
|
|
Source: Youtube
In 2002, deep brain stimulation (or DBS) was granted approval for the treatment of Parkinson’s disease by the US Food and Drug Administration (FDA). The historical starting point for this technology, however, dates quite far back…
Further back than many of you may be thinking actually…
In his text “Compositiones medicamentorum” (46 AD), Scribonius Largo, head physician of the Roman emperor Claudius, first suggested using pulses of electricity to treat afflictions of the mind.

Roman emperor Claudius. Source: Travelwithme
He proposed that the application of the electric ray (Torpedo nobiliana) on to the cranium could be a beneficial remedy for headaches (and no, I’m not kidding here – this was high tech at the time!).

Torpedo nobiliana. Source: Wikipedia
These Atlantic fish are known to be very capable of producing an electric discharge (approximately 200 volts). The shock is quite severe and painful – the fish get their name from the Latin “torpere,” meaning to be stiffened or paralysed, referring specifically to the response of those who try to pick these fish up – but the shock is not fatal.
Now, whether Largo was ever actually allowed to apply this treatment to the august ruler is unknown, and beyond the point. What matters here is that physicians have been considering and using this approach for a long time. And more recently, the application of it has become more refined.
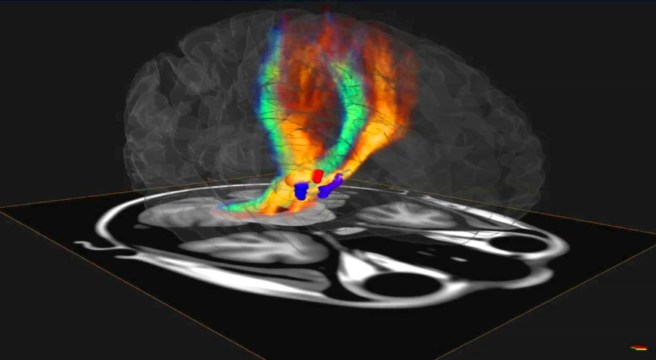
What is deep brain stimulation?
The modern version of deep brain stimulation is a surgical procedure in which electrodes are implanted into the brain. It is used to treat a variety of debilitating symptoms, particularly those associated with Parkinson’s disease, such as tremor, rigidity, and walking problems.














 Acetylcysteine. Source:
Acetylcysteine. Source: 










{kind=link}