A frequently used quote and sage words when analysing scientific data, especially clinical trial data.
Nilotinib is a cancer drug from Novartis that has the Parkinson’s community very excited. In October 2015, researchers at Georgetown University announced that a phase 1 open-label clinical study involving 12 people with Parkinson’s had demonstrated some pretty impressive results (click here to read more about this). The results of that first clinical trial have been published (click here to read more on this), but follow up studies have been hampered by study design issues (click here for more on this).
Today a letter to the editor of the Journal of Parkinson’s disease (published in this months issue) was brought to our attention (click here to read the letter). It queries one important aspect of the results from that first Nilotinib clinical trial for Parkinson’s disease.
In the letter, Prof Michael Schwarzschild of Massachusetts General Hospital (Boston) notes that 8 of the 11 subjects in the study had their monoamine oxidase-B (MAO-B) inhibitor treatment withdrawn less than a month after starting the trial. The change of treatment regime was made due to “increased psychosis in the first 2–4 weeks after Nilotinib administration”.
For reasons which we will outline below, a small change like this in a clinical trial could have major implications for the end results.
What are MAO-B inhibitors?
After the chemical dopamine is used by a neuron, it is reabsorbed by the dopamine cell and broken down for disposal. MAO-B is the enzyme that breaks down dopamine.
Selegiline is an example of a MAO-B inhibitor. Source: KnowMental
As the schematic above illustrates, dopamine is released by dopamine neurons and then binds to a receptor on a neighbouring cell. After this process has occurred, the dopamine detaches and it is reabsorbed by the dopamine neuron via a particular pathway called the dopamine transporter. Back inside the dopamine cell, dopamine is quickly broken down by the enzyme MAO-B into 3,4-Dihydroxyphenylacetic acid (or DOPAC).
Now, by blocking MAO-B, more dopamine is left hanging around inside the cell where it can be recycled and used again. Thus, this blockade increases the level of dopamine in the brain, which helps with alleviating the motor features of Parkinson’s disease. This simple concept has lead to the development of MAO-B inhibitors which are used in the treatment of the condition.
Why is this important to the Nilotinib results?
Dopamine is broken down by MAO-B into DOPAC. DOPAC can be further broken down into Homovanillic acid (HVA), and both DOPAC and HVA are often used in research studies to indicate levels of dopamine activity. Higher levels of both (in theory) should indicate higher levels of dopamine. It is a means of inferring greater dopamine production.
In the published results of the Nilotinib clinical trial, the researchers used increased HVA levels as an indication of greater dopamine production as a result of taking Nilotinib. But Prof Schwarzschild is correct in providing a cautionary warning of over-interpreting this result. You see, by discontinuing the treatment of MAO-B inhibitors shortly after starting the study, one would expect to see a rise in HVA levels regardless of any effect Nilotinib may be having. Without the MAO-B inhibitors, more dopamine will be broken down thus resulting in increased levels of HVA (compared to the baseline measurements at the start of the study).
And this issue is particularly important since HVA measurements taken at the start of the study (before the MAO-B inhibitors were removed) were compared with HVA measurement taken at the end of the study.
Another commentary discussing the Nilotinib results published in July of last year (in the same journal) actually questioned the value of measuring HVA levels, saying that prior studies have suggested that HVA levels can vary greatly between subjects at similar disease stages, and in general do not correlate well with disease progression.
Whether the removal of MAO-B inhibitors alters the overall interpretation of the first clinical study results is a subject for debate. Something interesting did appear to be happening in the participants involved in the first trial (whether this could have been a placebo effect could also be debated). Obviously, as Prof Schwarzschild’s letter indicates, what we really require now is a carefully designed, placebo-controlled, randomised clinical trial to determine if the initial results can be replicated.
And we are still awaiting news regarding a start date for that delayed trial.
With the end of the 2016, we thought it would be useful and interesting to provide an overview of where we believe things are going with Parkinson’s disease research in the new year. This post can be a primer for anyone curious about the various research activities, and food for thought for people who may have some fresh ideas and want to get involved with the dialogue.
Never before has so much been happening, and never before has there been greater potential for real change to occur. It is a very exciting time to be involved in this field, and it really does feel like we are on the cusp of some major discoveries.
In today’s post we will outline what to expect from Parkinson’s research in 2017.
Before we start: something important to understand –
The goal of most of the research being conducted on Parkinson’s disease is ultimately focused on finding a cure.
But the word ‘cure’, in essence, has two meanings:
The end of a medical condition, and
The substance or procedure that ends the medical condition
These are two very different things.
And in a condition like Parkinson’s disease, where the affected population of people are all at different stages of the disease – spanning from those who are not yet aware of their condition (pre-diagnosis) to those at more advanced stages of the disease – any discussion of a ‘cure for Parkinson’s disease’ must be temporal in its scope.
In addition to this temporal consideration, everyone is different.
A ‘cure’ for one person may not have an impact on another person – particularly when genetics is included in the equation. Currently there is a clinical trial which is only being tested on people with Parkinson’s disease who have a particular genetic mutation (Click here to read more about this).
With all of that said, there are 4 key areas of ongoing/future research:
Defining and understanding the biology of the condition
Early detection
Slowing/halting the disease
Replacing what has been lost
EDITOR’S NOTE HERE: While we appreciate that this list does not take into account important research dealing with the improving the day-to-day living and quality of life of those affected by Parkinson’s disease (such as prevention of falling, etc), we are primarily focusing here on finding a ‘cure’.
Let’s now have a look at and discuss each of these key areas of research:
The first key area of research feeds into all of the others.
It is only through a more thorough understanding of the mechanisms underlying Parkinson’s disease that we will be able to provide early detection, disease halting therapies, and cell replacement options. A better conception of the disease process would open doors in all of the other areas of research.
Given the slow pace of progress thus far, you will understand that this area of research is not easy. And it is made difficult by many issues. For example, it may be that we are blindly dealing with multiple diseases that have different causes and underlying mechanisms, but display the same kinds of symptoms (rigidity, slowness of movement and a resting tremor). Multiple diseases collectively called ‘Parkinson’s’. By not being able to differentiate between the different diseases, we have enormous confounding variables to deal with in the interpretation of any research results. And this idea is not as far fetched as it may sound. One of the most common observations within a group of people with Parkinson’s disease is the variety of disease features the group presents. Some people are more tremor dominate, while others have severe rigidity. Who is to say that these are not manifestations of different diseases that share a common title (if only for ease of management).
This complication raises the possibility that rather than being a disease, ‘Parkinson’s’ may actually be a syndrome (or a group of symptoms which consistently occur together).
Recently there have been efforts to deal with this issue within the Parkinson’s research community. We have previously written about the improved diagnostic criteria for Parkinson’s disease (click here to read that post). In addition, as we mentioned above, some new clinical trials are focusing on people with very specific types of Parkinson’s disease in which the subjects have a particular genetic mutation (Click here to read more about this). Better stratification of the disease/s will help us to better understand it. And with the signing into law of the 21 century Cures Act by President Obama, the Parkinson’s research community will have powerful new data collection tools to use for this purpose – in addition to more funding for research at the National Institute of Health (Click here to red more on this).
More knowledge of the basic biology of Parkinson’s disease is critical to the road forward. Whether the Parkinson’s disease-associated proteins, like alpha synuclein, are actually involved with the cell death associated with the condition is a question that needs to be resolved. If they are simply the bio-product of an alternative (unseen) disease process is important to know.
It is impossible to know what the new year will bring for new discoveries in the basic biology of Parkinson’s disease. Compared to 20 years ago, however, when the new discoveries were few and far between, 2017 will bring with it major new discoveries every month and we’ll do our best to report them here.
Early detection for Parkinson’s disease
Consider the impact of a pregnancy test on a person’s life. Source: Wikipedia
Ethically, the ‘early detection’ area of research can be a bit of a mine field, and for good reasons. You see, if we suddenly had a test that could accurately determine who is going to get Parkinson’s disease, we would need to very carefully consider the consequences of using it before people rush to start using it in the clinic.
Firstly there are currently no disease halting treatments, so early knowledge of future potential events may not be useful information. Second, there is the psychological aspect – such information (in light of having no treatment) may have a dramatic impact on a person’s mental wellbeing. And thirdly, such information would have huge implications for one’s general life (for example, individuals are legally bound to tell their banks and insurance companies about such information). So you see, it is a very tricky field to tackle.
Having said all of that, there are some very positive aspects to early detection of Parkinson’s disease. Early indicators (or biomarkers) may tell us something new about the disease, opening novel avenues for research and therapeutic treatments. In addition, early detection would allow for better tracking of the disease course, which would enhance our ideas about how the condition starts and changes over time.
There are numerous tests being developed – from blood tests (click here and here for posts we wrote about this topic) to saliva tests (again, click here for our post on this topic). There are even a simple urine test (click here for our post on this) and breath analysis test (click here for more on this) being developed. And there are ever increasing brain imaging procedures which may result in early detection methods (Click here for more on this).
How does the Parkinson’s research community study early detection of Parkinson’s disease though? Well, we already know that people with rapid eye movement (REM) sleep disorder problems are more likely to develop Parkinson’s disease. Up to 45 percent of people suffering REM sleep behaviour disorders will go on to develop Parkinson’s disease. So an easy starting point for early detection research is to follow these people over time. In addition, there are genetic mutations which can pre-dispose individuals to early onset Parkinson’s disease, and again these individuals can be followed to determine common ‘biomarkers’ (aspects of life that are shared between affected individuals). Epidemiological studies (like the Honolulu Heart study – click here for more on this) have opened our eyes to keep features and aspects of Parkinson’s disease that could help with early detection as well.
One of the most significant findings in Parkinson’s disease research over the last few years has been the discovery that transplanted dopamine cells can develop Lewy bodies over time. It is very important for everyone to understand this concept: healthy embryonic cells were placed into the Parkinsonian brain and over the space of one or two decades some of those cells began to display the key pathological feature of Parkinson’s disease: dense, circular clusters of protein called Lewy bodies.
The implications of this finding are profound: Healthy cells (from another organism) developed the features of Parkinson’s disease. And this is (presumably) regardless of the genetic mutations of the host. It suggests that the disease spreads by being passed from cell to cell. There is a very good open-access article about this in the journal Nature (click here to read that article).
Slowing down the progression of Parkinson’s disease is where most of the new clinical trials are focused. There are numerous trials are focused on removing free-floating alpha synuclein (the main protein associated with Parkinson’s disease). This is being done with both vaccines and small molecules (such as antibodies). Beyond possibly slowing the disease, whether these clinical trials are successful or not, they will most definitely provide an important piece of the puzzle that is missing: is alpha synuclein involved with the spread of the disease? If the trials are successful, this would indicate ‘Yes’ and by blocking alpha synuclein we can slow/halt the spread of the disease. If the trials fail, this would suggest that alpha synuclein is not responsible, and indicate that we need to focus our research attention elsewhere.
2017 will be very big year for Parkinson’s disease as some of these clinical trials will be providing our first glimpse at resolving this major question.
Replacing what is lost
Cell transplantation for Parkinson’s disease. Source: AtlasofScience
So if we discover a means of stopping the disease with a vaccine or a drug, this will be fantastic for people who would be destined to develop the condition… but what about those still living with the disease. Halting the condition will simply leave them where ever they are on the course of the disease – a rather unappealing situation if one is in the latter stages of the condition.
Cell transplantation is one means of replacing some of the cells that have been lost in this disease. Most of the research is focused on the dopamine neurons whose loss is associated with the appearance of the movement features of Parkinson’s disease.
Unfortunately, this area of research is more ‘blue sky’ in terms of its clinical application. It will be some time before cell transplantation has a major impact on Parkinson’s disease. And while many research groups have plans to take this approach to the clinic, there are currently just two ongoing clinical trials for cell transplantation in Parkinson’s disease:
The former is behind schedule due to the technical matters (primarily the source of the tissue being transplanted) and the latter is controversial to say the least (click here and here to read more). In the new year we will be watching to see what happens with a major research consortium called G-Force (strange name we agree). They are planning to take dopamine neurons derived from embryonic stem cells to clinical trials in 2018. Embryonic stem cells represents a major source of cells for transplantation as they can be expanded in a petri dish (millions of cells from just one cell). If they can be pushed in the right direction and they develop into dopamine neurons, they would allow people to start having some of the cells that they have lost to Parkinson’s disease to be replaced.
Above we have discussed the key areas of Parkinson’s disease (dealing with ‘finding a cure’) for 2017. We would love to hear your thoughts on them. If not, here on the SoPD, then somewhere else. Please get involved with the discussion in which ever forum you choose. Speak up and add your personal account of things to the discussion.
It is only through the sharing of ideas, information, and experiences that we are going to figure out this debilitating condition.
And now we are going to change focus and discuss what we are expecting/hoping for in the new year (particularly from the clinical side of things):
Recently some major players have come together to focus on Parkinson’s disease:
Bayer and healthcare investment firm Versant Ventures joined forces to invest $225 million in stem-cell therapy company BlueRock Therapeutics. This venture will be focused on induced pluripotent stem cell (iPSC)-derived therapeutics for cardiovascular disease and neurodegenerative disorders, particularly Parkinson’s disease (co-founders Lorenz Studer and Viviane Tabar are world renowned experts in the field of cell transplantation for Parkinson’s disease). Importantly, BlueRock has acquired rights to a key iPSC intellectual property from iPS Academia Japan, and with 4 years of funding they will be looking to make things happen (Click here to read more on this).
Evotec and Celgene are also jumping into the IPS cell field, but they are collaborating to screen for novel drug targets. (Click here to read more on this).
For a long time we have been hearing that the major tech company Apple is working on software and devices for Parkinson’s disease. They already provide ResearchKit and CareKit software/apps. Hopefully in the new year we will hear something about their current projects under development (Click here to read more on this).
In February of 2016, seven of the world’s largest pharmaceutical companies signed up to Critical Path for Parkinson’s set up by Parkinson’s UK. It will be interesting in the new year to see what begins to develop from this initiative.
Parkinson’s UK has also set up the Virtual Biotech, which is looking at providing faster means for new drugs to be brought to market. Hopefully this will take off in 2017.
In addition, there are many clinical trials starting and also announcing results. Here are the top 20 that we are keeping an eye on:
Herantis Pharma, a Finnish pharmaceutical company, will begin recruiting 18 people with Parkinson’s disease for their Conserved Dopamine Neurotrophic Factor (or CDNF) clinical trial. CDNF is very similar to GDNF which we have previously discussed on this site (Click here for that post). Herantis will be collaborating with another company, Renishaw, to deliver the CDNF into the brain (Click here to read more on this trial).
The results of the double-blind, placebo controlled clinical study of the diabetes drug Exenatide will be announced in 2017. We have previously discussed this therapy (click here and here for more on this), and we eagerly await the results of this study.
AAV2-hAADC, which is a gene therapy treatment – a virus that works by allowing cells in the body other than neurons to process levodopa. The results of the phase one trial were successful (click here to read about those results) and the company (Voyager Therapeutics) behind the product are now preparing for phase 2 trials (Click here for more on this).
Donepezil (Aricept®) is an Alzheimer’s therapy that is being tested on dementia and mild cognitive impairment in Parkinson’s disease (Click here for more on this trial).
Oxford Biomedica is attempting to proceed with their product, OXB-102, which is a gene therapy treatment – a virus that modifies neurons so that they produce dopamine. Phase 1 successful, but did not show great efficacy. Phase 2 is underway but not recruiting (click here for more on this trial).
Biotie is proceeding with their product, SYN120, which is new class of combination drug (dual antagonist of the serotonergic 5-HT6 and 5-HT2A receptors) which is being tested as a treatment of cognition and psychosis in Parkinson’s disease (Click here for more on this).
Acorda Therapeutics is continuing to take the new inhalable form of L-dopa, called CVT-301 to the clinic. Phase 1 trials were successful (Click here and here to read more) and phase 2 trials are being planned.
Related to caffeine, Istradefylline, is an A2A receptor antagonist, already approved in Japan, that is designed to reduce “off” time and suppress dyskinesias. Phase 1 testing was successful (Click here for more on this) and phase 2 trials are being planned.
Another product from Biotie, Tozadenant, is an A2A receptor antagonist designed to reduce “off” time and suppress dyskinesias.
UniQurewas developing AAV2-GDNF – A gene therapy treatment – a virus designed to deliver GDNF (a naturally occurring protein that may protect dopamine neurons) in the brain (Click here for more on this trial). The company has recently announced cost cutting, however, and removed AAV2-GDNF from it’s list of products under development, so we are unsure about the status of this product.
AstraZeneca are taking their myeloperoxidase (MPO) inhibitor, AZD3241, through phase 2 trials at the moment (Click here for more on this trial). Oxidative stress/damage and the formation of excessive levels of reactive oxygen species plays a key role in the neurodegeneration associated with Parkinson’sdisease. MPO is a key enzyme involved in the production of reactive oxygen species. By blocking it, AstraZeneca hopes to slow/halt the progression of Parkinson’s disease.
Genervon Biopharmaceuticals will be hopefully be announcing more results from their phase 2 clinical trial of GM 608 (Click here for more on the trial). GM 608 has been shown to protect neurons against inflammatory factors floating around in the brain. Initial results looked very interesting, though the study was very small (Click here for more on those results).
Neurimmune (in partnership with Biogen) is proceeding with their product, BIIB054, which is an immunotherapy – an antibody that clears free floating alpha-synuclein in an attempt to halt the spread of the disease (Click here for more on this trial).
Neuropore is continuing to move forward with their product, NPT200-11, which is a drug designed to stabilize alpha-synuclein, preventing it from misfolding and aggregating. Phase 1 trial was successful (Click here and here to read more on this). Phase 2 trials are being planned.
Prothena are very pleased with their product, PRX002 (an immunotherapy – an antibody that clears free floating alpha-synuclein in an attempt to halt the spread of the disease (similar to BIIB054 described above)). Phase 1 trials were successful (Click here for more on this).
Edison Pharma is currently conducting a phase 2 trial of Vatiquinone on Visual and Neurological Function in Patients with Parkinson’s Disease (Click here for more on this trial). Vatiquinone modulates oxidative stress by acting on the mitochondria on cells.
Isradipine (Prescal®) – a calcium channel blocker that is approved for treatment of high blood pressure – is being tested in Parkinson’s disease by the Michael J Fox Foundation (Click here for more on this).
Inosine – which is a nutritional supplement that converts to urate, a natural antioxidant found in the body – is going to be tested in a phase 3 clinical trial (Click here for more on that trial).
In 2015, Vernalis has licensed its adenosine receptor antagonist programme (including lead compound V81444) to an unnamed biotech company. We are hoping to see the results of the phase 1 trial that was conducted on V81444 for Parkinson’s disease sometime in the new year (Click here to read more about that trial).
And finally, we are hoping to see progress with Nilotinib (Tasigna®) – A cancer drug that has demonstrated great success in a small phase 1 trial of Parkinson’s disease. Unfortunately there have been delays to the phase 2 trial due to disagreements as to how it should be run (Click here to read more). We have been following this story (Click here and here and here to read more), and are very disappointed with the slow progress of what could potentially be a ‘game-changer’ for the Parkinson’s community. Hopefully the new year will bring some progress.
Please note that this is not an exhaustive list – we have missed many other compounds being tested for Parkinson’s disease. For example there are always alternative versions of products currently on the market being tested in the clinic (eg. new L-dopa products). We have simply listed some of the novel approaches here that we are particularly interested in.
EDITORIAL NOTE HERE: All of the team at the SoPD wants to wish everyone a very enjoyable festive season where ever you are. And all the very best for the new year!
Last week a research report was published in the prestigious journal Science Translational Medicine (that means that it’s potentially really important stuff). The study involved a new drug that is being clinically tested for diabetes.
In last week’s study, however, the new drug demonstrated very positive effects in Parkinson’s disease.
In today’s post we will review the new study and discuss what it means for Parkinson’s.
FACT: One in every 19 people on this planet have diabetes (Source: DiabetesUK).
It is expected to affect one person in every 10 by 2040.
Diabetes (or ‘Diabetes mellitus’) is basically a group of metabolic diseases that share a common feature: high blood sugar (glucose) levels for a prolonged period. There are three types of diabetes:
Type 1, which involves the pancreas being unable to generate enough insulin. This is usually an early onset condition (during childhood) and is controlled with daily injections of insulin.
Type 2, which begins with cells failing to respond to insulin. This is a late/adult onset version of diabetes that is caused by excess weight and lack of exercise.
Type 3, occurs during 2-10% of all pregnancies, and is transient except in 5-10% of cases.
In all three cases inulin plays an important role.
What is insulin?
Insulin is a chemical (actually a hormone) that our body makes, which allows us to use sugar (‘glucose’) from the food that you eat.
Glucose is a great source of energy. After eating food, our body releases insulin which then attaches to cells and signals to those cells to absorb the sugar from our bloodstream. Without insulin, our cells have a hard time absorbing glucose. Think of insulin as a “key” which unlocks cells to allow sugar to enter the cell.
What does diabetes have to do with Parkinson’s disease?
So here’s the thing: 10–30% of people with Parkinson’s disease are glucose intolerant (some figures suggest the percentage may be as high as 50%).
Why?
We do not know.
Obviously, however, this ratio is well in excess of the 6% prevalence rate in the general public (Source:DiabetesUK). We have discussed the curious relationship between diabetes and Parkinson’s disease in a previous post (click here to read it).
And the relationship between Parkinson’s disease and diabetes is not a one way street: A recent analysis of 7 large population studies found that people with diabetes are almost 40% more likely to develop Parkinson’s disease that non-diabetic people (Click here for more on this).
EDITORIAL NOTE HERE: We would like to point out that just because a person may have diabetes, it does not necessarily mean that they will go on to develop Parkinson’s disease. There is simply a raised risk of developing the latter condition. It is good to be aware of these things, but please do not panic.
We have no idea why there is an association between diabetes and Parkinson’s disease, but each month new pieces of research are published that support the connection between Parkinson’s and diabetes, and this all provides encouraging support for an ongoing clinical trial (which we will discuss below).
So what research has been done?
Well, just this year alone there have been some interesting studies reported. The first piece of research deals with a drug that is used for treating type-2 diabetes:
Title: Metformin Prevents Nigrostriatal Dopamine Degeneration Independent of AMPK Activation in Dopamine Neurons. Author: Bayliss JA, Lemus MB, Santos VV, Deo M, Davies JS, Kemp BE, Elsworth JD, Andrews ZB. Journal: PLoS One. 2016 Jul 28;11(7):e0159381. PMID:27467571 (This article is OPEN ACCESS if you would like to read it)
Metformin (also known as Glucophage) has been one of the most frequently prescribed drugs for the treatment of type 2 diabetes since 1958 in the UK and 1995 in the USA. The mechanism by which Metformin works is not entirely clear, but it does appear to increase the body’s ability to recognise insulin.
Metformin treatment has previously been found to be neuroprotective. The researchers in this study wanted to determine if a protein called ‘AMPK’ was involved in that neuroprotective effect. They generated cells that do not contain AMPK and grew dopamine neurons – the brain cells badly affected by Parkinson’s disease.
In both cell cultures and in mice, the researchers found that Metformin was neuroprotective both in normal conditions and in the absence of AMPK. The study could not explain how the neuroprotective potential of Metformin was working, but it adds to the accumulating pile of evidence that some diabetes treatments may be having very positive effects in Parkinson’s disease.
A second piece of research from early this year goes even further:
Title: Reduced incidence of Parkinson’s disease after dipeptidyl peptidase-4 inhibitors-A nationwide case-control study. Authors: Svenningsson P, Wirdefeldt K, Yin L, Fang F, Markaki I, Efendic S, Ludvigsson JF. Journal: Movement Disorders 2016 Jul 19. PMID:27431803
Using the Swedish Patient Register, the researchers of this study identified 980 people with Parkinson’s disease who were also diagnosed with type 2 diabetes between July 1, 2008, and December 31, 2010. For comparative sake, they selected 5 controls (non-Parkinsonian) with type 2 diabetes (n = 4,900) for each of their Parkinsonian+diabetic subjects. Their analysis found a significant decrease in the incidence of Parkinson’s disease among individuals with a history of DPP-4 inhibitor intake.
DPP-4 inhibitors work by blocking the action of DPP-4, which is an enzyme that destroys the hormone incretin. Incretin helps the body produce more insulin only when it is needed and reduce the amount of glucose being produced by the liver when it is not needed. By blocking DPP-4, we are increasing the production of insulin.
Authors concluded that ‘clinical trials with DPP-4 inhibitors may be worthwhile’ in people with Parkinson’s disease.
So what was published last week?
Metabolic Solutions Development is a Kalamazoo (Michigan)-based company that is developing a new drug (MSDC-0160) to treat type 2 diabetes. Last week, Prof Patrik Brundin and colleagues from the Van Andel Institute in Grand Rapids published a research report that suggested MSDC-0160 may have very beneficial effects in Parkinson’s disease:
Title: Mitochondrial pyruvate carrier regulates autophagy, inflammation, and neurodegeneration in experimental models of Parkinson’s disease. Authors: Ghosh A, Tyson T, George S, Hildebrandt EN, Steiner JA, Madaj Z, Schulz E, Machiela E, McDonald WG, Escobar Galvis ML, Kordower JH, Van Raamsdonk JM, Colca JR, Brundin P. Journal: Sci Transl Med. 2016 Dec 7;8(368):368ra174. PMID:27928028
The drug from Kalamazoo, MSDC-0160, functions by reducing the activity of a recently identified protein that carries pyruvate into mitochondria.
What does this mean?
Pyruvate is a very important molecule in our body. The body can make glucose from pyruvate through a process called gluconeogenesis, which simply means production of new glucose. Thus, pyruvate is essential in providing cells with fuel to create energy (for more on pyruvate, click here for a good review article).
Pyruvate is carried into the power house of the cell – the mitochondria – by a protein called mitochondrial pyruvate carrier (MPC). The drug from Kalamazoo, MSDC-0160, is a blocker of MOC. It reduces the activity of MPC.
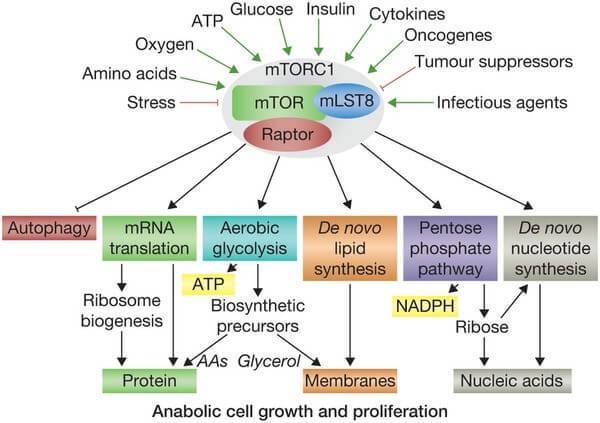
MPC also has other functions. It is known to be a key controller of certain cellular processes that influences mammalian target of rapamycin (mTOR) activation. mTOR responds to signals to nutrients, growth factors, and cellular energy status and controls the cells response. For example, insulin can signal to mTOR the status of glucose levels in the body. mTOR also deals with infectious or cellular stress-causing agents, thus it could be involved in a cells response to conditions like Parkinson’s disease.
Given the interaction with mTOR, the researchers in Michigan hypothesised that MSDC-0160 might reduce the neurodegeneration of dopaminergic neurons in animal models of Parkinson’s disease.
And this is exactly what they found.
The researchers reported that MSDC-0160 protected dopamine neurons in a mouse model of Parkinson’s disease. It also protected human midbrain dopamine neurons grown in cell culture when they were exposed to a toxic chemical. In addition, it demonstrated neuroprotective effects in a worm (called Caenorhabditis elegans) that produces a lot of the parkinson’s related protein alpha synuclein. MSDC-0160 even slowed the cell loss observed in a genetically engineered mouse that exhibits a slow loss of dopamine neurons. Basically, treatment with MSDC-0160 protected the cells from whatever the researcher threw at them.
How did it do this?
The researchers found that MSDC-0160 was reducing mTOR activity and also initiating a process called autophagy (which is the garbage disposal system of the cell). By kick starting the rubbish removal system, the cells were healthier. In addition, treatment with MSDC-0160 resulted in less inflammation – or activation of the immune system – in the brain.
Sounds very interesting. When do clinical trials start?
We’re not sure. They will most likely be in the planning stages though. If MSDC-0160 is approved for diabetes, it will be easier to have it approved for Parkinson’s disease as well.
Other diabetes drugs, however, are currently being tested in clinical trials for Parkinson’s disease. Of particular interest is Exenatide, which is just finishing a placebo-controlled, double blind phase 2 clinical trial. We are expecting the results for that trial early next year. Previous clinical studies suggested very positive results for Exenatide:
Title: Exenatide and the treatment of patients with Parkinson’s disease. Authors: Aviles-Olmos I, Dickson J, Kefalopoulou Z, Djamshidian A, Ell P, Soderlund T, Whitton P, Wyse R, Isaacs T, Lees A, Limousin P, Foltynie T. Journal: J Clin Invest. 2013 Jun;123(6):2730-6. PMID:23728174 (This study is OPEN ACCESS if you would like to read it)
The researchers running this clinical study gave Exenatide to a group of 21 patients with moderate Parkinson’s disease and evaluated their progress over a 14 month period (comparing them to 24 control subjects with Parkinson’s disease). Exenatide was well tolerated by the participants, although there was some weight loss reported amongst many of the subjects (one subject could not complete the study due to weight loss). Importantly, Exenatide-treated patients demonstrated improvements in their clinician assessed PD ratings, while the control patients continued to decline. Interestingly, in a two year follow up study – which was conducted 12 months after the patients stopped receiving Exenatide – the researchers found that patients previously exposed to Exenatide demonstrated a significant improvement (based on a blind assessment) in their motor features when compared to the control subjects involved in the study.
The results of that initial clinical study were intriguing and exciting, but it is important to remember that the study was open-label: the subjects knew that they were receiving the drug. This means that we can not discount the placebo effect causing some of the beneficial effects reported.
And Exenatide is not the only diabetes drug being tested
Pioglitazone is another licensed diabetes drug that is now being tested in Parkinson’s disease. It reduces insulin resistance by increasing the sensitivity of cells to insulin. Pioglitazone has been shown to offer protection in animal models of Parkinson’s disease (click here and here for more on this). And the drug is currently being tested in a clinical trial.
So what does it all mean?
People with diabetes appear to be more vulnerable than the general population to developing Parkinson’s disease, and many people with Parkinson’s disease have glucose processing issues. It would be very interesting to better understand the link between Parkinson’s disease and diabetes. Why is it that so many people with Parkinson’s disease are glucose intolerant? And why do so many people with diabetes go on to develop Parkinson’s? Answering either of these questions might provide further insight into how both conditions function. And given that drugs associated with one appear to help with the other only strengthens the curious association.
As mentioned above, 2017 will bring the results of Exenatide clinical trial, upon which a lot of hope is riding. If it provides positive benefits, then we will finally have a treatment that can slow the progression of the disease. In addition, we will be able to delve more deeply into how Exenatide is causing it’s effect. Positive outcomes for Exenatide will also open the flood gates for many of the other clinically approved diabetes medications which could be trialled on people with Parkinson’s disease.
So despite how you may be feeling about 2017 (based on the events of 2016), we here at the SoPD believe that there is a lot to look forward to in the new year.
Exciting new last week from a small biotech company called Voyager Therapeutics which is using gene therapy to treat neurodegenerative disease. Their primary product (VY-AADC01) is focused on Parkinson’s disease and the initial results look very positive.
The press release has indicates that the treatment is well tolerated and has beneficial effects on the subject’s motor functions. This last part is very interesting as the trial is being conducted on people with advanced Parkinson’s disease.
In today’s post, we’ll review the technology and what the results mean.
In Parkinson’s disease, we often talk about the loss of the dopamine neurons in the midbrain as a cardinal feature of the disease. When people are diagnosed with Parkinson’s disease, they have usually lost approximately 50-60% of the dopamine neurons in an area of the brain called the substantia nigra.
The dark pigmented dopamine neurons in the substantia nigra are reduced in the Parkinson’s disease brain (right). Source: Memorangapp
The midbrain is – as the label suggests – in the middle of the brain, just above the brainstem (see image below). The substantia nigra dopamine neurons reside there.
Location of the substantia nigra in the midbrain. Source: Memorylossonline
The dopamine neurons of the substantia nigra generate dopamine and release that chemical in different areas of the brain. The primary regions of that release are areas of the brain called the putamen and the Caudate nucleus. The dopamine neurons of the substantia nigra have long projections (or axons) that extend a long way across the brain to the putamen and caudate nucleus, so that dopamine can be released there.
The projections of the substantia nigra dopamine neurons. Source: MyBrainNotes
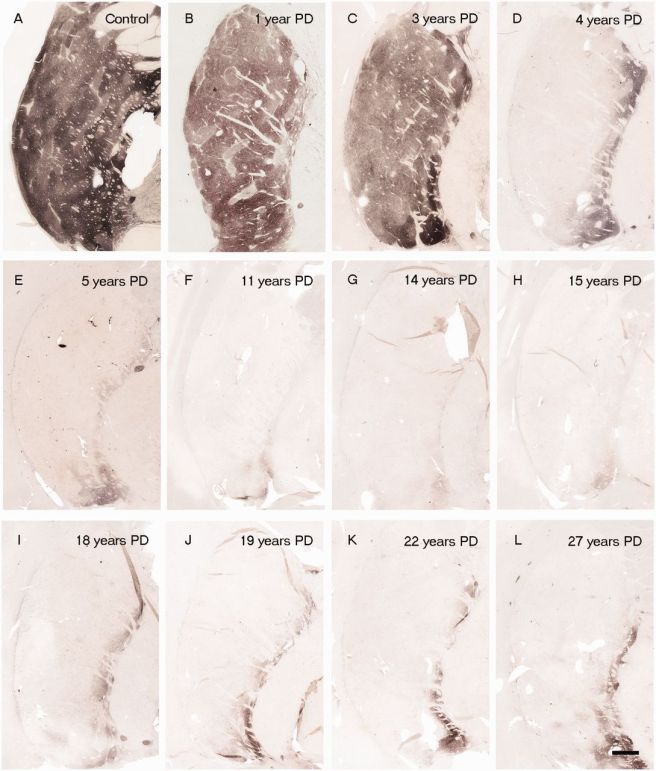
In Parkinson’s disease, these ‘axon’ extensions that project to the putamen and caudate nucleus gradually disappear as the dopamine neurons of the substantia nigra are lost. When one looks at brain sections of the putamen after the axons have been labelled with a dark staining technique, this reduction in axons is very apparent over time, especially when compared to a healthy control brain.
The putamen in Parkinson’s disease (across time). Source: Brain
Previously we have discussed replacing the loss dopamine by transplanting dopamine producing cells into the putamen (click here to read that post), but some researchers now believe that this is not necessary. Instead they have proposed using gene therapy for Parkinson’s disease.
What is gene therapy?
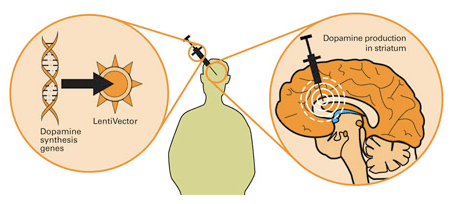
The gene therapy involves inducing cells to produce proteins that they usually do not. This is usually done using genetically modified viruses which have had all the disease causing component removed, allowing us to use the virus as an efficient delivery system. Viruses by their very nature are very good at infecting cells, so if we remove the disease causing components, what is left is a very effective delivery system. Taking this approach one step further, we could next take genes involved with dopamine synthesis and insert them into our empty virus. By then injecting this virus into the brain, we could produce dopamine in any infected cells (it’s slightly more complicated than that, but you get the basic idea).
Gene therapy for Parkinson’s disease. Source: Wiki.Epfl
This approach demonstrated amazing results in preclinical studies in the lab, but the transition to the clinic has not been easy (click here for a good review of the field).
What has been done in the clinic for gene therapy and Parkinson’s disease?
The first clinical attempt at gene therapy for Parkinson’s disease involved injecting a virus containing a gene called glutamic acid decarboxylase (GAD), which is an enzyme involved in the production of a chemical called GABA. The virus was injected into an area of the brain called the subthalamic nucleus, which becomes over-active in Parkinson’s disease. By ectopically producing GAD in the subthalamic nucleus, researchers were able to reduce the level of activity (this is similar to deep brain stimulation in Parkinson’s disease which modulates the activity of the subthalamic nucleus). The clinical trials for GAD produced modest results. The virus was well tolerated, but the clinical effect was limited.
Another clinical trial attempted to cause cells in the putamen to produce a chemical called neurturin (which is very similar to GDNF – we have previously written about GDNF, click here to read that post). The goal of the study was to prove neuroprotection and regeneration to the remaining dopamine neurons, by releasing neurturin in the putamen. Subjects were injected in the putamen with the virus and then the participants were followed for 15 months. Unfortunately,this study failed to demonstrate any meaningful improvement in subjects with Parkinson’s disease.
So what were the results of the trial?
Voyager Therapeutics‘s gene therapy product, VY-AADC01 is an adeno associated virus that carries a gene called Aromatic L-amino acid decarboxylase (or AADC).
AADC is the enzyme that converts L-dopa into dopamine. L-dopa can be naturally produced in the brain from Tyrosine that is absorbed from the blood. It is also the basic component of many treatments for Parkinson’s disease.
By injecting VY-AADC01 into the putamen of people with advanced Parkinson’s disease, Voyager is hoping to alleviate the motor features of the condition by allowing the brain to produce a constant supply of dopamine in the exact location that is missing the dopamine (remember, the putamen is where dopamine is released). This approach will not cure the disease, but it may make life a lot easier for those affected by it.
The phase 1b clinical trial was designed to assess whether the virus had any negative side effects in humans. After the subjects were injected in the brain with VY-AADC01, they were assessed at six and twelve months after the surgery. The results suggest that the virus was well tolerated and resulted in increased AADC enzyme activity, enhanced response to L-dopa treatment, and clinically meaningful improvements in various measures of patients’ motor function (44% improvement in ‘off medication’ measures and 55% improvement in ‘on medication’ measures).
The company currently has 2 groups of subjects injected with the virus (two different concentrations) and they are looking to have a third group injected in early 2017. Phase 2 trials are planned to begin in late 2017.
What does it all mean?
Well, this is a very interesting result and bodes well for other companies taking similar gene therapy approaches (these include Oxford BioMedica and Genepod Therapeutics).
They are also interesting results because the subjects involved in the study all have advanced Parkinson’s disease (the average time since diagnosis in the subject was 10 years). So it is very positive news to see beneficial effects in later stage subjects.
Our ability to delivery of genes to different locations is a symbol of how far we have come with our understanding of biology. The fact that this knowledge is now having a positive impact in the medical world is very exciting. Gene therapy is one treatment approach that we here at SoPD are very excited about and watching very closely.
This week over 40,000 neuroscientists from all over the world have gathered for the annual Society for Neuroscience conference in sunny San Diego. It is 5 days of non-stop presentations of scientific results.
One of the presentations made this year was delivered by Dr Russell Kern, executive vice president and chief scientific officer of International Stem Cell Corp (ISCO). It dealt with the controversial on-going stem cell clinical trial in Australia. In the presentation, Dr Kern outlined the study and gave an update on the first patient in the Phase 1 clinical trial, who was transplanted at the end of July. The second patient is scheduled be treated in the next three weeks. A total of 12 are expected to be treated.
During the three months following the first surgery, the attending physicians observed no signs of complications (which is a very good thing). Unfortunately, according to San Diego Union Tribute, Dr Kern is then said to have implied that ‘there are some indications of efficacy in relieving symptoms of the movement disorder’. In addition, Dr Kern suggested that ‘the patient’s handwriting has improved’.
Long time readers of this blog know that we have been extremely critical of this trial from the start (Click here and here to read them). We make no apologise for this. The pre-clinical data that has been presented thus far in no way justifies taking these particular cells to the clinic. We believe it irresponsible. And our opposition is supported by many other researchers in the Parkinson’s research field (Click here for an example).
It defies belief, however, that Dr Kern would suggest to a conference audience or a media outlet that a patient who is 3 months post surgery could be exhibiting functional improvements. It is widely acknowledged in the Parkinson’s disease research field that it takes 2-3 years for the cells (that are transplanted into the brain) to mature and become functional (click here for more on this). In addition, during their preclinical studies Dr Kern and his colleagues observed very little in the way of behavioural improvements 12 months after transplantation (when compared to control conditions), so how is it that they are seeing such rapid improvements in their first human subject?
If Dr Kern’s suggestions of functional improvements are based solely on the unblinded observations of the clinician and the patient, then sharing such information publicly is extremely inappropriate. Unprofessional at best, but potentially unethical. At the very least, any suggestions of functional recovery in cases like these should be supported by brain scans (indicating increases in dopamine activity) and blinded, unbiased investigator scoring. Otherwise any reported outcomes could simply be due to the placebo effect (as the patient knows that he has been transplanted), and thus not valid for a Parkinson’s community desperate to see positive results in a potential therapy.
We also have concerns regarding the financial feasibility of the current study. Shares in ISCO have fallen from their giddy highs of $2.50 a share back in 2010 to a recent all-time low of just $0.055 (valuing the company at less than $6 million). According to their most recent financial statement, the company is burning $343,000 per month (for the year ended December 31, 2015), and the company ended 2015 with a cash position of just over $530,000. They partly resolved this problem in March of this year by issuing more shares (Source), but one does worry that this kind of activity can not be maintained indefinitely.
Here at the SoPD, we are very keen for cell transplantation to become a viable treatment option for people with Parkinson’s disease in the very near future. But the approach must be rigorously tried and tested, and presented to the highest standards before it can be considered feasible. As we have said before, the standards surrounding this particular trial (demonstrated by inappropriate disclosures of information during an ongoing clinical trial) are lacking.
FULL DISCLOSURE – The author of this blog is associated with research groups conducting the current Transeuro transplantation trials and the proposed G-Force embryonic stem cell trials planned for 2018. He has endeavoured to present an unbiased coverage of the news surrounding this current clinical trial, but when unacceptable statements are being made to media outlets, well, he is human and it is difficult to remain unbiased. He shares the concerns of the Parkinson’s scientific community that the research supporting the current Australian trial is lacking in its thoroughness, and will potentially jeopardise future work in this area.
It is important for all readers of this post to appreciate that cell transplantation for Parkinson’s disease is still experimental. Anyone declaring otherwise (or selling a procedure based on this approach) should not be trusted. While we appreciate the desperate desire of the Parkinson’s community to treat the disease ‘by any means possible’, bad or poor outcomes at the clinical trial stage for this technology could have serious consequences for the individuals receiving the procedure and negative ramifications for all future research in the stem cell transplantation area.
This is one of the first immuno-therapies being tested in Parkinson’s disease, and the results indicate that the treatment was active and well tolerated.
In this post we will review the press release and what it tells us regarding this clinical trial.
When your body is infected by a foreign agent, it begins to produce some things called antibodies. In most cases, these are Y-shaped proteins that binds to the un-wanted invader and act as a beacon for the immune system. It is a very effective system, allowing us to go about our daily business without getting sick on a regular basis. Antibodies allow us to build up immunity, or resistance of an organism to infection or disease.
Scientist have harnessed the power of this natural process, and they have use it to develop methods of helping our bodies fight off disease.
The first approach is called Acquired Immunity (or adaptive immunity), and it is based on the idea that exposure of the immune system to a pathogen (disease/damage causing agent) creates an ‘immunological memory’ within our immune system, and this leads to an enhanced response to subsequent future encounters with that same pathogen.
Scientists have used the idea of acquired immunity to develop what we call vaccines – which are simply small, neutral fragments of specific pathogen that help the immune system to build up immunity (or resistance) before the body is attacked by the disease-causing pathogen itself.
Passive immunisation is simply the sharing of antibodies. And that might sound a bit disturbing, but it is actually a naturally occurring process. For example, a mother’s antibodies are transferred to her baby in the womb via the placenta.
And again, scientists have devised ways of producing passive immunisation artificially. And recently researchers have been using this approach to attack many medical conditions (particularly cancer), in an area of medicine called immunotherapy.
Think of it as simply boosting the immune system by supplementing the supply of antibodies. Scientists can produce high levels of antibodies that specifically target a particular pathogen and then transfer those antibodies to affected people via an intravenous injection.
How is this being used for Parkinson’s disease?
Well, we have previously discussed the idea of a vaccine for Parkinson’s disease (click here to read that post), and we have been closely following the progress of an Austrian company, AffiRis, who are leading the vaccination approach (Click here for that post).
The vaccine approach is targeting the Parkinson’s disease associated protein, Alpha synuclein. It is believed that a bad kind of alpha synuclein is causing the spread of the condition, by being passed from cell to cell. The goal of the vaccine is to capture and remove all of the alpha synuclein being passed between cells and thus (hopefully) halt the progress of – or at least slow down – the disease.
And this week, another company – Prothena – has reported the results of their phase 1 trial for a passive immunity approach to Parkinson’s disease. They have been injecting subjects in the trial with a treatment called PRX002.
(Remember that a phase 1 trial simply tests the safety of a treatment in humans, it is not required to test efficacy of the treatment. Efficacy comes with phases 2 & 3 trials)
What is PRX002?
PRX002 is a monoclonal antibody. The scientists at the biotech company Prothena have artificially produced large amounts of antibodies to alpha synuclein and these have been injected into people with Parkinson’s disease.
Prothena provide a short video explaining this concept (click here to view the video).
So what were the results of the Prothena study?
The study was conducted in collaboration the pharmaceutical company Roche. It was a double-blind (so both the researchers and subjects did not know what they were receiving until the conclusion of the study), placebo-controlled study involving 80 people with Parkinson’s disease. The subjects were randomly assigned to one of six groups, which received either PRX002 or a placebo. There were six doses of PRX002 tested in the study (0.3, 1, 3, 10, 30 or 60 mg/kg).
The study was conducted over six-month, during which patients received three once-a-month injections of either PRX002 or placebo. The subjects were then followed for an observational period of three months.
According to the press release, no serious treatment-related adverse events were reported in PRX002 treated patients. Mild treatment-related adverse events (greater than anything experienced within the placebo group) were noted in 4 of the 12 subjects in the highest dosage group of PRX002, including constipation and diarrhoea.
Importantly, the investigators reported that thePRX002 antibodies were crossing the blood brain barrier and entering the brain. This resulted in a rapid reduction of alpha-synuclein levels (in some cases by up to 97 percent after a single dose!).
The follow-on Phase 2 clinical study is expected to begin in 2017.
What is the difference between the vaccine and the passive immunity approaches?
Basically, it comes down to levels of control. With a vaccination, once you have injected the vaccine and the immune system is activated, there isn’t much you can do to control the response of the body. And that immune memory is going to last a long time. The passive immunity response, on the other hand, requires regular injections of antibodies which can be stopped if adverse effects are noted.
Plus – and forgive me if I sound a little bit cynical here – drug companies prefer a regular treatment approach (which they can charge for each visit) compared to a one-shot cure. It’s simply a better business model.
What happens next?
In both cases – the vaccine and the passive immunity approaches – phase 2 trials are being set up by the respective companies and we will wait to see have affective these treatments are at slowing down Parkinson’s disease.
If they are affective, expect big headlines in the media and plans for adults everywhere to start being vaccinated. If they fail,…. well, we will have to re-address our understanding of the role of alpha synuclein in Parkinson’s disease.
Interesting times lie ahead.
The banner for todays post was sourced from Prothena
It seems everyday we read stories in the media about the benefits of these things called antioxidants. We are repeatedly told that we ‘need more antioxidants in our diet’, because they will help to stave off debilitating conditions like Parkinson’s disease.
Last week, however, a study was published which indicates that this may not be the case.
In todays post we look at antioxidants and their impact on Parkinson’s disease.
Berries are a wonderful source of antioxidants. Source: Steroidal
Antioxidants are one of those subjects that is often discussed, but not well understood. So before we review the study that was published last week, let’s first have a look at what we mean when we talk about antioxidants.
What is an antioxidant?
An antioxidant is simply a molecule that prevents the oxidation of other molecules.
OK, but what does that mean?
Well, the cells in your body are made of molecules. Molecules are combinations atoms of one or more elements joined by chemical bonds. Atoms consist of a nucleus, neutrons, protons and electrons.
Oxidation is the loss of electrons from a molecule, which in turn destabilises the molecule. Think of iron rusting. Rust is the oxidation of iron – in the presence of oxygen and water, iron molecules will lose electrons over time. Given enough time, this results in the complete break down of objects made of iron.
The exact same thing happens in biology. Molecules in your body go through a similar process of oxidation – losing electrons and becoming unstable. This chemical reaction leads to the production of what we call free radicals, which can then go on to damage cells.
What is a free radical?
A free radical is an unstable molecule – unstable because they are missing electrons. They react quickly with other molecules, trying to capture the needed electron to re-gain stability. Free radicals will literally attack the nearest stable molecule, stealing an electron. This leads to the “attacked” molecule becoming a free radical itself, and thus a chain reaction is started. Inside a living cell this can cause terrible damage, ultimately killing the cell.
Antioxidants are thus the good guys in this situation. They are molecules that neutralize free radicals by donating one of their own electrons. The antioxidant don’t become free radicals by donating an electron because by their very nature they are stable with or without that extra electron.
How free radicals and antioxidants work. Source: h2miraclewater
What are good sources of antioxidants?
While human being are pretty poor at producing antioxidants, plants produce LOTS! Thus vegetables and fruits are a fantastic source of antioxidants.
Sources of antioxidants (no. 3 is our favourite). Source: DrAxe
The Oxygen radical absorbance capacity (ORAC) score mentioned in the figure above is a method of measuring the antioxidant capacity of various substances. For comparative sake, a piece of tofu has an ORAC score of approximately 90, a beef steak has an ORAC score of approximately 10, and a ‘Redbull’ energy drink has an ORAC score of 0 (as they all have very few antioxidants – Source:Superfoodly).
A source of major antioxidants are vitamins (such as beta-carotene, vitamin C, and vitamin E). Vitamins are essential nutrients that our bodies needs (in small amounts) to function properly. Many of them are also potent antioxidants.
Vitamin C (or ascorbic acid), in particular, is a powerful antioxidant and it is found in both animals and plants. Unfortunately for humans, however, one of the enzymes needed to make ascorbic acid was lost by a genetic mutation during primate evolution, and so we must obtain it from our diet (eat lots of oranges folks).
How could antioxidants work for Parkinson’s disease?
Postmortem analysis of the brains of people who had Parkinson’s disease has revealed numerous signs of oxidative damage, and this has lead to many researchers hypothesising that oxidation is a key component of the disease.
So what research was published last week?
The results of this study:
Title: Intake of antioxidant vitamins and risk of parkinson’s disease. Authors: Hughes KC, Gao X, Kim IY, Rimm EB, Wang M, Weisskopf MG, Schwarzschild MA, Ascherio A. Journal: Movement Disorders. 2016 Oct 27. doi: 10.1002/mds.26819. PMID:27787934
In this study, the investigators wanted to look at the consumption of antioxidant vitamins and the risk of developing Parkinson’s disease. In order to do this, they needed large pools of medical data that they could analyse. They used the databases from the Nurses’ Health Study (NHS) and the Health Professionals Follow-Up Study (HPFS) in the USA.
NHS study was started in 1976 when 121,700 female registered nurses (aged 30 to 55 years) completed a mailed questionnaire. They provided an overview of their medical histories and health-related behaviours. The HPFS study was established in 1986, when 51,529 male health professionals (40 to 75 years) responded to a similar questionnaire. Both the NHS and the HPFS send out follow-up questionnaires every 2 years.
The investigators in the current study, removed the data from people who reported ‘implausible total energy intake at baseline (<660 or >3,500 kcal/day for women and <800 or >4,200 kcal/day for men)’, missed reporting for any survey, or had a diagnosis of Parkinson’s disease at the start of the study. This left them with the survey results of 80,750 women and 48,672 men to analyse.
From these pools of subjects, they found a total of 1036 people with Parkinson’s disease (554 in HPFS and 482 in NHS). When the investigators looked at antioxidant vitamin consumption, they found that vitamin E was not associated with an increased or decreased risk of Parkinson’s disease. Vitamin C intake showed indications of reducing the risk of developing Parkinson’s, but this not significant.
The investigators concluded that their results do not support the hypothesis that consumption of antioxidant vitamins reduces the risk of Parkinson’s disease.
What about other Parkinson’s disease research on antioxidants?
There have been several clinical trials for antioxidants and Parkinson’s disease. Of particular interest has been the research surrounding Coenzyme Q10 (also known as ubiquinone and ubidecarenone).Coenzyme Q10 is an antioxidant that exhibited positive preclinical results for Parkinson’s disease, and this led to several large clinical trials:
Title: A randomized clinical trial of high-dosage coenzyme Q10 in early Parkinson disease: no evidence of benefit. Authors: Parkinson Study Group QE3 Investigators., Beal MF, et al. Journal: JAMA Neurol. 2014 May;71(5):543-52. PMID:24664227
This article reported the results of a phase III randomized, placebo-controlled, double-blind clinical trial at 67 North American sites, consisting of 600 participants. While Coenzyme Q10 was safe and well tolerated by the subjects in the study, it demonstrated no evidence of clinical benefit.
One justified critique of this study, however, was the variety of subjects with Parkinson’s disease involved in the study. It has been suggested that a clinical trial should be performed with coenzyme Q10 in people with Parkinson’s disease who have a proven mutation in the PINK1 gene as these are the subjects who are most likely to benefit from this approach. That would be an interesting trial.
So what does it all mean?
Well, the study published last week needs to be replicated with another large database before any serious conclusions can be made. For all the hype around antioxidants, however, there is a worrying lack of supporting evidence that they actually have any effect (in the case of lung cancer there are even suggestions that some vitamin antioxidants could exacerbate the situation – click here for more on this).
The results of the study reviewed above do suggest that our view of oxidation in Parkinson’s disease needs to be re-addressed. It may be that oxidation may simply be an end step in the condition, and trying to block it with antioxidants is fruitless.
It should be noted that we are not suggesting here that people should stop taking antioxidants – they are an important part of any balanced diet, necessary for normal biological functioning. We are simply presenting the evidence that some of the hype surrounding their potential is unfounded.
As usual, as more information comes to hand, we shall present it here. Watch this space.
The banner for todays post was sourced from Pinkhope
For more than 50 years, L-dopa (a critical ingredient used by the brain to produce the chemical dopamine) has been one of the primary therapies used in the treatment of Parkinson’s disease. Over those years, there have been several different versions of L-dopa, providing advantages over previous forms. Last week, the results of clinical trials involving a new inhalable version of L-dopa were published.
In this post we will review the results of those studies.
The motor features (a resting tremor in one of the limbs, slowness of movement, and rigidity in the limbs) of Parkinson’s disease begin to appear when most of the dopamine producing neurons in the brain have been lost (specifically, >60% of the midbrain dopamine neurons). Thus for the last 50 years the primary means of treating Parkinson’s disease has been via dopamine replacement therapies.
Why don’t we just inject people with dopamine?
The chemical dopamine has a very difficult time crossing the blood-brain barrier, which is a thick membrane surrounding the brain. This barrier protects the brain from unwanted undesirables (think toxic chemicals), but it also blocks the transfer of some chemicals that exert a positive impact (such as dopamine).
When dopamine is blocked from entering the brain, other enzymes can convert it into another chemical called ‘norepinephrine’ (or epinephrine) and this conversion can cause serious side effects in blood pressure and glucose metabolism.
In addition, any dopamine that does find its way into the brain is very quickly broken down by enzymes. Thus, the amount of time that dopamine has to act is reduced, resulting in a very limited outcome. And these reasons are why doctors turned to L-dopa instead of dopamine in the treatment of Parkinson’s disease.
What is L-dopa?
Basically, Levodopa (L-dopa) is a chemical intermediary in the production of dopamine. That is to say, you need L-dopa to make dopamine. L-dopa is very stable inside the body and crosses the blood-brain-barrier very easily.
In the UK, a commonly used version is known as ‘Sinemet®‘(produced by Merck).
The chemical structure of L-dopa. Source: Wikipedia
The best way to understand what L-dopa is probably be to explain the history of this remarkable chemical.
The history of L-dopa
Until the 1950s there were few treatment options for Parkinson’s disease, but a young scientist in Sweden was about to change that.
In 1957, he discovered that when he injected the brains of rabbits with a neurotoxin (reserpine) it killed the dopamine neurons (and the animals exhibited reduced movement). He also discovered that by injecting the dopamine precursor –L-dopa – into those same animals, he was able to rescue their motor ability. Importantly, he found that the serotonin precursor (called 5-hydroxytryptophan) was not capable of reversing the reduction in motor ability, indicating that the effect was specific to L-dopa.
Here is the 1957 report:
Title: 3,4-Dihydroxyphenylalanine and 5-hydroxytryptophan as reserpine antagonists.
Authors: Carlsson A, Lindqvist M, Magnusson T.
Journal: Nature. 1957 Nov 30;180(4596):1200. No abstract available.
PMID: 13483658 (the article on the Nature website – access required)
At the time, we did not know that dopamine was depleted in Parkinson’s disease. And people with Parkinson’s continued to suffer.
It was not until 1960 that the critical discovery of Parkinson’s disease was made by another young European scientist. Carlsson’s research (and that of others) inspired the Austrian researcher, Oleh Hornykiewicz to look at dopamine levels in people with Parkinson’s disease.
In his study, Hornykiewicz found very high levels of dopamine in the basal ganglia of normal postmortem adult brains, but a marked and consistent reduction (approx. 10-fold) in six postmortem cases of Parkinsonisms. The basal ganglia is one of the main regions of the brain that dopamine neurons communicate with (releasing dopamine there).
Title: Distribution of noradrenaline and dopamine (3-hydroxytyramine) in the human brain and their behavior in diseases of the extrapyramidal system Authors: Ehringer H, Hornykiewicz O. Journal: Parkinsonism Relat Disord. 1998 Aug;4(2):53-7. No abstract available. PMID:18591088
Importantly, Hornykiewicz did not stop there.
In November 1960, Hornykiewicz approached Walther Birkmayer, a doctor at a home for the aged in Vienna, and together they began some clinical trials of L-dopa in July 1961. Birkmayer injected 50 to 150 mg intravenously in saline into 20 volunteers with Parkinsonism. In their report, Birkmayer and Hornykiewicz wrote this regarding the results:
“The effect of a single intravenous injection of l-dopa was, in short, a complete abolition or substantial relief of akinesia. Bedridden patients who were unable to sit up, patients who could not stand up when seated, and patients who when standing could not start walking performed after l-dopa all of these activities with ease. They walked around with normal associated movements, and they could even run and jump. The voiceless, aphonic speech, blurred by palilalia and unclear articulation, became forceful and clear as in a normal person. For short periods of time the people were able to perform motor activities, which could not be prompted to any comparable degree by any other known drug”
Despite their initial excitement, Birkmayer and Hornykiewicz found that the response to L-dopa was very limited in its duration. In addition, subsequent trials by others were not able to achieve similar results, with many failing to see any benefit at all.
And that was when George stepped into the picture.
Dr George Cotzias…and yes, he is holding a brain. Source: New Scientist
Dr George Cotzias was a physician working in New York who became very interested in the use of L-dopa for Parkinson’s disease. And he discovered that by starting with very small doses of L-dopa, given orally every two hours and gradually increasing the dose gradually he was able to stabilize patients on large enough doses to cause a dramatic changes in their symptoms. His studies led ultimately to the Food and Drug Administration (FDA) approving the use of L-dopa for use in PD in 1970. Cotzias and his colleagues were also the first to describe L-dopa–induced dyskinesias.
How does L-dopa work?
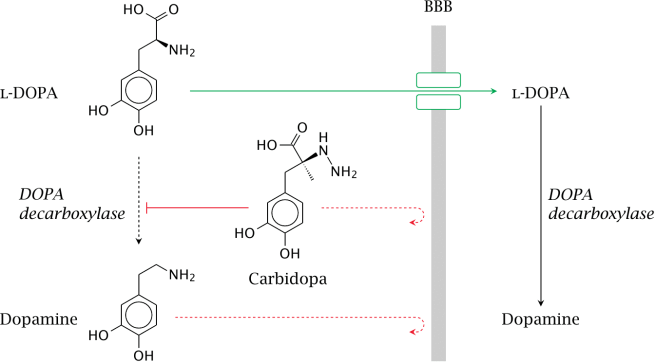
When you take an L-dopa tablet, the chemical will enter your blood. Via your bloodstream, it arrives in the brain where it will be absorbed by cells. Inside the cells, another chemical (called DOPA decarboxylase) then changes it into dopamine. And that dopamine is released, and that helps to alleviate the motor features of Parkinson’s disease.
The production of dopamine, using L-dopa. Source: Watcut
Outside the brain, there is a lot of DOPA decarboxylase in other organs of the body, and if this is not blocked then the effect of L-dopa is reduced in the brain, as less L-dopa reaches the brain. To this end, people with Parkinson’s disease are also given Carbidopa (Lodosyn) which inhibits DOPA decarboxylase outside of the brain (Carbidopa does not cross the blood-brain-barrier).
How does the L-dopa inhaler work?
The company behind this new product, Acorda Therapeutics, spent many years developing a powdered version of levodopa that could be delivered to the lungs. Early on in this developmental process the scientists realised a problem: while normal asthma inhalers only need to release micrograms of their medicine to the lungs, a L-dopa inhaler would need to deliver 1,000 times more than that to have any effect. The huge amounts were needed to ensure that enough L-dopa would get from the lungs into the brain to be effective. Thus, the ARCUS inhaler delivers 25 to 50 milligrams in two breaths.
The inhaler contains capsules of L-dopa, which are designed to break open so that the powder can escape. By sucking on the inhaler (see image below), the open capsule starts spinning, releasing the levodopa into the air and subsequently into the lungs.
Pretty straightforward, right? Nice idea, cool design, easy to use.
But does it work?
What were the results of the clinical trials?
Title: Preclinical and clinical assessment of inhaled levodopa for OFF episodes in Parkinson’s disease. Authors: Lipp MM, Batycky R, Moore J, Leinonen M, Freed MI. Journal: Sci Transl Med. 2016 Oct 12;8(360):360ra136. PMID:27733560 (This article is OPEN ACCESS if you would like to read it)
In their research report, the scientists provided data from three studies: preclinical, phase one clinical, and phase two clinical. In the preclinical work, they measured the levels of L-dopa in dogs who had inhaled levodopa powder. When they looked at blood samples, they found that levodopa levels peaked in all of the animals 2.5 min after administration. This represented a very quick route to the blood system, as dogs that were given levodopa plus carbidopa orally did not exhibit peak blood levodopa levels until 30 min after administration.
In the phase one (safety) clinical trial, 18 healthy persons were enrolled, and again comparisons were made between inhaled CVT-301 and orally administered carbidopa/levodopa. This study demonstrated that CVT-301 was safe and had a similar rapidity of action as in the preclinical dog study.
Next, the researchers conducted a phase two (efficacy) clinical study. This involve 24 people with Parkinson’s disease inhaling CVT-301 as a single 50mg dose during an OFF episode (periods of no prescribed medication). 77% of the CVT-301 treated subjects showed an increase in plasma levodopa within 10 min. By comparison, only 27% of a group of subjects taking oral doses of carbidopa/levodopa at a 25-mg/100-mg dose achieved the same levels within that time. Improvements in timed finger tapping and overall motor function (as measured by the Unified Parkinson’s Disease Rating Scale) were observed between 5 and 15 minutes after administration.
The most common adverse event was cough, but all of the coughing events were considered mild to moderate, generally occurring at the time of inhalation. In most cases, they were resolved rapidly and became less frequent after initial dosing.
So what does it all mean?
Inhalation of L-dopa may represent a novel means of treating people with Parkinson’s disease, especially those who struggle with swallowing pills. The most obvious benefit is the speed with which the subjects see results.
The amount of L-dopa being used is very high, however, and we will be interested to see the results of more long term studies before passing judgement on the inhaler approach. We’ll keep you informed as more information comes to hand.
The banner for today’s post is sourced from the BBC
In today’s post we are going to review the results of a phase 1 trial for new kind of drug being oriented at Parkinson’s disease. The results were announced in late September, and they indicate that the drug was well tolerated by subjects taking part in the study.
Here at the Science of Parkinson’s disease we are always on the look out for novel drug therapies. Many of the treatments currently being tested in the clinic are simply different versions of L-dopa or a dopamine agonist.
So when Prexton Therapeutics recently announced the results of their phase 1 clinical trial for their lead drug, PXT002331, we sat up and took notes. PXT002331 (formerly called DT1687) is the first drug of its kind to be tested in Parkinson’s disease.
It is a mGluR4 positive allosteric modulator.
What on earth is mGluR4 positive allosteric modulator?
The metabotropic glutamate receptors (mGluR) are an abundant family of receptors in the brain. Proteins bind to these receptors and activate (or block) an associated function. There are many different types of these receptors and mGluR4 is simply a small subset. The mGluR4s, however, are present in the areas affected by Parkinson’s disease, and this is why this particular family of receptors has been the focus of much research attention.
But what about the positive allosteric modulator part of ‘mGluR4 positive allosteric modulator’
Yes, good question.
This is the key part of this new approach. Allosteric modulators are a new class of orally available small molecule therapeutic agents. Traditionally, most marketed drugs bind directly to the same part of receptors that the body’s own natural occurring proteins attach to. This means that those drugs are competing with those endogenous proteins, thus limiting the potential effect of the drug.
Allosteric modulators get around this problem by binding different parts of the receptor. And instead of simply turning on or off the receptor, allosteric modulators can either turn up the volume of the signal being sent by the receptor or decrease the signals. This means that when the body’s naturally occurring protein binds in the receptor, allosteric modulators can either amplify the effect or reduce it depending on which type of allosteric modulators is being administered.
There are two different types of allosteric modulators: positive and negative. And as the label suggests, positive allosteric modulators (or PAMs) increase the signal from the receptor while negative allosteric modulators (or NAMs) reduce the signal. Thus, mGluR4 PAMS are amplifying the signal of the mGluR4 receptors.
Why do we want an amplification of a particular signal?
That is a hard question to answer.
Here’s the short explanation:
When you are planning to make a movement with your body, the process of actually initiating that movement begins in the cortex, specifically the primary motor cortex:
A cross section of the human brain illustrating the primary motor cortex. Source: Droso4schools
The primary motor cortex receives information from other regions of the brain (such as the prefrontal cortex where you make a lot of your decisions), and it will then send a signal down into the brain and down the spinal cord telling the limbs to move. On the way down through the brain, the signal will pass through a series of check points that will filter the signal and determine the final strength of it.
A schematic of the feedback loop of check points. Source: Parkinson’s Biology
EDITOR’S NOTE: We have borrowed this image from the Parkinson’s biology blog, which we are huge fans of. We highly recommend people visit that site as well as our lovely site. They also provide easy to understand explanations of the biology of Parkinson’s disease.
These checkpoints represent a large feedback loop. The critical step in this process is the processing being conducted in the basal ganglia, which can be broken down into different subregions:
A schematic of the components of the basal ganglia. Source: Parkinson’s Biology
The globus pallidus (GPi) is the last area of the basal ganglia that the signal will pass through on it’s way to the thalamus (the ultimate decider of whether you will move or not), so if there is anything going wrong between these two structures the initiation of movement will be disrupted.
In a normal brain, the chemical dopamine is being produced in an area called the substantia nigra pars compacta (say that three times really fast). That dopamine is released in the striatum and other areas of the basal ganglia, and it has a mediating effect on the signal passing through these structures.
In Parkinson’s disease, however, the dopamine producing cells of the pars compacta are loss – 60% by the time a person starts to have the clinical motor features appearing. The loss of this dopamine leaves the whole system ‘unmediated’. The feedback loop becomes extremely inhibited, resulting in problems initiating movement.
Deep brain stimulation can un-inhibit the globus pallidus, by mediating the signal passing through that structure. But this requires surgery and the implanting of probes deep inside the brain.
A schematic of deep brain stimulation of the globus pallidus. Source: Parkinson’s Biology (great website!)
A better way of reducing the inhibition in this feedback loop is the replacement of dopamine (which we do via the taking of treatments like L-dopa). This has been the standard approach for more than 50 years.
A new method of reducing the inhibition in the feedback loop would be to chemically targeting the globus pallidus, and this is what scientists are trying to do with the mGluR4 PAMS. By amplifying the signal of mGluR4s in the globus pallidus, the scientists believe that they can reduce the level of inhibition in the feedback loop.
The hope is that this approach is a less Parkinson’s disease-affected treatment. That is to say, the globus pallidus is structurally less affected by Parkinson’s disease than the substantia nigra pars compacta, and thus any treatment of the globus pallidus should be more stable over time (as the disease progresses).
That said, it is acknowledged that mGluR4 PAMS are NOT a potential cure for Parkinson’s disease, but rather a better way of treating the condition.
What research has been done on mGluR4 PAMS and Parkinson’s disease?
In August of 2003, some researchers at the pharmaceutical company Merck published a study which indicated that activation of mGluR4 could decrease the excessive levels of inhibition in the globus pallidus.
Title: Group III metabotropic glutamate receptor-mediated modulation of the striatopallidal synapse. Authors: Valenti O, Marino MJ, Wittmann M, Lis E, DiLella AG, Kinney GG, Conn PJ. Journal: Journal of Neuroscience. 2003 Aug 6;23(18):7218-26. PMID:12904482 (This article is OPEN ACCESS if you would like to read it)
The researchers found that an mGluR4 agonist (a protein that binds to the receptor directly, encouraging the associated action) reduced inhibitory signal being produced in the globus pallidus (through a presynaptic mechanism of action). They next demonstrated that the effect did not happen in mice which do not have mGluR4s, illustrating the specificity of the effect. They finished the study by injecting the mGluR4 agonist into a rodent model of Parkinson’s disease and found beneficial effects – that were equivalent to L-dopa.
Based on this research, the scientists at Merck next turned their attention to modulating the mGluR4s in the globus pallidus using allosteric modulators:
Title: Allosteric modulation of group III metabotropic glutamate receptor 4: a potential approach to Parkinson’s disease treatment. Authors: Marino MJ, Williams DL Jr, O’Brien JA, Valenti O, McDonald TP, Clements MK, Wang R, DiLella AG, Hess JF, Kinney GG, Conn PJ. Journal: Proc Natl Acad Sci U S A. 2003 Nov 11;100(23):13668-73. PMID:14593202 (This article is OPEN ACCESS if you would like to read it)
In this article, the same researchers introduce a positive allosteric modulator called ‘PHCCC’ which has a preference for binding to mGluR4. They found that when they put PHCCC – in combination with the mGluR4 agonist used in the previous study – onto cells in petri dishes, they got an amplification of the reduction in inhibition in the cells. Administered alone, PHCCC also produced a marked reversal of the motor deficit observed in a rodent model of Parkinson’s disease.
With these results, the scientists could begin building the justification for taking mGluR4 PAMs to the clinic. They were interested, however, in what impact mGluR4 PAMs could have on the involuntary motor problems associated with long-term L-dopa use, called dyskinesias (we have previously written about these – click here to read that post). So they decided to investigate whether mGluR4 PAMs may have an impact on dyskinesias:
Title: Pharmacological stimulation of metabotropic glutamate receptor type 4 in a rat model of Parkinson’s disease and L-DOPA-induced dyskinesia: Comparison between a positive allosteric modulator and an orthosteric agonist. Authors: Iderberg H, Maslava N, Thompson AD, Bubser M, Niswender CM, Hopkins CR, Lindsley CW, Conn PJ, Jones CK, Cenci MA. Journal: Neuropharmacology. 2015 Aug;95:121-9. PMID:25749357 (This article is OPEN ACCESS if you would like to read it)
In this study, the investigators compared a mGluR4 PAM with a mGluR4 agonist (similar to that used in the previous studies) in rodent models of L-dopa induced dyskinesias. They found that the neither of the two drugs modified the development of dyskinetic behaviours, nor could they modify the behaviours when given together with L-dopa. In fact, when a low dose of L-dopa was given to the animals (resulting in only mild dyskinesias), the researchers found that by adding mGluR4 PAM the dyskinetic behaviours became more exaggerated. The investigators concluded that stimulation of mGluR4 does not have anti-dyskinetic activity. This is an important characteristic to determine before taking a drug to the clinic for Parkinson’s disease.
So what were the results of the phase 1 clinical trial?
In July of 2012, Merck spun off the research into a new company called Prexton Therapeutics. The company almost immediately started setting up a phase 1 safety clinical trial for its lead compound, the mGluR4 PAM: PXT002331. A total of 64 healthy volunteers were enrolled to evaluate the safety and tolerability of several different doses of orally taken PXT002331. The study was completed on time and demonstrated that PXT002331 is safe and well tolerated (at doses well above those that produce robust effects in Parkinson’s disease animal models).
Very positive news.
The planning of a phase 2 clinical trial in people with Parkinson’s disease is now underway. It will take place in the first half of 2017, and this study will provide the first indications as to whether this new treatment approach will be effective in human at treating the features of Parkinson’s disease. We will keep you posted on the success of that study when the results become available.
Are other biotech companies using this approach?
Yes, PAM-based therapies for Parkinson’s disease are very much in vogue at the moment.
Just this month, the biotech company Asceneuron received a grant from The Michael J. Fox Foundation for Parkinson’s Research for the development of positive allosteric modulators of the M1 muscarinic acetylcholine receptor (M1 PAMs). So we can hopefully expect more from this approach to therapies.
Interesting times. And hopefully positive results to come.
EDITOR’S NOTE: It is important to remember that any clinical trial research discussed on this blog is of an educational nature. Nothing written here can or should be mistaken as medical advice. All of these drugs are still experimental and require extensive testing before being offered to the general population. Please speak with a certified clinician before attempting any change to your current medical treatment regime.
The image used in the banner of today’s post was sourced from MedTechBoston
This is the kind of post that can really get someone in quite a bit of trouble.
Both the legal kind of trouble and the social media type of trouble.
Given the online excitement surrounding a particular video that appeared on the internet last week, however, we thought that it would be useful to have a look at the research that has been done on the medicinal use of Cannabis and Parkinson’s disease.
In addition, we will assess the legal status regarding the medicinal use of Cannabis (in the UK at least).
Cannabis being grown for medicinal use. Source: BusinessWire
This week a video appeared online that caused a bit of interest (and hopefully not too many arrests) in the Parkinson’s community.
Here is the video in question:
The video was posted by Ian Frizell, a 55 year old man with early onset Parkinson’s disease. He has recently had deep brain stimulation (DBS) surgery to help control his tremors and he has also posted a video regarding that DBS surgery which people might find useful (Click here to see this).
In the video, Ian turns off his DBS stimulator and his tremors quickly become apparent. He then ‘self medicates’ with cannabis off camera and begins filming again some 20-30 minutes later to show the difference. The change with regards to his tremor are very clear and quite striking.
Here at the SoPD, we find the video very interesting, but we have two immediate questions:
How is this reduction in tremors working?
Would everyone experience the same effect?
We have previously seen many miraculous treatments online (such as coloured glasses controlling dyskinesias video from a few years ago) which have failed when tested under controlled conditions (the coloured glasses did not elicit any effect in the clinical setting – click here to read more). Some of these amazing results can simply be put down to the notorious placebo effect (we have previously discussed this in relation to Parkinson’s disease – click here to read the post), while others may vary on a person to person basis.
Thus, while we applaud Mr Frizell for sharing his finding with the Parkinson’s community, we are weary that the effect may not be applicable to everyone. For this reason, we have made a review of the scientific literature surrounding Cannabis and Parkinson’s disease.
But first:
What exactly is Cannabis?
Drawings of the Hemp plant, from Franz Eugen Köhler’s ‘Medizinal-Pflantzen’. Source: Wikipedia
Cannabis (also known as marijuana) is a family of flowering plants that can be found in three types: sativa, indica, and ruderalis. Cannabis is widely used as a recreational drug, behind only alcohol, caffeine and tobacco in its usage. It typically consumed as dried flower buds (marijuana), as a resin (hashish), or as various extracts which are collectively known as hashish oil.
While the three varieties of cannabis (sativa, indica, and ruderalis) may look very similar, pharmacologically they have very different properties. Cannabis sativa is often reported to cause a “spacey” or heady feeling, while Cannabis indica causes more of a “body high”. Cannabis ruderalis, by contrast, is less well used due to its low Tetrahydrocannabinol levels.
What is Tetrahydrocannabinol?
Tetrahydrocannabinol (or THC) is one of the principle psychoactive components in Cannabis. It a chemical that is believed to be a plant defensive mechanism against herbivores. THC is a cannabinoid, a type of chemical that attaches to the cannabinoid receptors in the body, and it is this pathway that many scientists are exploring for future neuroprotective therapies for Parkinson’s disease (For a good review on the potential cannabinoid-based therapies for Parkinson’s disease, click here).
A second type of cannabinoid is Cannabidiol (or CBD). CBD is considered to have a wider scope for potential medical applications. This is largely due to clinical reports suggesting reduced side effects compared to THC, in particular a lack of psychoactivity.
So what research has been done regarding Cannabis and Parkinson’s disease?
In 2004, a group of scientists in Prague (Czech Republic) were curious to determine cannabis use in people with Parkinson’s disease, so they conducted a study and published their results:
Title: Survey on cannabis use in Parkinson’s disease: subjective improvement of motor symptoms. Authors: Venderová K, Růzicka E, Vorísek V, Visnovský P. Journal: Mov Disord. 2004 Sep;19(9):1102-6. PMID:15372606
The researchers posted out 630 questionnaires to people with Parkinson’s disease in Prague. In total, 339 (53.8%) completed questionnaires were returned to them. Of these, 85 people reported Cannabis use (25.1% of returned questionnaires). They usually consumed it with meals (43.5%), and most of them were taking it once a day (52.9%).
After consuming cannabis, 39 responders (45.9%) described mild or substantial alleviation of their Parkinson’s symptoms in general, 26 (30.6%) improvement of rest tremor, 38 (44.7%) alleviation of rigidity (bradykinesia), 32 (37.7%) alleviation of muscle rigidity, and 12 (14.1%) improvement of L-dopa-induced dyskinesias.
Importantly, half of the people who consumed cannabis experience no effect on their Parkinson’s disease features, and four responders (4.7%) reported that cannabis actually worsened their symptoms. So while this survey suggested some positive effects of cannabis in the treatment of Parkinson’s disease, it is apparent that the effect is different between people.
Additional surveys have been conducted around the world, with similar results (Click here to read more on this).
Have there been any clinical trials?
Yes, there have.
In the 1990s, there was a very small clinical study of cannabis use as a treatment option for Parkinson’s disease, and this study failed to demonstrate any positive outcome. In the study, none of the 5 people with Parkinson’s disease experienced any effect on their Parkinson’s motor features after a week of smoking cannabis (click here for more on this).
This study was followed up by a larger study:
Title: Cannabis for dyskinesia in Parkinson disease: a randomized double-blind crossover study. Authors: Carroll CB, Bain PG, Teare L, Liu X, Joint C, Wroath C, Parkin SG, Fox P, Wright D, Hobart J, Zajicek JP. Journal: Neurology. 2004 Oct 12;63(7):1245-50. PMID:15477546
In this randomized, double-blind, placebo-controlled study, 19 people with Parkinson’s disease randomly received either oral cannabis extract or a placebo (twice daily) for 4 weeks. They then took no treatment for an intervening 2-week ‘washout’ period, before they were given the opposite treatment for 4 weeks (so if they received the cannabis extract during the first 4 weeks, they would be given the placebo during the second 4 weeks). In all cases, the participants and the researchers were ‘blind’ to (unaware of) which treatment was being given.
The results indicated that cannabis was well tolerated by all of the participants in the study, but that it had no pro- or anti-Parkinsonian actions. The researchers found no evidence for a treatment effect on levodopa-induced dyskinesia.
In addition to this study, there has been a recent double-blind clinical study of cannabidiol (CBD, mentioned above) in the treatment of Parkinson’s disease:
Title: Effects of cannabidiol in the treatment of patients with Parkinson’s disease: an exploratory double-blind trial. Authors: Chagas MH, Zuardi AW, Tumas V, Pena-Pereira MA, Sobreira ET, Bergamaschi MM, dos Santos AC, Teixeira AL, Hallak JE, Crippa JA. Journal: J Psychopharmacol. 2014 Nov;28(11):1088-98. PMID:25237116
The Brazilian researchers who conducted the study took 21 people with Parkinson’s disease and assigned them to one of three groups which were treated with placebo, small dose of CBD (75 mg/day) or high dose of CBD (300 mg/day). They found that there was no positive effects by administering CBD to people with Parkinson’s disease, except in their self-reported measures on ‘quality of life’.
So what does all of this mean?
Firstly, let us be clear that we are not trying to discredit Mr Frizell or suggest that what he is experiencing is not a real effect. The video he has uploaded suggests that he is experiencing very positive benefits by consuming cannabis to help treat his tremors.
Having said that, based on the studies we have reviewed above we (here at the SoPD) have to conclude that the clinical evidence supporting the idea of cannabis as a treatment for Parkinson’s disease is inconclusive. There does appear to be some individuals (like Mr Frizell) who may experience some positive outcomes by consuming the drug, but there are also individuals for whom cannabis has no effect.
One of the reasons that cannabis may not be having an effect on everyone with Parkinson’s disease is that many people with Parkinson’s disease actually have a reduction in the cannabis receptors in the brain (click here for more on this). This reduction is believed to be due to the course of the disease. If there are less receptors for cannabis to bind to, there will be less effect of the drug.
Ok, but how might cannabis be having a positive effect on the guy in the video?
Cannabis is known to cause the release of dopamine in the brain – the chemical classically associated with Parkinson’s disease (Click here and here for more on this). Thus the positive effects that Mr Frizell is experiencing may simply be the result of more dopamine in his brain, similar to taking an L-dopa tablet. Whether enough dopamine is being released to explain the full effect is questionable, but this is still one possible explanation.
There could be questions regarding the long term benefits of Mr Frizell’s cannabis use, as long term users of cannabis generally have reduced levels of dopamine being released in the brain (Click here for more on this). Although the drug initially causes higher levels of dopamine to be released, over time (with long term use) the levels of dopamine in the brain gradually reduce.
I live in the UK. Is it legal for me to try using Cannabis for my Parkinson’s disease?
National status on Cannabis possession for medical purposes. Source: Wikipedia
The map above is incorrect, with regards to the UK at least (and may be incorrect for other regions as well).
According to the Home Office, it is illegal for UK residents to possess cannabis in any form (including medicinal).
Cannabis is illegal to possess, grow, distribute or sell in the UK without the appropriate licences. It is a Class B drug, which carries penalties for unlicensed dealing, unlicensed production and unlicensed trafficking of up to 14 years in prison (Source: Wikipedia; and if you don’t trust Wikipedia, here is the official UK Government website).
In 1999, a major House of Lords inquiry made the recommendation that cannabis should be made available with a doctor’s prescription. The government of the U.K., however, has not accepted the recommendations. Cannabis is not recognised as having any therapeutic value under the law in England and Wales.
Having said all of this, there has recently been an all-party group calls for the legalisation regarding cannabis for medicinal uses to be changed (click here for more on this). Whether this will happen is yet to be seen.
So the answer is “No, you are not allowed to use cannabis to treat your Parkinson’s disease”.
Except…
(And here is where things get a really grey)
There is a cannabis-based product – Sativex – which can be legally prescribed and supplied under special circumstances. Sativex is a mouth spray developed and manufactured by GW Pharmaceuticals in the UK. It is derived from two strains of cannabis leaf and flower, cultivated for their controlled proportions of the active compounds
THC and CBD.
In 2006, the Home Office licensed Sativex so that:
Doctors could privately prescribe it (at their own risk)
Pharmacists could possess and dispense it
Named patients with a prescription could possess
In June 2010 the Medicines Healthcare Regulatory products Agency (MHRA) authorised Sativex as an extra treatment for patients with spasticity due to Multiple Sclerosis (MS). Importantly, doctors can also prescribe it for other things outside of the authorisation, but (again) this is at their own risk.
EDITORIAL NOTE: Given that possessing cannabis is illegal and that more research into the medicinal benefits of cannabis for Parkinson’s disease is required, we here are the SoPD can not endorse the use of cannabis for treating Parkinson’s disease.
While we are deeply sympathetic to the needs of many individuals within the Parkinson’s community and agree with a reconsideration of the laws surrounding the medicinal use of cannabis, we are also aware of the negative consequences of cannabis use (which can differ from person to person).
If a person with Parkinson’s disease is considering a change in their treatment regime for any reason, we must insist that they first discuss the matter with their trained medical physician before undertaking any changes.
The information provided here is strictly for educational purposes only.
The banner for today’s post was sourced from the IBTimes.