Many members of the Parkinson’s community will have heard of deep brain stimulation – a surgical procedure that is offered to individuals with particularly bad tremor or dyskinesias – but there is now another form of stimulation that is now being tested in people with PD.
Spinal cord stimulation has long been used as a therapy for back pain and research groups have recently been asking if this technique could be applied to Parkinson’s.
In today’s post we will discuss some recently published data that points towards certain aspects of the motor features of Parkinson’s that could benefit from spinal cord stimulation, particularly freezing of gait.
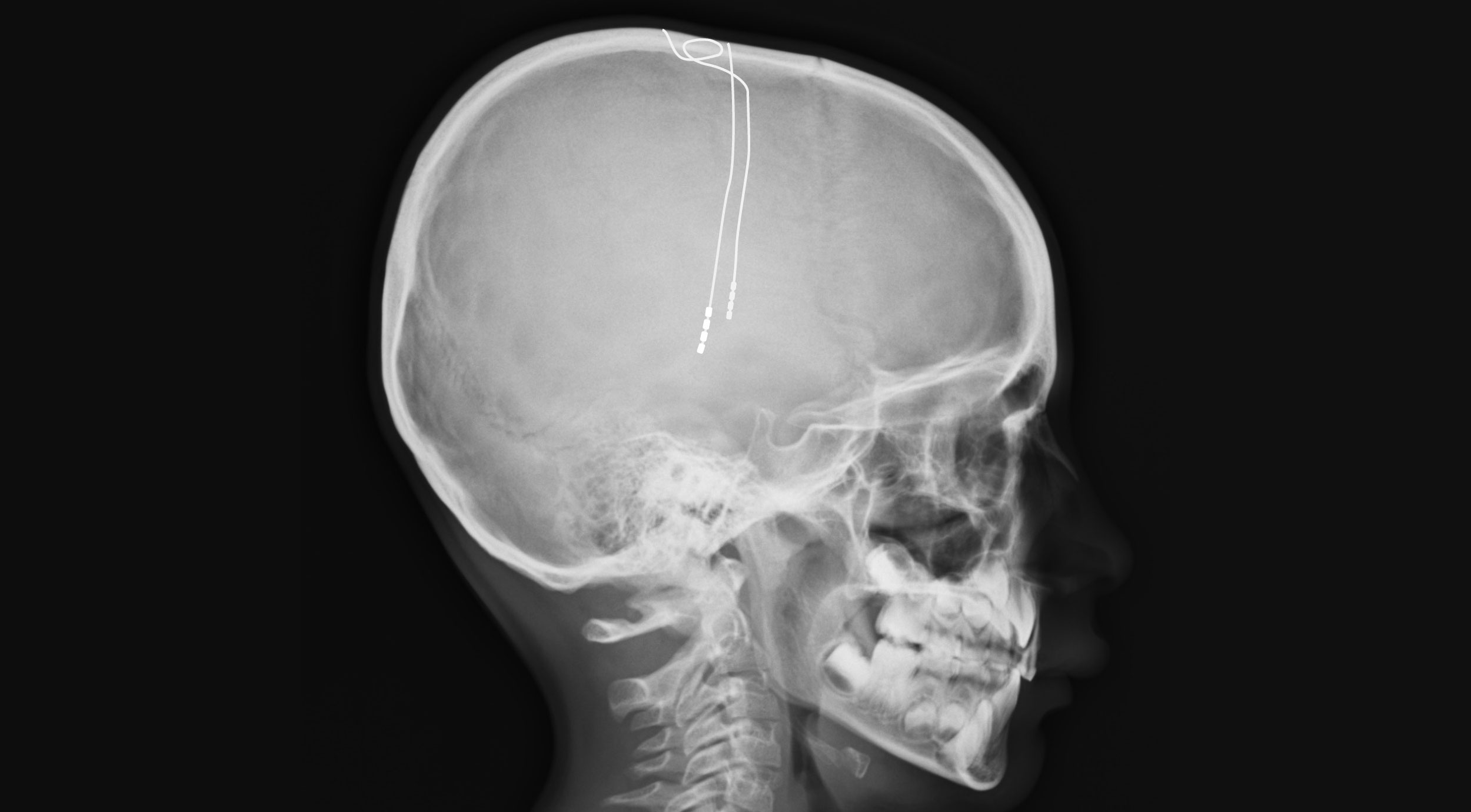
Deep brain stimulation electrodes implanted in the brain. Source: 2ndFriday
Deep brain stimulation (or DBS) has now become a routine treatment option for those in the Parkinson’s community with particularly debilitating motor features (such as severe tremor or dyskinesias).
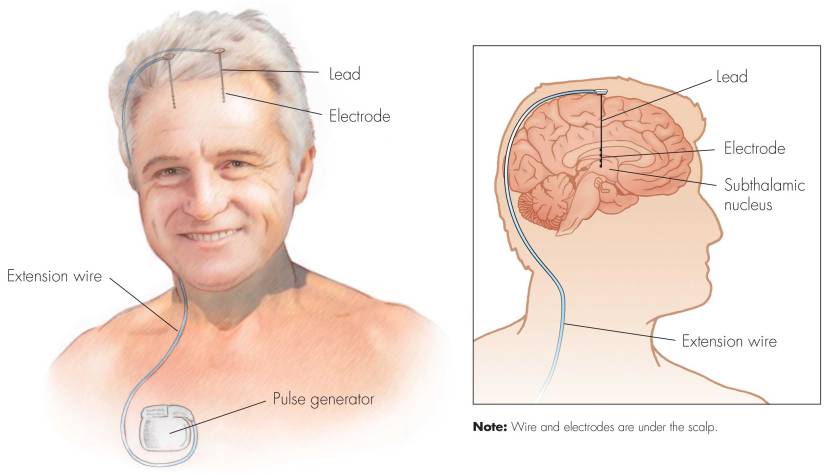
First introduced in 1987, deep brain stimulation consists of three components: the pulse generator, an extension wire, and the leads (which the electrodes are attached to). All of these components are implanted inside the body. Similar to a pace maker for the heart, the DBS system is turned on, programmed and turned off remotely.
The electrodes that are implanted deep in the brain are tiny, and the very tip of the electrode has small metal plates (each less than a mm in width) which provide the pulses that will help mediate the activity in the brain.
Deep brain stimulation (DBS) has now become a standard treatment option for people with Parkinson’s (Click here to read more about DBS), but recently researchers have been investigating a whole new form of stimulation to further help alleviate the symptom of the condition.
Spinal cord stimulation – the electrical modulation of the spinal cord – has been tested in models of Parkinson’s in laboratories for the last decade, and this week we saw the publication of the results of a pilot clinical study testing this approach in humans with Parkinson’s.
In today’s post we will discuss what spinal cord stimulation is, review the results of this pilot study, and discuss what could happen next for this new treatment approach.
2017 was the 200th anniversary of the first report of Parkinson’s by one James Parkinson in 1817 (Click here to read a previous post on this), and the 20th anniversary of the discovery of the first genetic mutation associated with Parkinson’s (Click here to read more about this).
It was also the 50th anniversary of the first use of a technique called spinal cord stimulation.
What is spinal cord stimulation?
Spinal cord stimulation is a form of implantable neuromodulation. Similar to deep brain stimulation (or DBS), it involves using electrical signals to modulate neural activity. But rather than electrodes being placed into the brain (in the case of DBA), spinal cord stimulation involves – as the label on the can suggests – specific areas of the spinal cord being stimulated for the treatment of certain types of pain.
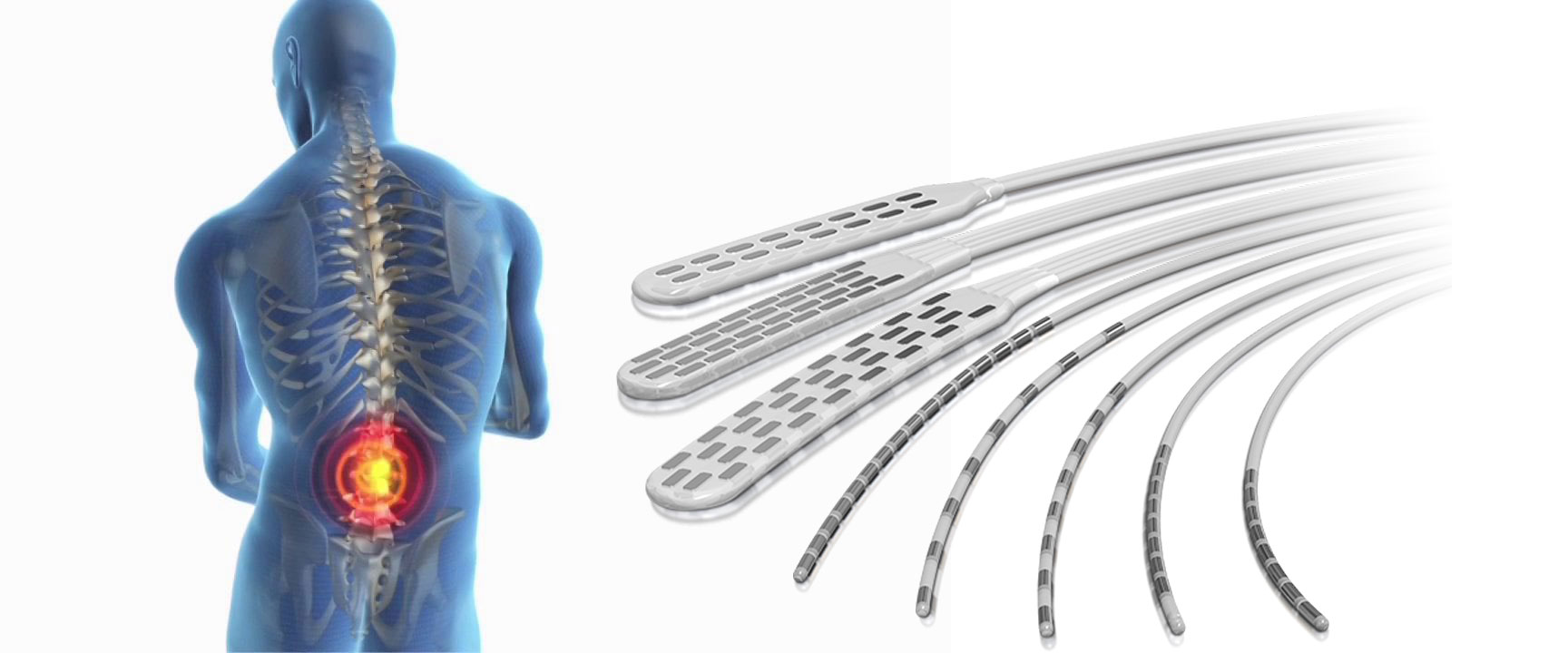
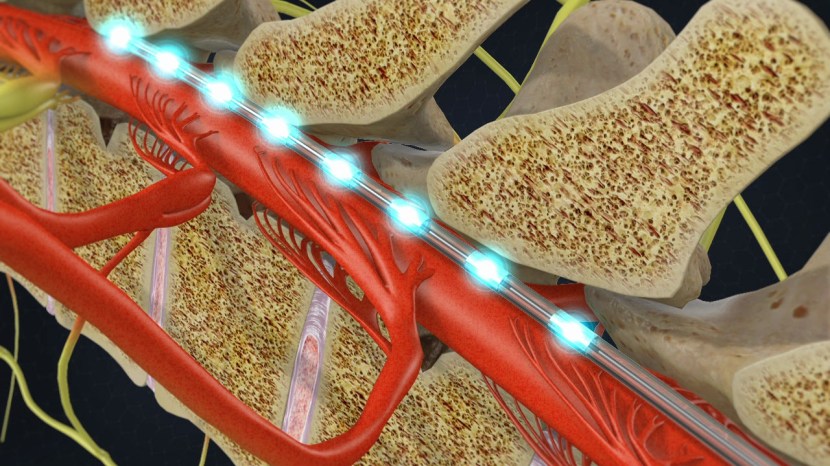
The treatment involves a column of stimulating electrodes that is surgically implanted in the epidural space of the spine. And before you ask: the epidural space is the area between the outer protective skin of the spinal cord (called the dura mater) and the surrounding vertebrae. So the device lies against the spinal cord, and is protected by the bones that make up the spine (as shown in the image below).
The stimulating electrodes within the epidural space. Source: SpineOne
An electrical pulse generator is implanted in the lower abdomen and conducting wires are connected between the electrodes to the generator. Much like deep brain stimulation, the system is entirely enclosed in the body and operated with a remote control.
An x-ray of the spine with a stimulator implanted (towards the top of the image, and cords leading off to the bottom left). Source:Wikipedia
As many readers will be aware from 2017 represents the 200 year anniversary of the first description of Parkinson’s disease by one Mr James Parkinson.
Many readers will not be aware, however, that 2017 is also represents the 50th anniversary of the first use of a technique called spinal cord stimulation:
What is spinal cord stimulation?
An x-ray of the spine with a stimulator implanted (towards the top of the image, and cords leading off to the bottom left). Source: Wikipedia
A spinal cord stimulator involves a small device being used to apply pulsed electrical signals to the spinal cord. It is generally used for pain relief, but it has recently been tested in a variety of other medical conditions.
The device is a column of stimulating electrodes that is surgically implanted in the epidural space of the spine. And before you ask: the epidural space is the area between the outer protective skin of the spinal cord (called the dura mater) and the surrounding vertebrae. So the device lies against the spinal cord, and is protected by the bones that make up the spine (as shown in the image below).
The stimulating electrodes within the epidural space. Source: SpineOne
An electrical pulse generator is implanted in the lower abdomen and conducting wires are connected between the electrodes to the generator. Much like deep brain stimulation, the system is entirely enclosed in the body and operated with a remote control.
How does spinal cord stimulation work?
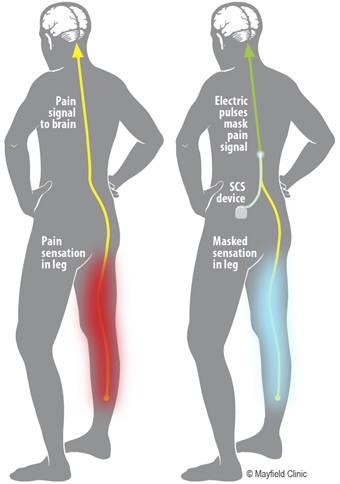
The stimulation basically interrupts the feeling of pain – blocking it from reaching the brain – substituting it with a more pleasing sensation called paresthesia (a kind of tingling or numbness).
The stimulation does not eliminate the source of pain, it simply masks it by interfering with the signal going to the brain. As a result the amount of relief from pain varies from person to person. In general, spinal cord stimulation resulting in a 50-70% reduction in pain.
But Parkinson’s results from inability to move, how would spinal cord stimulation work in Parkinson’s disease?
Yeah, this is a good question and the answer is not entirely clear, but the researchers (behind the research we discuss below) suggest that beneficial effects from spinal cord stimulation in Parkinson’s disease could be coming from direct activation of ascending pathways reaching thalamic nuclei and the cerebral cortex. That is to say (in plain English): activation of the spinal cord results in a signal going up into the brain where it alters the interaction between two of the regions involved in the initiation of movement (the thalamus and the cortex). And as we shall discuss below, there is evidence backing this idea.
Ok, so how much research has been done on spinal cord stimulation for Parkinson’s disease?
Actually quite a bit (in fact, for a good early review on the topic – click here).
The first real attempt at spinal cord stimulation for Parkinson’s disease was this report here:
Title: Spinal Cord Stimulation Restores Locomotion in Animal Models of Parkinson’s Disease Authors: Fuentes, R., Petersson, P., Siesser, W. B., Caron, M. G., & Nicolelis, M. A. L. Journal: Science (2009) 323(5921), 1578-1582. PMID:19299613 (This article is OPEN ACCESS if you would like to read it)
It was conducted by Prof Miguel Nicolelis and his colleagues at Duke University. Duke were kind enough to make this short video about the research:
In their research report, the scientists injected mice with a drug that reduced the level of dopamine in the brain (the tyrosine hydroxylase inhibitor alpha-methyl-para-tyrosine or AMPT). Similar to Parkinson’s disease, this resulted in a significant reduction in the movements of those mice. It also resulted in changes in the neuronal activity patterns of cells in an area of the brain called the motor cortex (we have talked about the motor cortex in a previous post). When the researchers then conducted spinal cord stimulation on these mice, they found that stimulation corrected both the loss of movement and the altered activity in the motor cortex.
The researchers then tested spinal cord stimulation in rats which had their dopamine system severely depleted (using the neurotoxin 6-OHDA), and they again found that the treatment could rescue the loss of locomotor ability. Curiously, spinal cord stimulation in the rats also caused an increase in locomotion activity after the stimulation period had stopped. On top of this, the researchers found that spinal cord stimulation aided the effect of L-dopa, allowing lower doses of L-dopa to achieve the same behavioural results as higher doses in animals not receiving spinal cord stimulation.
These initial results were then replicated in primates:
Title: Spinal cord stimulation alleviates motor deficits in a primate model of Parkinson disease. Authors: Santana MB, Halje P, Simplício H, Richter U, Freire MA, Petersson P, Fuentes R, Nicolelis MA. Journal: Neuron. 2014 Nov 19;84(4):716-22. PMID:25447740 (This article is OPEN ACCESS if you would like to read it)
In this study, the researchers modelled Parkinson’s disease in five adult marmosets using the neurotoxin 6-OHDA, which resulted in a reduction in spontaneous behaviour and a significant loss of dopamine neurons in the brain. They then implanted a spinal cord stimulator in each of the animals, which once activated resulted in a 200% improvement in some aspects of behavioural activity. Improvements observed in Parkinson’s-like features included freezing (31%), hypokinesia (23%), posture (23%), and bradykinesia (21%) as calculated by investigators blind to the treatment conditions of each subject.
In the brain, the researchers found that spinal cord stimulation resulted in similar improvements in neural activity as that seen with L-dopa treatment. Given all of these results, the investigators concluded that spinal cord stimulation “should be further tested in clinical studies aimed at measuring its long-term efficacy as a less invasive, long-term therapy for” people with Parkinson’s disease.
And it was not just Prof Nicolelis’ group that has achieved these results. Japanese researchers have also reported spinal cord stimulation having beneficial effects in models of Parkinson’s disease:
Title: Spinal cord stimulation exerts neuroprotective effects against experimental Parkinson’s disease. Authors: Shinko A, Agari T, Kameda M, Yasuhara T, Kondo A, Tayra JT, Sato K, Sasaki T, Sasada S, Takeuchi H, Wakamori T, Borlongan CV, Date I. Journal: PLoS One. 2014 Jul 10;9(7):e101468. PMID:25009993 (This article is OPEN ACCESS if you would like to read it)
In this report, the researchers actually found that spinal cord stimulation resulted in neuroprotection in a classical model of Parkinson’s disease (rodent 6-OHDA striatal delivery). Across three different levels of stimulation, the researchers reported better rescue of motor deficits and protection of dopamine neurons (particularly for 50Hz stimulation). The researchers also provided evidence suggesting that the neuroprotective effect might have something to do with a protein called Vascular endothelial growth factor (or VEGF). Interestingly, they found that the neuroprotective protein GDNF (that we have discussed before – click here for that post) was not involved.
So has this spinal stimulation procedure ever been conducted in humans with Parkinson’s disease before?
Yes, it has. But the results were a bit disappointing.
Title: Spinal cord stimulation failed to relieve akinesia or restore locomotion in Parkinson disease. Authors: Thevathasan W, Mazzone P, Jha A, Djamshidian A, Dileone M, Di Lazzaro V, Brown P. Journal: Neurology. 2010 Apr 20;74(16):1325-7. PMID:20404313 (This article is OPEN ACCESS if you would like to read it)
In this very small clinical study, just two people (both 75+ years of age) with Parkinson’s disease were fitted with spinal cord stimulators. Ten days after the surgery, the subjects participated in a blind analysis of the motor effects of spinal stimulation (blind analysis meaning that the assessors were not aware of their surgical treatment). The assessors, however, found no improvements as a result of the stimulation treatment.
This report lead to a letter to the journal from Prof Nicolelis and his colleagues:
In their letter, Prof Nicolelis and co point out several issues with the clinical study that may impact the final results (such as the tiny size of the study (only two participants) and the fact that the electrodes were located at a high cervical level, while in the rodent study they were located at a high thoracic level). In addition, the commercially available electrodes used in the human clinical study did not match the relative size or orientation of the electrodes used in the rodent study.
The researchers of the clinical study suggested that the beneficial motor effect described in the rodent study may be due to an increase in arousal (as a result of higher stimulation). But Prof Nicolelis and colleagues pointed out in their letter that their rodent study included three control experiments (including air puffs, trigeminal stimulation at the highest intensity tolerated by the animals, and direct measurements of changes in heart rate following spinal stimulation) which did not find a strong connection between arousal response and recovery seen in the level of locomotion.
The letter concluded that the results of the small clinical trial were inconclusive, and that further research in nonhuman primate models of Parkinson’s are required to determine the effects of electrode design and stimulation parameters. The doctors behind the clinical study agreed that more research is required.
And what do we know about this new clinical study?
Unfortunately, not very much.
The study is being conducted by Prof. Mandar Jog of Western University. Recently the Parkinson’s Society Southwestern Ontario provided some funding towards the study (Click here for more on this), but that is about as much as we could find on the work.
So what does it all mean?
Summing up: Spinal cord stimulation is a technique that is used to alleviate severe back pain. It has recently been proposed for Parkinson’s disease, resulting in several clinical trials. Here at the SoPD we are not sure what our opinion on spinal cord stimulation is at present, except that more research is obviously required.
If the results from the new clinical study (being conducted in Canada) indicate that spinal cord stimulation has beneficial effects for people with Parkinson’s disease, it would certainly represent a significant step forward for the community which relies heavily on symptom masking drugs at present. Before proceeding to wider clinical availability, however, larger clinical studies will be required to truly demonstrate safety and efficacy.
We’ll let you know if we hear anything else about this developing area of research.
The banner for today’s post was sourced from Greg Dunn