According to our friends at Wikipedia:
A placebo (/pləˈsiboʊ/ plə-see-boh; Latin placēbō, “I shall please” from placeō, “I please”) is a simulated or otherwise medically ineffectual treatment for a disease or other medical condition intended to deceive the recipient. Sometimes patients given a placebo treatment will have a perceived or actual improvement in a medical condition, a phenomenon commonly called the placebo effect or placebo response.

In our previous post we wrote about cell transplantation and we cited the two double-blind clinical studies that found little positive effect resulting from the procedure.
In both of those studies, half the participants were given a sham surgery – that is, they were put into the surgery room, anesthetized, an incision was made in their scalps, but nothing was injected into their brains. They (and their assessing investigators) were not told if they were in the transplant group or the sham/control group and they were left in this ‘blind’ state for 12-18 months.
Time is a funny thing.
After a couple of weeks of wondering which group they were in and self assessing their abilities since the surgery, some of the individuals in those studies may have started to think that you are in one group or the other. This is a very human thing to do.
The effect is VERY strong. And it can mess with a clinical study in terrible ways.
In one of the double-blind clinical studies discussed in the last post (Freed et at, 2001), one of the patients had described herself as ‘not being physically active for several years’ before her surgery. Shortly after her surgery, she found that she was able to hike and ice skate again. A miraculous change in situations.
Twelve months after the surgery, however, she found out that she’d had been in the sham/control surgery group. Nothing had been injected into her brain. She had received NO treatment.
Her response was solely due to the placebo effect.
The Placebo effect in Parkinson’s disease
Early last year there was an interesting study conducted that looked at the placebo effect and Parkinson’s disease.

Title: Placebo effect of medication cost in Parkinson disease: a randomized double-blind study.
Author: Espay AJ, Norris MM, Eliassen JC, Dwivedi A, Smith MS, Banks C, Allendorfer JB, Lang AE, Fleck DE, Linke MJ, Szaflarski JP.
Journal: Neurology. 2015 Feb 24;84(8):794-802.
PMID: 25632091
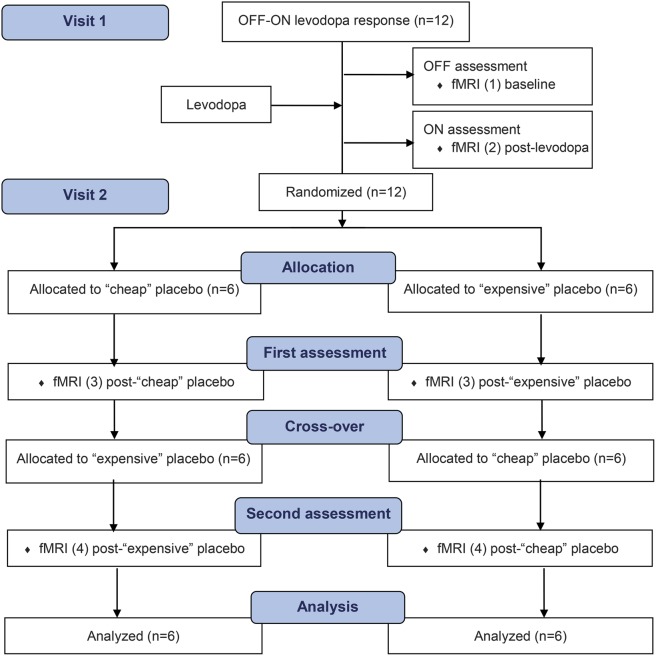
The investigators conducted a double-blind study involving 12 patients with moderate-severe Parkinson disease (average age of the subjects was 62.4 ± 7.9 years; and their average time since diagnosis was 11 ± 6 years). The study involved two visits to the clinic – the first visit involved a clinical assessment while the subjects were both ‘off’ and ‘on’ their standard medication. The assessment also involved a brain scan (fMRI). This was done to determine the magnitude of the dopaminergic benefit of their standard medication.
During the second visit, the subjects were told that they would be given two formulations – a “cheap” and “expensive” – of a “novel injectable dopamine agonist”. Both of these solutions were simply the same saline (medical salt water) solution. Four hours after being give the first injection, the subjects were given the other solution. In this manner, the subjects were exposed to both the ‘cheap’ and ‘expensive’ solutions. During visit 2, the subjects were clinically assessed and brain scanned 3 times, once before the first solution was injected, once after the first solution, and once after the second solution was given.
Below is a flowchart illustrating the structure study:
Source: Neurology
The results were interesting:
- Both of the placebos improved motor function when compared with the baseline (no medication state)
- The expensive placebo had more effect than the cheap placebo (remember: they were the same solution!)
- The benefits were greater when patients were randomized first to expensive placebo followed by the cheap.
- There was a significant difference in the level of improvement between the cheap and expensive placebos (UPDRS-III), with the expensive placebo giving better benefits
- Brain imaging demonstrated that activation was greater when the cheap placebo was given first.
The authors concluded that the “expensive placebo significantly improved motor function and decreased brain activation in a direction and magnitude comparable to, albeit less than, levodopa. Perceptions of cost are capable of altering the placebo response in clinical studies“.
The authors also wrote a summary of the debriefing that followed the study, where the subjects were informed about the true nature of the study. They told the subjects that rather than being injected with a novel dopamine agonist, they were simply given a saline solution – the same solution for both ‘cheap’ and ‘expensive’. They reported that “responses ranged from disbelief to amazement regarding changes experienced“. It must have been rather bewildering to have been told that the positive benefits you experienced were ‘all in your head’ and not based on any pharmacological effect.
While extremely unethical, we here at the SoPD can’t help but wonder about long this placebo effect could last. Would the difference between the cheap and expensive solutions still exist in 12 months time if the subjects were left blinded and continued to take them?
So how might this work?
We know that the placebo effect in Parkinson’s disease is controlled by the release of dopamine – one of the chemicals in the brain that is affected by Parkinson’s disease. Importantly, we know that it the endogenous dopamine that is causing the effect – that is the dopamine our brains are producing naturally as opposed to the L-dopa treatment.
The dopamine that helps to control our motor movements is also involved with positive anticipation, motivation, and response to novelty. Thus when the placebo solution was given to subjects in this study, they believed that they were receiving an active drug and demonstrated an “expectation of reward” response. And the more expensive solution simply heightened the expectation and positive anticipation, therefore increasing the amount of dopamine produced/released.
Given that dopamine is involved with both the features of Parkinson’s disease AND with the mechanisms of anticipation/expectation, you can begin to understand why the placebo effect is such an enormous problem for clinicians undertaking clinical trials.
It would be nice, however, to have a better understanding of the placebo effect and try to harness its positive benefits while also treating Parkinson’s with diseasing slowing/halting therapies.

“In one of the double-blind clinical studies discussed in the last post (Freed et at, 2001), one of the patients had described herself as ‘not being physically active for several years’ before her surgery. Shortly after her surgery, she found that she was able to hike and ice skate again. A miraculous change in situations.
Twelve months after the surgery, however, she found out that she’d had been in the sham/control surgery group. Nothing had been injected into her brain. She had received NO treatment.
Her response was solely due to the placebo effect.”
WOW!
LikeLike
Maybe these would work too? As an adjunct to whatever else Dr recommends or that seems to help
Increase Dopamine with a Healthy Lifestyle (from a website I am not sure about but it does have footnotes)
-Boost Dopamine with Exercise
-Sunlight can increase the number of dopamine receptors and create vitamin D which activates the genes that release dopamine. (42, 43)
-Increase Dopamine with Meditation
-Creative hobbies of all kinds, including knitting, quilting, sewing, drawing, photography, woodworking, and home repair, bring the brain into a meditative state.
-Music Gets Dopamine Flowing
-Boost Dopamine with Touch
-The Role of Dopamine and Sleep-Research suggests that lack of sleep may reduce the number of dopamine receptors. (54)
-Blast Dopamine with a Cold Shower-Taking a shower with 14C°/57F° water can increase dopamine substantially — up to 250%! (58)
I will go look for any SOPD posts about these
LikeLike