
|
# # # # Numerous epidemiological studies have indicated that smoking might have a protective effect against developing Parkinson’s. As a result, researchers have long explored the neuroprotective potential of various ingredients in cigarettes. One of the active chemicals in smoking is nicotine, and preclinical research has reported that this stimulant has neuroprotective properties. Unfortunately, the results of a large clinical trial assessing nicotine treatment in people with Parkinson’s (called the NIC-PD trial) has not been able to demonstrate any protection. If anything, the results suggest that nicotine treatment made Parkinson’s worse. In today’s post, we will look at the epidemiological and preclinical data leading up to the NIC-PD study, we’ll review the results of the trial, and discuss what all of this means for Parkinson’s. # # # # |
Tavia Gordon. Source: Projecteuclid
In 1950, Dr Tavia Gordon noticed something interesting.
He observed that while the overall mortality rates for Japanese men in the USA and Japan were very similar, the incidence of heart disease was significantly lower in Japan. When he looked at Japanese men in Hawaii, he noticed that they were halfway between the other two cohorts.
He described his findings in this report:
 Title: Mortality experience among the Japanese in the United States, Hawaii, and Japan.
Title: Mortality experience among the Japanese in the United States, Hawaii, and Japan.
Author: Gordon T.
Journal: Public Health Rep (1896). 1957 Jun;72(6):543-53.
PMID: 13432134 (This report is OPEN ACCESS if you would like to read it)
Importantly, his observations led to the setting up of a major longitudinal study which became known as the Honolulu Heart Study.
Interesting, but what does this have to do with Parkinson’s?
Well, the original purpose of the Honolulu Heart study was to determine whether there was a difference in heart disease incidence between Japanese people living in Japan and individuals of Japanese ancestry living in Hawaii.
The participants recruited for the study were “non-institutionalized men of Japanese ancestry, born 1900-1919, resident on the island of Oahu.” In all, 12,417 men were identified as meeting the criteria. Of those contacted, 1,269 questionnaires were ‘return to sender’, 2,962 men declined to participate in the study, and 180 died before the study commenced. That left 8,006 participants who would be studied and agreed to be followed for the rest of their lives.
From October 1965 onwards, the participants were interviewed and given physical examinations every few years. The interview processed asked for:
- Family and personal history of illness
- Sociological history
- Smoking status
- Physical activity level
The physical examination was very thorough, looking at:
- ECG (Electrocardiography – electrical activity of the heart)
- Urine analysis
- Measurements of weight, height, skinfold thickness, etc.
- Blood pressure and serum cholesterol
As a result of this huge effort, the study built up a HUGE amount of epidemiological information regarding these 8,006 individuals.
Ok. Great. But again, what does this have to do with Parkinson’s????
Given the enormous number of individuals involved in the study and the length of time that they were followed, it was inevitable that a certain percentage of them would develop Parkinson’s as the study progressed. And as such, the Honolulu Heart Study represents one of the largest epidemiological study of Parkinson’s to date.
In 1994, a group of research involved in the study, published some very interesting findings relating to Parkinson’s.
This is the study:
 Title: Prospective study of cigarette smoking and the risk of developing idiopathic Parkinson’s disease.
Title: Prospective study of cigarette smoking and the risk of developing idiopathic Parkinson’s disease.
Authors: Grandinetti A, Morens DM, Reed D, MacEachern D.
Journal: American Journal of Epidemiology 1994 Jun 15;139(12):1129-38.
PMID: 8209872
In this study, the researchers reported that a total of 92 of the 8006 individuals enrolled in the Honolulu Heart study had developed Parkinson’s. The majority of the cases were diagnosed between 55 and 79 years of age (n=80). Diagnosis after the age of 80 was very rare. It is interesting to note that when the researchers divided the group into those ‘born before 1910’ and those ‘born after 1910’, the older group (born before 1910) had a lower incidence of Parkinson’s.
The researchers also found that men who had smoked cigarettes at any time prior to their enrollment in the study in 1965, had a reduced risk of developing Parkinson’s (relative risk = 0.39 – a relative risk of 1.0 would mean normal risk level, a number below 1.0 indicates reduced risk). The results appeared to be suggesting that smoking reduced the chance of developing Parkinson’s.
This finding was made alongside other interesting correlations (Note: coffee and alcohol also reduced the risk of Parkinson’s in this study):
 Source: Grandinetti et al (1994).
Source: Grandinetti et al (1994).
And a few years later the authors published a follow up paper which rejected the possibility that smoking was killing people before they could develop Parkinson’s (selective mortality representing a false positive).
This is that paper:
 Title: Evidence against the operation of selective mortality in explaining the association between cigarette smoking and reduced occurrence of idiopathic Parkinson disease.
Title: Evidence against the operation of selective mortality in explaining the association between cigarette smoking and reduced occurrence of idiopathic Parkinson disease.
Authors: Morens DM, Grandinetti A, Davis JW, Ross GW, White LR, Reed D.
Journal: Am J Epidemiol. 1996 Aug 15;144(4):400-4.
PMID: 8712197 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers found that the age-adjusted incidence rate of Parkinson’s in smokers was less than half that in nonsmokers (34.4 versus 94.2 cases per 100,000 person-years of pre-illness follow-up). They concluded that these data support a neuroprotective effect for smoking against Parkinson’s.
Wait. Are you saying smoking protects people against Parkinson’s?
That is what the initial data suggested.
EDITOR’S NOTE: THIS DOES NOT MEAN THAT EVERYONE SHOULD RUSH OUT AND START SMOKING. PLEASE DON’T DO THAT.
READ ON.
Subsequent independent studies found similar results.
For example:
 Title: Exploring causality of the association between smoking and Parkinson’s disease.
Title: Exploring causality of the association between smoking and Parkinson’s disease.
Authors: Gallo V, Vineis P, Cancellieri M, Chiodini P, Barker RA, Brayne C, Pearce N, Vermeulen R, Panico S, Bueno-de-Mesquita B, Vanacore N, Forsgren L, Ramat S, Ardanaz E, Arriola L, Peterson J, Hansson O, Gavrila D, Sacerdote C, Sieri S, Kühn T, Katzke VA, van der Schouw YT, Kyrozis A, Masala G, Mattiello A, Perneczky R, Middleton L, Saracci R, Riboli E.
Journal: Int J Epidemiol. 2019 Jun 1;48(3):912-925.
PMID: 30462234 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers collected data from the NeuroEPIC4PD study, a prospective European population-based cohort study involving 13 research centers in eight countries. A total of 715 Parkinson’s cases were identified in the broader cohort of 220,494 individuals. When the investigators looked at smoking habits, they found that former smokers had a 20% decreased risk and current smokers had a halved risk of developing Parkinson’s (compared with never smokers).
So, I should start smoking then?
No, that would not be a good idea.
Smoking is associated with all sorts of other health issues.
In addition, when researchers dig deeper, they find that smoking might not be good for people who have been diagnosed with Parkinson’s.
What do you mean?
Last year, this report was published:
 Title: Lifestyle factors and clinical severity of Parkinson’s disease.
Title: Lifestyle factors and clinical severity of Parkinson’s disease.
Authors: Gabbert C, König IR, Lüth T, Kasten M, Grünewald A, Klein C, Trinh J.
Journal: Sci Rep. 2023 Jun 12;13(1):9537.
PMID: 37308498 (This report is OPEN ACCESS if you would like to read it)
In this report, the researchers explored the association of life style factors (such as coffee drinking, aspirin intake, and smoking) with motor and non-motor symptoms in a cohort of 35,959 American patients who had been diagnosed with Parkinson’s. The data used was collected from the Michael J Fox Foundation’s Fox Insight Study.
 The results of their analysis indicated that people with Parkinson’s who smoked after their diagnosis had more problems with drooling, swallowing, & freezing of gait. Additionally, smokers also had more mood-related symptoms (unexplained pains, problems remembering, & feeling sad).
The results of their analysis indicated that people with Parkinson’s who smoked after their diagnosis had more problems with drooling, swallowing, & freezing of gait. Additionally, smokers also had more mood-related symptoms (unexplained pains, problems remembering, & feeling sad).
In another study, the investigators found that people with Parkinson’s who smoked tended to have fewer deaths from neurologic causes, but were significantly more likely to die from smoking-related cancers such as lung cancer (Click here to read more about that).
So it is not a good idea to start smoking after a diagnosis of Parkinson’s.
So how could smoking be having it’s protective effect before someone is diagnosed with Parkinson’s?
Well, cigarettes are full of lots of different chemicals, but the main active substance in tobacco is the stimulant nicotine.
Nicotine is a naturally produced alkaloid that has been shown to be neuroprotective in preclinical models of Parkinson’s. For example, this report demonstrated that smoking-relevant levels of nicotine had beneficial effects on stressed dopamine neurons:
 Title: Smoking-Relevant Nicotine Concentration Attenuates the Unfolded Protein Response in Dopaminergic Neurons.
Title: Smoking-Relevant Nicotine Concentration Attenuates the Unfolded Protein Response in Dopaminergic Neurons.
Authors: Srinivasan R, Henley BM, Henderson BJ, Indersmitten T, Cohen BN, Kim CH, McKinney S, Deshpande P, Xiao C, Lester HA.
Journal: J Neurosci. 2016 Jan 6;36(1):65-79.
PMID: 26740650 (This report is OPEN ACCESS if you would like to read it)
In this report, the researchers grew cells in culture and treated them with a chemical that caused stress (tunicamycin). They also treated some of the cells for 2 weeks with nicotine (200 nm – a dose equivalent to what humans receive from cigarette smoking, vaping, or a nicotine patch) and they found that the nicotine reduced levels of cellular stress and improved performance.
Other preclinical studies have demonstrated similar neuroprotective properties for nicotine (Click here, here, and read more about this). In fact, administration of nicotine was even found to be protective in a non-human primate model of Parkinson’s (Click here to read more about that).
Based on these findings, the German and U.S. Parkinson Study Groups initiated a clinical trial to assess the disease modifying potential of nicotine in people recently diagnosed with Parkinson’s.
That study was called NIC-PD and the results of that study have recently been published:
 Title: Transdermal Nicotine Treatment and Progression of Early Parkinson’s Disease.
Title: Transdermal Nicotine Treatment and Progression of Early Parkinson’s Disease.
Authors: Oertel WH, Müller HH, Unger MM, Schade-Brittinger C, Balthasar K, Articus K, Brinkman M, Venuto CS, Tracik F, Eberling J, Eggert KM, Kamp C, Kieburtz K, Boyd JT.
Journal: NEJM Evid. 2023 Sep;2(9):EVIDoa2200311.
PMID: 38320207
The NIC-PD study was a double-blind, placebo-controlled Phase 2 clinical trial conducted across 24 clinical sites in the USA and Germany. It involved 163 individuals with recently diagnosed Parkinson’s who were not yet taking any dopamine replacement therapy (such as levodopa). They were randomly assigned (a ratio of 1:1) to be treated with either a transdermal nicotine patch (up to 28 mg/day) or a transdermal placebo patch.
The treatment period of the study was 52 weeks followed by an 8 weeks washout period of no treatment. The primary end point of the study (this is the predetermined measure of success) was change in UPDRS parts I-III scores between baseline and 60 weeks (Click here to read more about the study).
The results of the study indicated no benefit from nicotine treatment.
In fact, there was actually a trend toward an acceleration in symptom progression. That is to say, a worsening of Parkinson’s symptoms.
The researchers reported that the UPDRS parts I–III score increased 3.5 points in the placebo arm (N = 54), but they saw a 6.0 points increase in the nicotine arm (N = 47, P = 0.056) over the 60 weeks of the study. An increase in score indicates worsening of symptoms. When the investigators looked at the scores of the participants at 52 weeks (before the washout period), they found an even greater worsening of symptoms in those on nicotine compared to placebo (P = 0.010).
So nicotine treatment might make Parkinson’s symptoms worse?
That is what the results of the NIC-PD study suggest.
So what does it all mean?
Smoking is a terrible habit.
Efforts by 1950/60s advertising executives to make it ‘cool’ have fallen flat on their face as lung cancer rates sky rocketed in the 1980/90s (especially for Australian males):
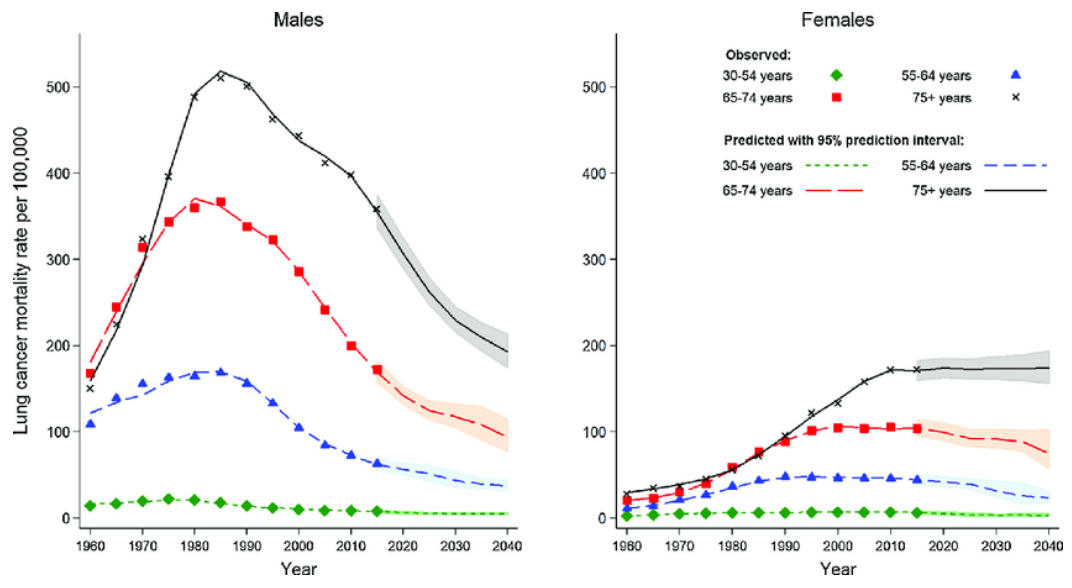 Source: Elsevier
Source: Elsevier
Overall, smoking was probably not a good move for humanity. The few benefits (alleviating stress levels during breaks at work, having something to do with your hands in social settings, looking cool, and reducing one’s risk of developing Parkinson’s) have been vastly outweighed by the tremendous cost and burden it has placed on our health care systems. And despite preclinical research demonstrating neuroprotective properties for some of the ingredients of smoking, the translation of those findings to humans has not provided any positive results to date.
The NIC-PD trial was a very interesting test of the neuroprotective potential of nicotine. The design of the study was clean and required nothing of the participants except to wear a patch. And the results were clear: Nicotine had no protective effect – if anything, the participants in the nicotine treatment arm were worse off than the placebo group. Thus, we can conclude that nicotine dose not appear to have any protective benefits for people with Parkinson’s.
There are of course other ingredients in smoking that could explain the “reduced risk of developing Parkinson’s” effect, and we will be exploring one of them in a future SoPD post. But for now, stay away from smoking folks. It’s not good for you.
Not good at all.
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
EDITOR’S NOTE: The author of this post is an employee of Cure Parkinson’s, so he might be a little bit biased in his views on research and clinical trials supported by the trust. That said, the trust has not requested the production of this post, and the author is sharing it simply because it may be of interest to the Parkinson’s community.
The information provided by the SoPD website is for information and educational purposes only. Under no circumstances should it ever be considered medical or actionable advice. It is provided by research scientists, not medical practitioners. Any actions taken – based on what has been read on the website – are the sole responsibility of the reader. Any actions being contemplated by readers should firstly be discussed with a qualified healthcare professional who is aware of your medical history. While some of the information discussed in this post may cause concern, please speak with your medical physician before attempting any change in an existing treatment regime.
In addition, many of the companies mentioned in this post are publicly traded companies. That said, the material presented on this page should under no circumstances be considered financial advice. Any actions taken by the reader based on reading this material is the sole responsibility of the reader. None of the companies have requested that this material be produced, nor has the author had any contact with any of the companies or associated parties. This post has been produced for educational purposes only.
The banner for today’s post was sourced from Bloomberg

For some reas
LikeLike
The recent demonstration that carbon monoxide induces expression of the anti-oxidant super-promoter Nrf-2 ( https://www.nature.com/articles/s41531-024-00763-6 ) offers a plausible mechanistic explanation for the smoking effect. Vitamin D is a promoter of Nrf-2. Sporadic PD is absent in the elderly rural-dwelling Massai of Kenya. This population is held as having our true, physiological D3 status. I dont smoke or inhale CO but I do take 4000 IU D3 daily to give me a Massai-like serum 25(OH)D of 125 nmol/L.
LikeLike