
The influence of genetics in Parkinson’s disease is difficult to determine. If it was simply a genetic disease, identical twins – who share identical DNA – should show no difference in their susceptibility to Parkinson’s disease. They should either both develop the condition, or not. Right?
But this is not the case.
In today’s post we will review a particularly interesting pair of identical twins.
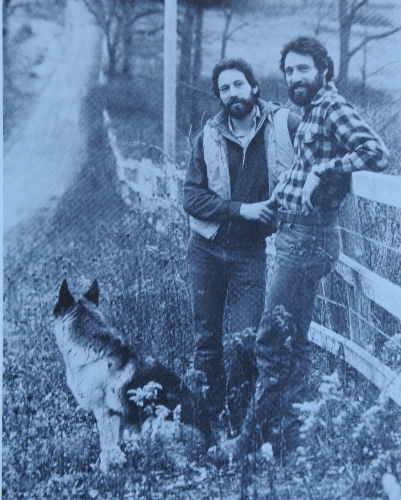
Jeff & Jack Gernsheimer in 1982. Source: ReadingEagle
When people ask the obvious question about the cause of Parkinson’s disease – ‘is it genetics or is it environment?’ – I have a standard answer: ‘it’s complicated’. I then tell them the curious story of identical twins Jeff and Jack Gernsheimer from eastern Pennsylvania. No other case better demonstrates the strange question of what causes Parkinson’s disease.
For almost their entire lives (69 years), Jeff and Jack have lived no more than half a mile apart. Breathing the same air, drinking the same water. They are literally neighbours – just a five-minute walk between their homes. In addition, since 1971 they have worked in the same office at a graphic design firm that they started together. The brothers were the focus of a story in the online magazine Nautilus last year. It’s a fantastic article and I fully recommend you read it.
So here’s the thing: In 2009 Jack was diagnosed with Parkinson’s disease.
To date, Jeff is yet to exhibit any signs of the condition.
Strange huh?
Two genetically identical people, living in the exact same environment and one of them develops Parkinson’s disease.
Ok, how do we explain this?
Hang on a second, slow down. I haven’t even got to the really interesting part yet:
After being diagnosed, Jack had his genome sequenced to see if there were any particular genetic mutations that might make him vulnerable to Parkinson’s disease. That analysis determined that Jack has a mutation in the most common Parkinson’s disease-associated gene: Glucocerebrosidase or GBA (which we have discussed in a previous blog post).
Interesting. So that explains the Parkinson’s disease?
No. Jack’s identical twin brother, Jeff, also has that exact same mutation.
So now we have a pair of identical twins who share the identical genetic code, live in the same environment, and have a genetic mutation associated with Parkinson’s disease, but only Jack has developed the condition while Jeff has not.
I think you will agree, it’s a really interesting tale… and with the help of modern science, it gets even more interesting.
How so?
In 2014, a research paper was published that utilized cells from both Jack & Jeff to determine what differences existed between them:

Title: iPSC-derived dopamine neurons reveal differences between monozygotic twins discordant for Parkinson’s disease.
Authors: Woodard CM, Campos BA, Kuo SH, Nirenberg MJ, Nestor MW, Zimmer M, Mosharov EV, Sulzer D, Zhou H, Paull D, Clark L, Schadt EE, Sardi SP, Rubin L, Eggan K, Brock M, Lipnick S, Rao M, Chang S, Li A, Noggle SA.
Journal: Cell Reports. 2014 Nov 20;9(4):1173-82.
PMID: 25456120 (this article is OPEN ACCESS if you would like to read it)
EDITOR’S NOTE HERE: Monozygotic means twins from the same egg, (as opposed to dizygotic meaning twins from two eggs). And discordant means ‘at variance, or at odds’ – in medicine it is used when one identical twin has a condition and the other does not.
The researchers conducting this study took skin cells from the brothers and they turned them into brain cells via a miraculous Nobel-prize winning approach. The technique firstly involves turning the skin cells into induced pluripotent stem cells (or iPS cells).

Source: Csiro
iPS cells can be used to make any cell you wish, and the researchers encouraged Jack and Jeff’s iPS cells to develop into dopamine neurons (one of the types of cells that are vulnerable in Parkinson’s disease).
When the researchers analysed the dopamine neurons from both twins, they found that both had half the normal levels GBA protein activity (an enzymatic reaction) due to the mutation in the GBA gene. The brother’s dopamine neurons also had approximately three times the normal levels of alpha-synuclein protein, and a reduced capacity to synthesize and release dopamine.

Dopamine neurons. Source: MindsofMalady
Then the researchers noticed something interesting: the dopamine cells from Jack (the affected twin) had lower dopamine levels than Jeff’s cells. This was rather strange: identical twins should actually have similar levels – all things being equal. The researchers attributed this decrease in dopamine to an increase in the levels of monoamine oxidase B (MAO-B) in Jack’s cells.
What is MAO-B?
Good question. MAO-B is an enzyme in dopamine neurons that helps to break down excess dopamine. After a cell releases dopamine, the cell will re-collect and recycle leftover/unused dopamine. MAO-B is the enzyme that breaks dopamine down. MAO-B inhibitors (such as Rasagiline or Azilect) have been used for some time as a therapy in Parkinson’s disease. By blocking MAO-B with MAO-B inhibitors, people with Parkinson’s disease can have increased levels of dopamine as the remaining dopamine does not get broken down so quickly.
The researchers studying Jack and Jeff’s iPS dopamine neurons found that by replacing the reduced GBA and inhibiting the oversupply of MAO-B (with MAO-B inhibitors) they made the dopamine neurons healthier – with an increase in dopamine levels and increased removal of excessive alpha-synuclein (the protein that is associated with Parkinson’s disease).
Are Jeff and Jack in a unique situation?
Nope. Not at all.
Here are some other examples:

Title: Pathology of PD in monozygotic twins with a 20-year discordance interval.
Author: Dickson D, Farrer M, Lincoln S, Mason RP, Zimmerman TR Jr, Golbe LI, Hardy J.
Journal: Neurology. 2001 Apr 10;56(7):981-2.
PMID: 11294946
This was a case study in which a pair of identical twins both developed Parkinson’s disease, but one of the twins was diagnosed 20 years before the other.

Title: Identical twins with Leucine rich repeat kinase type 2 mutations discordant for Parkinson’s disease.
Authors: Xiromerisiou G, Houlden H, Sailer A, Silveira-Moriyama L, Hardy J, Lees AJ.
Journal: Movement Disord. 2012 Sep 1;27(10):1323.
PMID: 22488887 (This article is OPEN ACCESS if you would like to read it)
This second case study involved a pair of twins who both carried a mutation in the Parkinson’s associated gene, Lrrk2 (click here to read more about this gene). They both developed Parkinson’s disease, but 10 years separated their diagnoses.
Title: Parkinson disease in twins: an etiologic study.
Authors: Tanner CM, Ottman R, Goldman SM, Ellenberg J, Chan P, Mayeux R, Langston JW.
Journal: JAMA. 1999 Jan 27;281(4):341-6.
PMID: 9929087 (This article is OPEN ACCESS if you would like to read it)
In this study, the scientists screened 19,842 white male twins enrolled in the National Academy of Sciences/National Research Council World War II Veteran Twins Registry. 163 pairs of twin were identified in which at least 1 twin had Parkinson’s disease (and medical records were available).
When diagnosis was made over the age of 50 years of age, approximately 10% of the twin pairs both had Parkinson’s disease (for both monozygotic and dizygotic twins). But when diagnosis was made under the age of 50, the monozygotic concordance was 100% – that is, all of the identical twins diagnosed under the age of 50 had Parkinson’s disease – while the dizygotic concordance remained around 10-20%. The researchers concluded that ‘this pattern strongly supports a primarily inherited cause of early-onset Parkinson’s disease’.
So how do we explain the difference seen in Jack and Jeff?
Some twins may be born with a vulnerability for Parkinson’s disease (like a genetic mutation, in the GBA or Lrrk2 gene for example), but there is some other factor/s that is influential in the initiation of the disease. And this is where scientists start talking about something called epigenetics (Epi, Greek for ‘over’ or ‘above’ and Genetics,…well, you should be able to work that one out).
Epigenetics is the study of changes in an organism that are caused by modifications or variations of gene expression rather than alteration of the genetic code itself. These variations may result from external factors that cause genes to turn on and off.

Source: 2ndActHealth
In the case of the Gernsheimer twins, if you read the story in the online magazine Nautilus you will find that their lives were not entirely the same. There were basic differences, for examples they went to different universities and in the 1970’s Jack enlisted in the army. But there were also some larger, life-altering differences: in the late 1980’s Jack lost a son in tragic circumstances. The brothers speculate that the stress/suffering associated with that particular event may have been a catalyst for the Parkinson’s that followed. Many researchers in the Parkinson’s disease field have speculated on whether a stressful/traumatic event in their lives was the causative agent for their Parkinson’s disease.
So what does it all mean?
It means that the answer is more complicated than first assumed.
And unfortunately, this is where I end up when people ask me about ‘genetics vs environment’ in the cause of Parkinson’s disease: a qualified we really don’t know. But I do always suggest that ‘Genetics vs environment’ may be too simplistic.
To finish, here is a nice, short video of the Gernsheimer twins discussing why they got involved in research:
The source of today’s banner was the AutismBlog.
























{kind=link}