of biological magic in induced pluripotent stem (or IPS) cells. We have previously discussed IPS cells and how they are created (Click here to read that post). By changing a subjects skin cell into a stem cell, researchers can grow the cell into any type of cell and then investigate a particular disease on a very individualised basis (the future of personalised medicine don’t you know).
IPS cell options available to Parkinson’s disease. Source: Nature
Using this IPS cell with a mutation in the LRRK2 gene, the researchers behind todays manuscript next grew the cells in culture and encouraged the cells to become dopamine producing cells (these are some of the most vulnerable cells in Parkinson’s disease). The investigators had previously shown that neurons grown in culture from cells with the G2019S mutation in the LRRK2 gene have elevated levels of of the Parkinson’s disease protein alpha Synuclein (Click here to read that OPEN ACCESS paper).
In this present study, the investigators wanted to know if these cells would also have elevated levels of alpha synuclein when transplanted into the brain. Their results indicate that the cells did. Next, the investigators wanted to use this transplantation model to see if the high levels of alpha synuclein in the transplanted cells would lead to the protein being passed to neighbouring cells.
Why did they want to do that?
One of the current theories regarding the mechanisms underlying the progressive spread of Parkinson’s disease is that the protein alpha synuclein is lead culprit. Under normal conditions, alpha synuclein usually floats around as an individual protein (or monomer), but sometime it starts to cluster (or aggregate) with other monomers of alpha synuclein and these form what we call oligomers. These oligomers are believed to be a toxic form of alpha synuclein that is being passed from cell to cell. And it ‘seeds’ the disease in each cell it is passed on to (Click here for a very good OPEN ACCESS review of this topic).
The passing of alpha synuclein between brain cells. Source: Nature
There have been postmortem analysis studies of the brains from people with Parkinson’s who have had cell transplantation therapy back in the 1990s. The analysis shows that some of the transplanted cells have evidence of toxic alpha synuclein in them – some of those cells have Lewy bodies in them, suggesting that the disease has been passed on to the healthy introduced cells from the diseased brain (Click here for the OPEN ACCESS research report about this).
In the current bioRxiv study, the investigators wanted to ask the reverse question:
Can unhealthy, toxic alpha synuclein producing cells cause the disease to spread into a healthy brain?
So after transplanted the Lrrk2 mutant cells into the brains of mice, they waited 11 weeks to see if the alpha synuclein would be passed on to the surrounding brain. According to their results, the unhealthy alpha synuclein did not transfer. They found no increase in levels of alpha synuclein in the cells surrounding the transplanted cells. The researchers concluded that within the parameters of their experiment, Parkinson’s disease-associated alpha synuclein spreading was not detected.
Interesting. When will this manuscript be published in a scientific journal?
We have no idea.
One sad truth of the old system of publication is: it may never be.
And this illustrates one of the beautiful features of bioRxiv.
This manuscript is probably going through the peer-review process at a particular scientific journal at the moment in order for it to be properly published. It is a process that will take several months. Independent reviewers will provide a critique of the work and either agree that it is ready for publication, suggest improvements that should be made before it can be published, or reject it outright due to possible flaws or general lack of impact (depending on the calibre of the journal – the big journals seem to only want sexy science). It is a brutal procedure and some manuscripts never actually survive it to get published, thus depriving the world of what should be freely available research results.
And this is where bioRxiv provides us with a useful forum to present scientific biological research that may never reach publication. Perhaps the researchers never actually intended to publish their findings, and just wanted to let the world know that someone had attempted the experiment and these are the results they got (there is a terrible bias in the world of research publishing to only publish positive results).
The point is: with bioRxiv we can have free access to the research before it is published and we do not have to wait for the slow peer-review process.
And there is definitely some public good in that.
EDITORS NOTE HERE: We are not suggesting for a second that the peer-review process should be done away with. The peer-review process is an essential and necessary aspect of scientific research, which helps to limit fraud and inaccuracies in the science being conducted.
What does it all mean?
This post may be boring for some of our regular readers, but it is important for everyone to understand that there are powerful forces at work in the background of scientific research that will determine the future of how information is disseminated to both the research community and general population. It is useful to be aware of these changes.
We hope that some of our readers will be bold/adventurous and have a look at some of what is on offer in the BioRxiv database. Maybe not now, but in the future. It will hopefully become a tremendous resource.
And we certainly encourage fellow researchers to use it (most of the big journals now accept preprint manuscripts being made available on sites like bioRxiv – click here to see a list of the journals that accept this practise) and some journals also allow authors to submit their manuscript directly to a journal’s submission system through bioRxiv via the bioRxiv to Journals (B2J) initiative (Click here for a list of the journals accepting this practise).
The times they are a changing…
The banner for today’s post was sourced from ScienceMag
Dipraglurant is a mGluR5 negative allosteric modulator (don’t panic, it’s not as complicated as it sounds).
In today’s post, we’ll explain what all of that means and look at the science behind this new treatment.
An example of a person with dyskinesia. Source: JAMA Neurology
For anyone familiar with Parkinson’s disease, they will know that long term use of the treatment L-dopa can lead to two possible outcomes:
The treatment loses it’s impact, requiring ever higher doses to be administered
The appearance of dykinesias
Now, not everyone taking L-dopa will be affected by both of these outcomes, but people with young, onset Parkinson’s disease do seem to be at risk of developing L-dopa induced dykinesias.
What are Dyskinesias?
Dyskinesias (from Greek: dys – abnormal; and kinēsis – motion, movement) are simply a category of movement disorders that are characterised by involuntary muscle movements. And they are certainly not specific to Parkinson’s disease.
As we have suggested above, they are associated in Parkinson’s disease with long-term use of L-dopa.
Below is a video of two legends: the late Tom Isaacs (who co-founded the Cure Parkinson’s Trust) and David Sangster (he founded www.1in20Parkinsons.org.uk). They were both diagnosed with Parkinson’s disease in their late 20’s. Tom, having lived with Parkinson’s for 20 years at the time of this video provides a good example of what dyskinesias look like:
As you can see, dyskinesias are a debilitating issue for anyone who suffers them.
How do dyskinesias develop in Parkinson’s disease?
Before being diagnosed and beginning a course of L-dopa, the locomotion parts of the brain in a person with Parkinson’s disease gradually becomes more and more inhibited. This increasing inhibition results in the slowness and difficulty in initiating movement that characterises this condition. A person with Parkinson’s may want to move, but they can’t.
They are akinetic (from Greek:a-,not,without; and kinēsis – motion).
Drawing of an akinetic individual with Parkinson’s disease, by Sir William Richard Gowers Source: Wikipedia
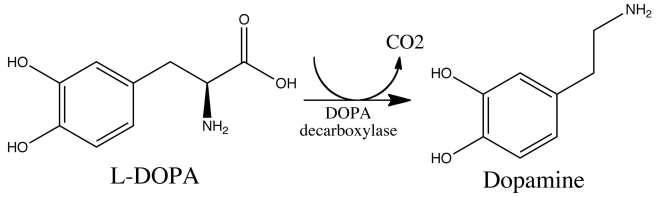
L-dopa tablets provide the brain with the precursor to the chemical dopamine. Dopamine producing cells are lost in Parkinson’s disease, so replacing the missing dopamine is one way to treat the motor features of the condition. Simply giving people pills of dopamine is a non-starter: dopamine is unstable, breaks down too quickly, and (strangely) has a very hard time getting into the brain. L-dopa, on the other hand, is very robust and has no problem getting into the brain.
Once inside the brain, L-dopa is quickly converted into dopamine. It is changed into dopamine by an enzyme called DOPA decarboxylase, and this change rapidly increases the levels of dopamine in the brain, allowing the locomotion parts of the brain to function more normally.
The chemical conversion of L-dopa to dopamine. Source: Nootrobox
In understanding this process, it is important to appreciate that when an L-dopa tablet is consumed and L-dopa enters the brain, there is a rapid increase in the levels of dopamine. A ‘spike’ in the supply of dopamine, if you will, and this will last for the next few hours, before the dopamine is used up.
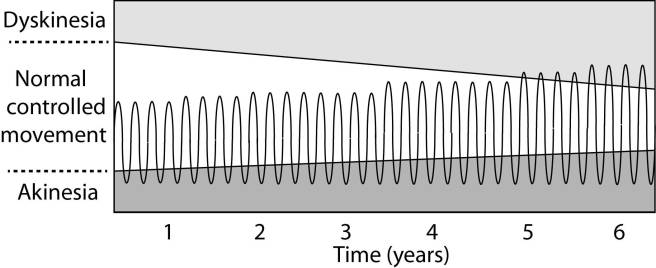
As the effects of the L-dopa tablet wear off, another tablet will be required. This use of multiple L-dopa pills across the day gives rise to a wave-like shape to the dopamine levels in the brain over the course of the day (see the figure below). The first pill in the morning will quickly lift the levels of dopamine enough that the individual will no longer feel akinetic. This will allow them to be able to function with normal controlled movement for several hours before the L-dopa begins to wear off. As the L-dopa wears off, the dopamine levels in the brain drop back towards levels that will leave the person feeling akinetic and at this point another L-dopa tablet is required.
After several years of L-dopa use, many people with Parkinson’s disease will experience a weaker response to each tablet. They will also find that they have more time during which they will be unable to move (exhibiting akinesia). This is simply the result of the progression of Parkinson’s disease – L-dopa treats the motor features of the disease but only hides/masks the fact that the disease is still progressing.
To combat this shorter response time, the dose of L-dopa is increased. This will result in increasing levels of dopamine in the brain (as illustrated by the higher wave form over time in the image below). It will take more L-dopa medication induced dopamine to lift the individual out of the akinetic state.
This increasing of L-dopa dosage, however, is often associated with the gradual development of abnormal involuntary movements that appear when the levels of L-dopa induced dopamine are the highest.
These are the dyskinesias.
Are there different types of dyskinesias?
Yes there are.
Dyskinesias have been broken down into many different subtypes, but the two main types of dyskinesia are:
Chorea – these are involuntary, irregular, purposeless, and unsustained movements. To an observer, Chorea will look like a very disorganised/uncoordinated attempt at dancing (hence the name, from the Greek word ‘χορεία’ which means ‘dance’). While the overall activity of the body can appear continuous, the individual movements are brief, infrequent and isolated. Chorea can cause problems with maintaining a sustained muscle contraction, which may result in affected people dropping things or even falling over.
Dystonia – these are sustained muscle contractions. They often occur at rest and can be either focal or generalized. Focal dystonias are involuntary contractions in a single body part, for example the upper facial area. Generalized dystonia, as the name suggests, are contraction affecting multiple body regions at the same time, typically the trunk, one or both legs, and another body part. The intensity of muscular movements in sufferers can fluctuate, and symptoms usually worsen during periods of fatigue or stress.
We have previously discussed the current treatment options for dyskinesias (click here to see that post).
Ok, so what clinical trials are Addex Therapeutics and the Michael J Fox Foundation preparing and why?
They are preparing to take a drug called Dipraglurant through phase III testing for L-dopa inducing dyskinesias in Parkinson’s disease. Dipraglurant is a mGluR5 negative allosteric modulator.
And yes, I know what you are going to ask next: what does any of that mean?
Ok, so mGluR5 (or Metabotropic glutamate receptor 5) is a G protein-coupled receptor. This is a structure that sits in the skin of a cell (the cell membrane), with one part exposed to the outside world – waiting for a chemical to bind to it – while another part is inside the cell, ready to act when the outside part is activated. The outside part of the structure is called the receptor.
Metabotropic receptors are a type of receptor that is indirectly linked with channels in cell membrane. These channels open and close, allowing specific elements to enter the cell. When a chemical (or agonist) binds to the receptor and it becomes activated, the part of the structure inside the cell will send a signal to the channel via a messenger (called a G-protein).
The chemical that binds to mGluR5 is the neurotransmitter glutamate.
But what about the “negative allosteric modulator” part of ‘mGluR5 negative allosteric modulator’
Good question.
This is the key part of this new approach. Allosteric modulators are a new class of orally available small molecule therapeutic agents. Traditionally, most marketed drugs bind directly to the same part of receptors that the body’s own natural occurring proteins attach to. But this means that those drugs are competing with those endogenous proteins, and this can limit the potential effect of the drug.
Allosteric modulators get around this problem by binding to a different parts of the receptor. And instead of simply turning on or off the receptor, allosteric modulators can either turn up the volume of the signal being sent by the receptor or decrease the signals. This means that when the body’s naturally occurring protein binds in the receptor, allosteric modulators can either amplify the effect or reduce it depending on which type of allosteric modulators is being administered.
There are two different types of allosteric modulators: positive and negative. And as the label suggests, positive allosteric modulators (or PAMs) increase the signal from the receptor while negative allosteric modulators (or NAMs) reduce the signal.
So Dipraglurant turns down the volume of the signal from the mGluR5 receptor?
Exactly.
By turning down the volume of the glutamate receptor mGluR5, researchers believe that we can reduce the severity of dyskinesias.
But hang on a second. Why are we looking at glutamate in dyskinesias? Isn’t dopamine the chemical of interest in Parkinson’s disease?
So almost 10 years ago, some researchers noticed something interesting in the brains of Parkinsonian monkeys that had developed dyskinesias:
Title: mGluR5 metabotropic glutamate receptors and dyskinesias in MPTP monkeys. Authors: Samadi P, Grégoire L, Morissette M, Calon F, Hadj Tahar A, Dridi M, Belanger N, Meltzer LT, Bédard PJ, Di Paolo T. Journal: Neurobiol Aging. 2008 Jul;29(7):1040-51. PMID:17353071
The researchers conducting this study induced Parkinson’s disease in monkeys using a neurotoxin called MPTP, and they then treated the monkeys with L-dopa until they began to develop dyskinesias. At this point when they looked in the brains of these monkeys, the researchers noticed a significant increase in the levels of mGluR5, which was associated with the dyskinesias. This finding led the researchers to speculate that reducing mGluR5 levels might reduce dyskinesias.
And it did!
Subsequent preclinical research indicated that targeting mGluR5 might be useful in treating dyskinesias, especially with negative allosteric modulators:
Title: The mGluR5 negative allosteric modulator dipraglurant reduces dyskinesia in the MPTP macaque model Authors: Bezard E, Pioli EY, Li Q, Girard F, Mutel V, Keywood C, Tison F, Rascol O, Poli SM. Journal: Mov Disord. 2014 Jul;29(8):1074-9. PMID:24865335
In this study, the researchers tested the efficacy of dipraglurant in Parkinsonian primates that had developed L-dopa induced dyskinesias. They tested three different doses of the drug (3, 10, and 30 mg/kg).
Dipraglurant significantly reduced dyskinesias in the monkeys, with best effect being reached using the 30 mg/kg dose. Importantly, the dipraglurant treatment had no impact on the efficacy of L-dopa which was still being used to treat the monkeys Parkinson’s features.
This research lead to a clinical trials in man, and last year Addex Therapeutics published the results of their phase IIa clinical trial of Dipraglurant (also called ADX-48621):
Title: A Phase 2A Trial of the Novel mGluR5-Negative Allosteric Modulator Dipraglurant for Levodopa-Induced Dyskinesia in Parkinson’s Disease. Authors: Tison F, Keywood C, Wakefield M, Durif F, Corvol JC, Eggert K, Lew M, Isaacson S, Bezard E, Poli SM, Goetz CG, Trenkwalder C, Rascol O. Journal: Mov Disord. 2016 Sep;31(9):1373-80. PMID:27214664
The Phase IIa double-blind, placebo-controlled, randomised trial was a dose escalation study, conducted in 76 patients with Parkinson’s disease L-dopa-induced dyskinesia – 52 subjects were given dipraglurant and 24 received a placebo treatment. The dose escalation assessment of dipraglurant started at 50 mg once daily to 100 mg 3 times daily. The study was conducted over 4 weeks.
The investigators found that dipraglurant significantly reduced the dyskinesias on both day 1 of the study and on day 14, and this treatment did not result in any worsening of the Parkinsonian features. And remember that this was a double blind study, so both the investigators and the participants had no idea which treatment was being given to each subject. Thus little bias can influence the outcome, indicating that dipraglurant really is having a beneficial effect on dyskinesias.
The company suggested that dipraglurant’s efficacy in reducing L-dopa-induced dyskinesia warrants further investigations in a larger number of patients. And this is what the company is now doing with the help of the Michael J. Fox Foundation (MJFF). In addition, dipraglurant’s potential benefits on dystonia are also going to be investigated with support from the Dystonia Medical Research Foundation (DMRF).
And the really encouraging aspect of this research is that Addex Therapeutics are not the only research group achieving significant beneficial results for dykinesias using this treatment approach (click here to read about other NAM-based clinical studies for dyskinesias).
Fingers crossed for more positive results here.
What happens next?
L-dopa induced dyskinesias can be one of the most debilitating aspects of living with Parkinson’s disease, particularly for the early-onset forms of the condition. A great deal of research is being conducted in order to alleviate these complications, and we are now starting to see positive clinical results starting to flow from that research.
These results are using new type of therapeutic drug that are designed to increase or decrease the level of a signal occurring in a cell without interfering with the normal functioning of the chemicals controlling the activation of that signal.
This is really impressive biology.
The banner for today’s post was sourced from Steam
A build up of a protein called alpha synuclein inside neurons is one of the characteristic feature of the Parkinsonian brain. This protein is believed to be partly responsible for the loss of dopamine neurons in this condition.
A similar build up of alpha synuclein is also seen in the deadly skin cancer, Melanoma… but those cells don’t die (?!?)… in fact, they just keep on dividing.
Why is there this critical difference?
In today’s post we look at an interesting new study that may have solved this mystery.
The truly baffling detail in this story, however, is that this relationship is reciprocal – if you have melanoma you are almost 3 times more likely to develop Parkinson’s disease than someone without melanoma (Source: Baade et al 2007; Gao et al 2009).
What is melanoma exactly?
Melanoma is a type of skin cancer.
It develops from the pigment-containing cells known as melanocytes. Melanocytes are melanin-producing cells located in the bottom layer (the stratum basale) of the skin’s outer layer (or epidermis).
The location of melanocytes in the skin. Source: Wikipedia
Melanocytes produce melanin, which is a pigment found in the skin, eyes, and hair. It is also found in the brain in certain types of cells, such as dopamine neurons (where it is referred to as neuromelanin).
Neuromelanin (brown) in dopamine neurons. Source: Schatz
Melanomas are usually caused by DNA damage resulting from exposure to ultraviolet radiation. Ultraviolet radiation from tanning beds increases the risk of melanoma (Source), as does excessive air travel (Source), or simply spending to much time sun bathing.
Approximately 2.2% of men and women will be diagnosed with melanoma at some point during their lives (Source).In women, melanomas most commonly occur on the legs, while in men they are most common on the back. Melanoma makes up 5% of all cancers (Source).
Generally, melanomas is one of the safer cancers, as it can usually be detected early by visual inspection. This cancer is made dangerous, however, by its ability to metastasise (or spread to other organs in the body).
Are there any genetic associations between Parkinson’s disease and melanoma?
No.
When the common genetics mutations that increase the risk of both conditions were previously analysed, it was apparent that none of the known Parkinson’s mutations make someone more susceptible to melanoma, and likewise none of the melanoma-associated genetic mutations make a person vulnerable to Parkinson’s disease (Meng et al 2012;Dong et al 2014; Elincx-Benizri et al 2014).
In fact, researchers have only found very weak genetic connections between two conditions (Click here to read our previous post on this). It’s a real mystery.
Are there any other connections between Parkinson’s disease and melanoma?
Yes.
Another shared feature of both Parkinson’s disease and melanoma is the build up of a protein called alpha synuclein. Alpha synuclein is believed to be one of the villains in Parkinson’s disease – building up inside a cell, becoming toxic, and eventually killing that cell.
But recently researchers noticed that melanoma also has a build up of alpha synuclein, but those cells don’t die:
Title: Parkinson’s disease-related protein, alpha-synuclein, in malignant melanoma Authors: Matsuo Y, Kamitani T. Journal: PLoS One. 2010 May 5;5(5):e10481. PMID:20463956 (This article is OPEN ACCESS if you would like to read it)
In this study, researchers from Japan found that alpha synuclein was detected in 86% of the primary and 85% of the metastatic melanoma. Understand that the protein is not detectable in the non-melanoma cancer cells.
So what is it doing in melanoma cells?
Recently, researchers from Germany believe that they have found the answer to this question:
Title: Treatment with diphenyl-pyrazole compound anle138b/c reveals that α-synuclein protects melanoma cells from autophagic cell death Authors: Turriani E, Lázaro DF, Ryazanov S, Leonov A, Giese A, Schön M, Schön MP, Griesinger C, Outeiro TF, Arndt-Jovin DJ, Becker D Journal: Proc Natl Acad Sci U S A. 2017 Jun 5. pii: 201700200. doi: 10.1073/pnas.1700200114 PMID:28584093
In their study, the German researchers looked at levels of alpha synuclein in melanoma cells. They took the melanoma cells that produced the most alpha synuclein and treated those cells with a chemical that inhibits the toxic form of alpha synuclein (which results from the accumulation of the protein).
What they observed next was fascinating: the cell morphology (or physically) changed, leading to massive melanoma cell death. The investigators found that this cell death was caused by instability of mitochondria and a major dysfunction in the autophagy process.
Mitochondria, you may recall, are the power house of each cell. They keep the lights on. Without them, the lights go out and the cell dies.
Mitochondria and their location in the cell. Source: NCBI
Autophagy is the garbage disposal/recycling process within each cell, which is an absolutely essential function. Without autophagy, old proteins and mitochondria will pile up making the cell sick and eventually it dies. Through the process of autophagy, the cell can break down the old protein, clearing the way for fresh new proteins to do their job.
Waste material inside a cell is collected in membranes that form sacs (called vesicles). These vesicles then bind to another sac (called a lysosome) which contains enzymes that will breakdown and degrade the waste material. The degraded waste material can then be recycled or disposed of by spitting it out of the cell.
What the German research have found is that the high levels of alpha synuclein keep the mitochondria stable and the autophagy process working at a level that helps to keeps the cancer cell alive.
Next, they replicated this cell culture research in mice with melanoma tumors. When the mice were treated with the chemical that inhibits the toxic form of alpha synuclein, the cancer cancer became malformed and the autophagy process was blocked.
The researchers concluded that “alpha synuclein, which in PD exerts severe toxic functions, promotes and thereby is highly beneficial to the survival of melanoma in its advanced stages”.
So what does all of this mean for Parkinson’s disease?
Well, this is where the story gets really interesting.
You may be pleased to know that the chemical (called Anle138b) which was used to inhibit the toxic form of alpha synuclein in the melanoma cells, also works in models of Parkinson’s disease:
Title: Anle138b: a novel oligomer modulator for disease-modifying therapy of neurodegenerative diseases such as prion and Parkinson’s disease. Authors: Wagner J, Ryazanov S, Leonov A, Levin J, Shi S, Schmidt F, Prix C, Pan-Montojo F, Bertsch U, Mitteregger-Kretzschmar G, Geissen M, Eiden M, Leidel F, Hirschberger T, Deeg AA, Krauth JJ, Zinth W, Tavan P, Pilger J, Zweckstetter M, Frank T, Bähr M, Weishaupt JH, Uhr M, Urlaub H, Teichmann U, Samwer M, Bötzel K, Groschup M, Kretzschmar H, Griesinger C, Giese A. Journal: Acta Neuropathol. 2013 Jun;125(6):795-813 PMID:23604588 (This article is OPEN ACCESS if you would like to read it)
In this first study the researchers discovered Anle138b by conducted a large screening study to identify for molecules that could inhibit the toxic form of alpha synuclein.
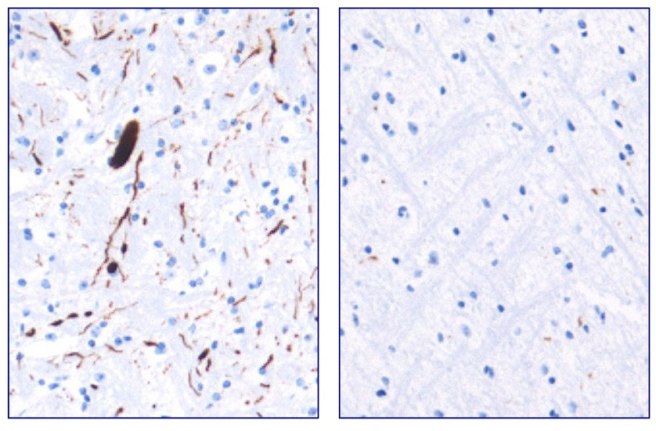
They next tested Anle138b in both cell culture and rodent models of Parkinson’s disease and found it to be neuroprotective and very good at inhibiting the toxic form of alpha synuclein. And the treatment looks to be very effective. In the image below you can see dark staining of toxic alpha synuclein in the left panel from the brain of an untreated mouse, but very little staining in the right panel from an Anle138b treated mouse.
Toxic form of alpha synuclein (dark staining). Source: Max-Planck
Importantly, Anle138b does not interfere with normal behaviour of alpha synuclein in the mice (such as production of the protein, correct functioning, and eventual degradation/disposal of the protein), but it does act as an inhibitor of alpha synuclein clustering or aggregation (the toxic form of the protein). In addition, the investigators found no toxic effects of Anle138b in any of their experiments even after long-term high-dose treatment (more than one year).
And in a follow up study, the drug was effective even if it was given after the disease model had started:
Title: The oligomer modulator anle138b inhibits disease progression in a Parkinson mouse model even with treatment started after disease onset Authors: Levin J, Schmidt F, Boehm C, Prix C, Bötzel K, Ryazanov S, Leonov A, Griesinger C, Giese A. Journal: Acta Neuropathol. 2014 May;127(5):779-80. PMID:24615514 (This article is OPEN ACCESS if you would like to read it)
During the first study, the researchers had started Anle138b treatment in the mouse model of Parkinson’s disease at a very young age. In this study, however, the investigators began treatment only as the symptoms were starting to show, and Anle138b was found to significantly improve the overall survival of the mice.
One particularly interesting aspect of Anle138b function in the brain is that it does not appear to change the level of the autophagy suggesting that the biological effects of treatment with Anle138b is cell-type–specific (Click here to read more about this). In cancer cells, it is having a different effect to that in brain cells. These differences in effect may also relate to disease conditions though, as Anle138b was not neuroprotective in a mouse model of Multiple System Atrophy (MSA; Click here to read more about this).
Is Anle138b being tested in the clinic?
Not yet.
Ludwig-Maximilians-Universität München and the Max Planck Institute for Biophysical Chemistry (Göttingen) have spun off a company called MODAG GmbH that is looking to advance Anle138b to the clinic (Click here for the press release). The Michael J Fox Foundation are helping to fund more preclinical development of this treatment (Click here to read more about this).
We will be watching their progress with interest.
What does it all mean?
Summing up: There are many mysteries surrounding Parkinson’s disease, but some researchers from Germany may have just solved one of them and at the same time developed a potentially useful new treatment.
They have discovered that the Parkinson’s associated protein, alpha synuclein, which is produced in large amounts in the skin cancer melanoma, is actually playing an important role in keeping those cancer cells alive. By finding a molecule that can block the build up of alpha synuclein, they have not only found a treatment for melanoma, but also potentially one for Parkinson’s disease.
And given that both diseases are closely associated, this could be seen as a great step forward. Two birds with one stone as the saying goes.
The banner for today’s post was sourced from Wikipedia




 Acetylcysteine. Source:
Acetylcysteine. Source: 

















































{kind=link}