Some people say that the eyes are the gateway to the soul.
Maybe. I don’t know. Poetic stuff though.
Research published recently, however, suggests that the eyes may also provide a useful aid in the diagnosis of Parkinson’s disease. In today’s post we will review what results have been published and try to understand what they mean for our understanding of this condition.

A schematic of the human eyeball. Source: NIDDK image library
The fact that you can see and read this page is a miraculous thing.
Amazing not just because light is entering your eye, being focused on a particular point in the back of the eyeball and then being turned into a signal that is transmitted to your brain for further analysis, but also because of all the other activities involved with sight. The muscle movements, for example, which are required for turning the eyeball the small fractions necessary for reading this sentence from left to right.
And then there is also the blood supply, keeping the whole system working. This feature is of particular interest to today’s post, as research published last week suggests that there are differences in the blood flow of the eyeball between people with and without Parkinson’s disease.
The anatomy of an eyeball
The human eyeball is – on the macro level – a fairly simple structure.
You have the Iris, which regulates the amount of light entering the eye. At the centre of the iris, you have a central opening called the pupil, which can dilate and constrict as required. Covering these is the cornea, a transparent circular skin. These structures all sit over the lens which helps to refract incoming light and focus it onto the retina. And the retina, of course, is the light sensitive layer that lines the interior of the eye – allowing us to see.
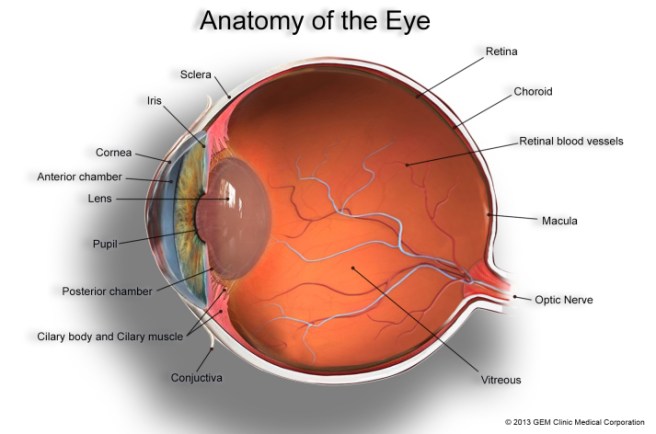
The anatomy of the eye. Source: GemClinic
Within the retina are specialised cells of two sorts:
- Rod cells (about 125 million of them per eye) which are necessary for seeing in dim light.
- Cone cells (6-7 million of these) which can be further divided into three types, each sensitive to different primary colours – red, green or blue.
These specialised ‘photoreceptive’ cells send signals down through the layers of the retina to what are called retinal ganglion cells which are the key conduits in the sending of information to the brain.
All of these cells require a constant blood supply, from arteries and veins spreading across the retina, and this a key part of our discussion today (see below).
So what have eyeballs got to do with Parkinson’s disease?
Good question. People with Parkinson’s disease often complain of from visual issues, such as reduced visual acuity, low contrast sensitivity and disturbed colour vision.
And there has been some research into the eyes with regards to Parkinson’s disease. A few weeks ago, this particular study was published:

Title: The retina as an early biomarker of neurodegeneration in a rotenone-induced model of Parkinson’s disease: evidence for a neuroprotective effect of rosiglitazone in the eye and brain.
Authors: Normando EM, Davis BM, De Groef L, Nizari S, Turner LA, Ravindran N, Pahlitzsch M, Brenton J, Malaguarnera G, Guo L, Somavarapu S, Cordeiro MF.
Journal: Acta Neuropathol Commun. 2016 Aug 18;4(1):86. doi: 10.1186/s40478-016-0346-z.
PMID: 27535749 (This article is OPEN ACCESS if you would like to read it)
The researchers in this study used a rodent model of Parkinson’s disease (rotenone-induced). In this model, the animals started losing dopamine cell loss in the brain at 60 days after the model of Parkinson’s disease was chemically induced.
The scientists examined the eyes of the rats at 10, 20, 40 and 60 days of the study. At the 20 day time point, the researchers began to see increased retinal ganglion cell death and swelling of the retinal layers in the eyes. These changes were obviously occurring well before the cell loss is observed in the brain, which leads the authors to ask whether the eyes could potentially used as an early indicator of Parkinson’s disease.
Of particular interest in this study was the use of Rosiglitazone to protect the retinal cells (AND the dopamine neurons in this rodent model of Parkinson’s disease). Rosiglitazone is an anti-diabetic drug. It works as an insulin sensitizer, by binding to fat cells and making them more responsive to insulin (we have previously discussed the curious relationship between Parkinson’s disease and diabetes (click here for more on this), and this result reinforces that connection). The scientists found that giving the drug once every 3 days had very beneficial effects of the survival of the retinal cells. They also observed significant neuroprotection after delaying the treatment for 10 days and then just giving one round of treatment, suggesting that a lot of the drug is not required for positive results.
EDITORIAL NOTE HERE: Before readers start to get any crazy ideas about sourcing and self medicating with Rosiglitazone, it is important to note that there are serious side effects associated with this class of drug. It has been associated with heart disease and stroke (click here to read more), and it should only be taken by people with diabetes and under the strict supervision of a qualified physician. It it mentioned here purely for educational purposes.
So obviously what is required is an examination of the eyes of people with Parkinson’s disease
Yep. And conveniently, in the same week as the previous study came out, this second study was also published:

Title: Evaluation of Retinal Vessel Morphology in Patients with Parkinson’s Disease Using Optical Coherence Tomography.
Authors: Kromer R, Buhmann C, Hidding U, Keserü M, Keserü D, Hassenstein A, Stemplewitz B.
Journal: PLoS One. 2016 Aug 15;11(8):e0161136.
PMID: 27525728 (This article is OPEN ACCESS if you would like to read it)
The researchers examined 49 people with Parkinson’s disease and 49 age- and sex-matched healthy controls. Blood vessels within the retina were identified and then divided into arteries and veins, based on their shape (using computer software). The results of the study indicate significant differences in the morphology of retinal veins in people with Parkinson’s disease when compared to controls.
Interestingly, the retinal effect was more significant on the side of the body firstly affected by Parkinson’s disease (a very common feature of Parkinson’s is that initially the condition will affect one side of the body more than the other).
What does it all mean?
For generations, we have focused on the clinical motor features of Parkinson’s disease (slowness, rigidity, and a resting tremor) when trying to determine if someone has the condition. Now we are learning that there may be other parts of the body that we should be investigating, which could not only provide us with novel diagnostic tools for earlier detection of the disease, but those areas may also provide us with new insights into disease onset and spread as well.
I may be getting a bit ahead of myself here but the possibilities are exciting and we’ll keep you abreast of these new findings as they come to us.
The banner for today’s post was sourced from the Photoforum.