Our apologies to anyone who is squeamish about needles, but this is generally how most people get their seasonal flu vaccination.
Why are we talking about flu vaccines?
Because new research, published last week, suggests everyone should be going out and getting them in the hope of reducing our risk of Parkinson’s disease.
In today’s post we will review the research, exactly what a flu vaccine is, and how it relates to Parkinson’s disease.

Electron micro photograph of Influenza viruses. Source: Neuro-hemin
Long time readers of the SoPD blog will know that I have a particular fascination with theories regarding a viral or microbial role in the development of Parkinson’s disease (the ‘idiopathic’ – or arising spontaneously – variety at least).
Why?
Numerous reasons. For example:
- The targeted nature of the condition (why are only selective groups of cells are lost in the brain during the early stages of the condition?)
- The unexplained protein aggregation (eg. Lewy bodies; could they be a cellular defensive mechanism against viruses/microbes – Click here to read more on this idea)
- The asymmetry of the onset (why do tremors start on only one side of the body in most cases?)
And we have previously discussed research here on the website regarding possible associations between Parkinson’s disease and and various types of viruses (including Hepatitis C, Herpes Simplex, and Influenza).
Today we re-visit influenza as new research has been published on this topic.
What is influenza?
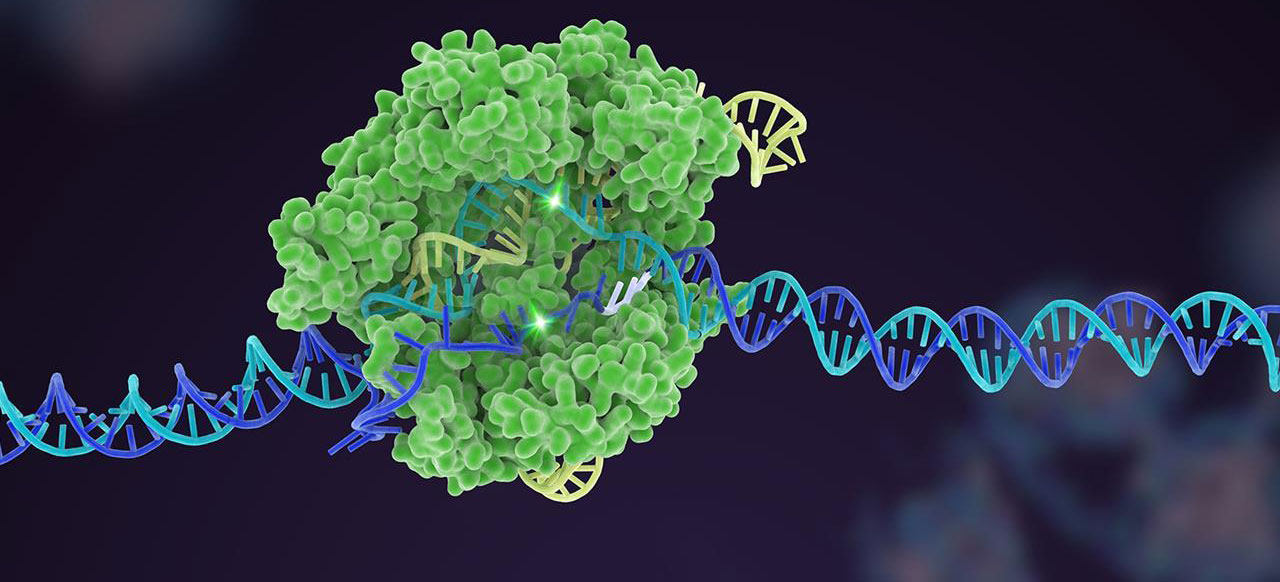
Influenza is a single-stranded, RNA virus of the orthomyxovirus family of viruses.

A schematic of the influenza virus. Source: CDC
It is the virus that causes ‘the flu’ – (runny nose, sore throat, coughing, and fatigue) – with the symptom arising two days after exposure and lasting for about a week. In humans, there are three types of influenza viruses, called Type A, Type B, and Type C. Type A are the most virulent in humans. The influenza virus behind both of the outbreaks in the 1918 pandemic was a Type A.

Schematic of Influenza virus. Source: Bcm
As the image above indicates, the influenza virus has a rounded shape, with “HA” (hemagglutinin) and “NA” (neuraminidases) proteins on the outer surface of the virus. The HA protein allows the virus to stick to the outer membrane of a cell. The virus can then infect the host cell and start the process of reproduction – making more copies of itself. The NA protein is required for the virus to exit the host cell and go on to infect other cells. Different influenza viruses have different combinations of hemagglutinin and neuraminidase proteins, hence the numbering. For example, the Type A virus that caused the outbreaks in the 1918 pandemic was called H1N1.
Inside the influenza virus, there are there are eight pieces (segments) of RNA, hence the fact that influenza is an RNA virus. Some viruses have DNA while others have RNA. The 8 segments of RNA provide the information that is required for making new copies of the virus. Each of these segments provides the instructions for making one or more proteins of the virus (eg. segment 4 contains the instructions to make the HA protein).

The 8 segments of RNA in influenza. Source: URMC
The Influenza virus is one of the most changeable viruses we are aware of, which makes it such a tricky beast to deal with. Influenza uses two techniques to change over time. They are called shift and drift.
Shifting is an sudden change in the virus, which produces a completely new combination of the HA and NA proteins. Virus shift can take place when a person or animal is infected with two different subtypes of influenza. When new viral particles are generated inside the cell, there is a mix of both subtypes of virus which gives rise to an all new type of virus.

An example of viral shift. Source: Bcm
Drifting is the process of random genetic mutation. Gradual, continuous, spontaneous changes that occur when the virus makes small “mistakes” during the replication of its RNA. These mistakes can results in a slight difference in the HA or NA proteins, and although those changes are small, they can be significant enough that the human immune system will no longer recognise and attack the virus. This is why you can repeatedly get the flu and why flu vaccines must be administered each year to combat new forms of circulating influenza virus.
What is a flu jab exactly?
Seasonal flu vaccination is a treatment that is given each year to minimise the risk of being infected by an influenza virus.
The ‘seasonal’ part of the label refers to the fact that the flu vaccine changes each year. Most flu vaccines target three strains of the viruses (and are thus called ‘Trivalent flu vaccines’) which are selected each year based on data collected by various health organisations around the world.
The three chosen viruses for a particular year are traditionally injected into and grown in hens’ eggs, then harvested and purified before the viral particles are chemically deactivated. The three dead viruses are then pooled together and packaged as a vaccine. As you can see in the image below, the process of vaccine production is laborious and takes a full year:

The process of vaccine production. Source: Linkedin
By injecting people with the dead viruses from three different strains of the influenza virus, however, the immune system has the chance to build up a defence against those viruses without the risk of the individual becoming infected (the dead viruses in the vaccine can not infect cells).
Flu vaccines cause the immune system to produce antibodies which are used by the immune system to help defend the body against future attacks from viruses. These antibodies generally take about two weeks to develop in the body after vaccination.
As we have said most injected flu vaccines protect against three types of flu virus. Generally each of the three viruses is taken from the following strains:
- Influenza A (H1N1) – the strain of flu that caused the swine flu pandemic in 2009.
- Influenza A (H3N2) – a strain of flu that mainly affects the elderly and people at risk with long term health conditions. In 2016/17 the vaccine contains an A/Hong Kong/4801/2014 H3N2-like virus.
- Influenza B – a strain of flu that particularly affects children. In 2016/17 the vaccine contains B/Brisbane/60/2008-like virus.
How effective are the vaccines?
Well, it really depends on which strains of influenza are going to affect the most people each year, and this can vary greatly. Overall, however, research from the Centers for Disease Control and Prevention (or CDC) suggests that the seasonal flu vaccine reduces the chance of getting sick by approximately 50% (Source). Not bad when you think about it.
Ok, so are there actually any connections between influenza and Parkinson’s disease?
This question is up for debate.
There are certainly some tentative associations between influenza and Parkinson’s disease. Early on, those connections were coincidental, but more recently research is suggesting that there could be a closer relationship.
Coincidental?
Between January 1918 and December 1920 there were two outbreaks of an influenza virus during an event that became known as the 1918 flu pandemic. Approximately 500 million people across the globe were infected by the H1N1 influenza virus, and this resulted in 50 to 100 million deaths (basically 3-5% of the world’s population). Given that is occurred during World War 1, censors limited the media coverage of the pandemic in many countries in order to maintain morale. The Spanish media were not censored, however, and this is why the 1918 pandemic is often referred to as the ‘Spanish flu’.

1918 Spanish flu. Source: Chronicle
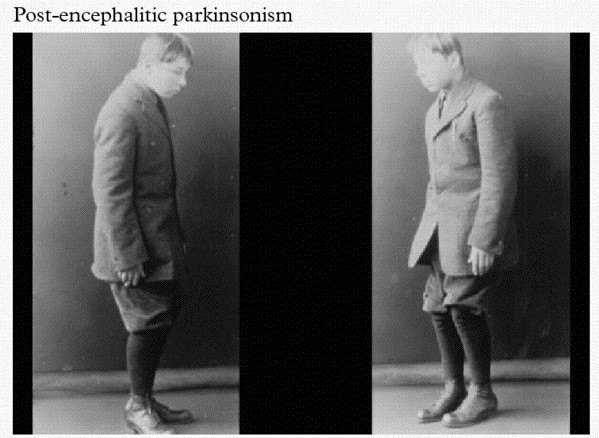
At the same time that H1N1 was causing havoc, a Romanian born neurologist named Constantin von Economo reported a number of unusual symptoms which were referred to as encephalitis lethargica (EL). This disease left victims in a statue-like condition, speechless and motionless.

Constantin von Economo. Source: Wikipedia
By 1926, EL had spread around the world, with nearly five million people being affected. Many of those who survived never returned to their pre-existing state of health. They were left frozen in an immobile state.
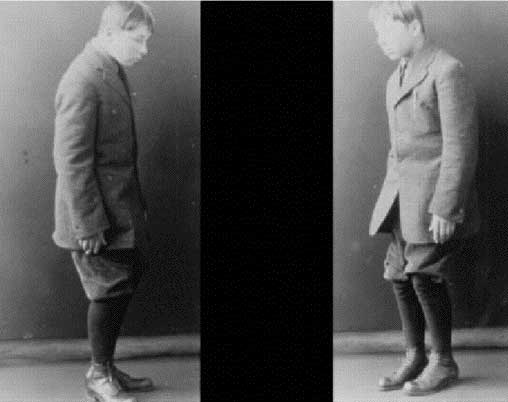
An individual with encephalitis lethargica. Source: Baillement
Historically, it was believed that EL was caused by the influenza virus from the 1918 Spanish influenza pandemic. This was largely due to a temporal association (things happening at approximately the same time) and the finding of influenza antigens in some of the suffers of EL (Click here to read more about this).
And then there were also the observations of Dr Oliver Sacks:

Amazing guy! Dr Oliver Sacks. Source: Pensologosou
During the late 1960s, while employed as a neurologist at Beth Abraham Hospital’s chronic-care facility in New York, Dr Sacks began working with a group of survivors of EL, who had been left immobile by the condition. He treated these individuals with L-dopa (the standard treatment for Parkinson’s disease now, but it was still experimental at the time) and he observed them become miraculously reanimated. The sufferers went from being completely motionless to suddenly active and mobile. Unfortunately the beneficial effects were very short lived.
You may be familiar with Dr Sack’s book about his experience of treating these patients. It is called ‘Awakenings’ and it was turned into a film starring actors Robin Williams and Robert De Niro.

Robin Williams and Robert De Niro in Awakenings. Source: Pinterest
More recent, postmortem analysis of the brains of EL patients found an absence of influenza RNA – click here for more on this), which has led many researchers to simply reject the association between influenza and EL. The evidence supporting this rejection, however, has also been questioned (click here to read more on this), leaving the question of an association between influenza and EL still open for debate.
I think it’s fair to say that we genuinely do not know what caused EL. Whether it was influenza or not is still be undecided.
Ok, so that was the coincidental evidence. Has there been a more direct connection between influenza and Parkinson’s disease?
This is Dr Richard J Smeyne:

Source: Researchgate
Nice guy.
He is a research faculty member in the Department of Developmental Neurobiology at St. Jude Children’s Research Hospital (Memphis, Tennessee).
He has had a strong interest in what role viruses like influenza could be playing in the development of Parkinson’s disease, and his research group has published several interesting research reports on this topic, including:

Title: Highly pathogenic H5N1 influenza virus can enter the central nervous system and induce neuroinflammation and neurodegeneration.
Author: Jang H, Boltz D, Sturm-Ramirez K, Shepherd KR, Jiao Y, Webster R, Smeyne RJ.
Journal: Proc Natl Acad Sci U S A. 2009 Aug 18;106(33):14063-8.
PMID: 19667183 (This article is OPEN ACCESS if you would like to read it)
Dr Smeyne and his colleagues found in this study that when they injected the highly infectious A/Vietnam/1203/04 (H5N1) influenza virus into mice, the virus progressed from the periphery (outside the brain) into the brain itself, where it induced Parkinson’s disease-like symptoms.
The virus also caused a significant increase in the accumulation of the Parkinson’s disease-associated protein Alpha Synuclein. In addition, they witnessed the loss of dopamine neurons in the midbrain of the mice at 60 days after the infection – that cell loss resembling what is observed in the brains of people with Parkinson’s disease.
Naturally this got the researchers rather excited!
In a follow up study on H5N1, however, these same researchers found that the Parkinson’s disease-like symptoms that they observed were actually only temporary:

Title: Inflammatory effects of highly pathogenic H5N1 influenza virus infection in the CNS of mice.
Authors: Jang H, Boltz D, McClaren J, Pani AK, Smeyne M, Korff A, Webster R, Smeyne RJ.
Journal: Journal for Neuroscience, 2012 Feb 1;32(5):1545-59.
PMID: 22302798 (This article is OPEN ACCESS if you would like to read it)
Dr Smeyne and colleagues repeated the 2009 study and had a closer look at what was happening to the dopamine neurons that were disappearing at 60 days post infection with the virus. When they looked at mice at 90 days post infection, they found that the number of dopamine neurons had returned to their normal number. This pattern was also observed in a region of the brain called the striatum, where the dopamine neurons release their dopamine. The levels of dopamine dropped soon after infection, but rose back to normal by 90 days post infection.
How does that work?
The results suggest that rather than developing new dopamine neurons in some kind of miraculous regenerative process, the dopamine neurons that were infected by the virus simply stopped producing dopamine while they dealt with the viral infection. Once the crisis was over, the dopamine neurons went back to life as normal. And because the researcher use chemicals in the production of dopamine to identify the dopamine neurons, they mistakenly thought that the cells had died when they couldn’t see those chemicals.
One interesting observation from the study was that H5N1 infection in mice induced a long-lasting inflammatory response in brain. The resident helper cells, called microglia, became activated by the infection, but remained active long after the dopamine neurons returned to normal service. The investigators speculated as to whether this activation may be a contributing factor in the development of neurodegenerative disorders.
And this is an interesting idea.
In a follow up study, they investigated this further by looking another influenza viruse that doesn’t actually infect cells in the brain:

Title: Induction of microglia activation after infection with the non-neurotropic A/CA/04/2009 H1N1 influenza virus.
Author: Sadasivan S, Zanin M, O’Brien K, Schultz-Cherry S, Smeyne RJ.
Journal: PLoS One. 2015 Apr 10;10(4):e0124047.
PMID: 25861024 (This article is OPEN ACCESS if you would like to read it)
In this study, a different type of influenza (H1N1) was tested, and while it did not infect the brain, it did cause the microglia cells to flare up and become activated. And again, this activation was sustained for a long period after the infection (at least 90 days).
This is a really interesting finding and relates to the idea of a “double hit” theory of Parkinson’s disease, in which the virus doesn’t necessarily cause Parkinson’s disease but may play a supplemental or distractionary role, grabbing the attention of the immune system while some other toxic agent is also attacking the body. Or perhaps simply weakening the immune system by forcing it to fight on multiple fronts. Alone the two would not cause as much damage, but in combination they could deal a terrible blow.
So what was the flu vaccine research published last week?
Again, from Dr Smeyne’s research group, this report looked whether the combination of an influenza virus infection plus a toxic agent gave a worse outcome than just the toxic agent by itself. An interesting idea for a study, but then the investigators threw in another component: what effect would a influenza vaccine have in such an experiment. And the results are interesting:

Title: Synergistic effects of influenza and 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) can be eliminated by the use of influenza therapeutics: experimental evidence for the multi-hit hypothesis
Authors: Sadasivan S, Sharp B, Schultz-Cherry S, & Smeyne RJ
Journal: npj Parkinson’s Disease 3, 18
PMID: N/A (This article is OPEN ACCESS if you would like to read it)
What the researchers found was that H1N1-infected mice that were treated with a neurotoxin (called MPTP – a toxin that specifically kills dopamine neurons) exhibit a 20% greater loss of dopamine neurons than mice that were treated with MPTP alone.
And this increase in dopamine neuron loss was completely eliminated by giving the mice the influenza vaccination. The researchers concluded that the results demonstrate that multiple insults (such as a viral infection and a toxin) can enhance the impact, and may even be significant in allowing an individual to cross a particular threshold for developing a disease.
It’s an intriguing idea.
Have epidemiologists (population data researchers) ever investigated a connection between Parkinson’s disease and influenza?
Good question.
And yes they have:
Title: Parkinson’s disease or Parkinson symptoms following seasonal influenza.
Authors: Toovey S, Jick SS, Meier CR.
Journal: Influenza Other Respir Viruses. 2011 Sep;5(5):328-33.
PMID: 21668692 (This article is OPEN ACCESS if you would like to read it)
In this first study, the researcher used the UK‐based General Practice Research Database to perform a case–control analysis (that means they compare an affected population with an unaffected ‘control’ population. They identified individual cases who had developed an ‘incident diagnosis’ of Parkinson’s disease or Parkinson’s like symptoms between 1994 and March 2007. For each of those case files identified, they matched them with at least four age matched control case files for comparative sake.
Their analysis found that the risk of developing Parkinson’s disease was not associated with previous influenza infections. BUT, they did find that Influenza was associated with Parkinson’s‐like symptoms such as tremor, particularly in the month after an infection. One can’t help but wonder if the dopamine neurons stopped producing dopamine during that period while they dealt with the viral infection.
But of course, I’m only speculating here… and it’s not like there was a second study suggesting that there is actually an association between Parkinson’s disease and influenza.
A year after that first study, a second study was published:

Journal: Association of Parkinson’s disease with infections and occupational exposure to possible vectors.
Authors: Harris MA, Tsui JK, Marion SA, Shen H, Teschke K.
Journal: Movement Disorder. 2012 Aug;27(9):1111-7.
PMID: 22753266
This second study reported that there is actually an association between Parkinson’s disease and influenza.
This investigation was also a case-control study, but it was based in British Columbia, Canada. The researchers recruited 403 individuals detected by their use of antiparkinsonian medications and matched them with 405 control subjects selected from the universal health insurance plan. Severe influenza was associated with Parkinson’s disease at an odds ratio of 2.01 (1 being no difference) and the range of the odds was 1.16-3.48. That’s pretty significant.
Interestingly, the effect is reduced when the reports of infection were restricted to those occurring within 10 years before diagnosis. This observation would suggest that early life infections may have more impact than previously thought.
Curiously, the researchers also found that exposure to certain animals (cats odds ration of 2.06; range 1.09-3.92) and cattle (2.23; range 1.22-4.09) was also associated with developing Parkinson’s disease.
Time to get rid of the pet cow.

Source: RSPB
Do any other neurodegenerative condition have associations with influenza?
In the limited literature search that we conducted, we only found reports dealing with influenza and Alzheimer’s disease.
Large studies suggest that Alzheimer’s is not associated with influenza (click here to read more on this). Interestingly, the Alzheimer’s associated protein beta amyloid has been shown to inhibit influenza A viruses (Click here to read that report), which may partly explain the lack of any association.
Influenza does have a mild association, however, with depression (Click here to see that report).
So what does it all mean?
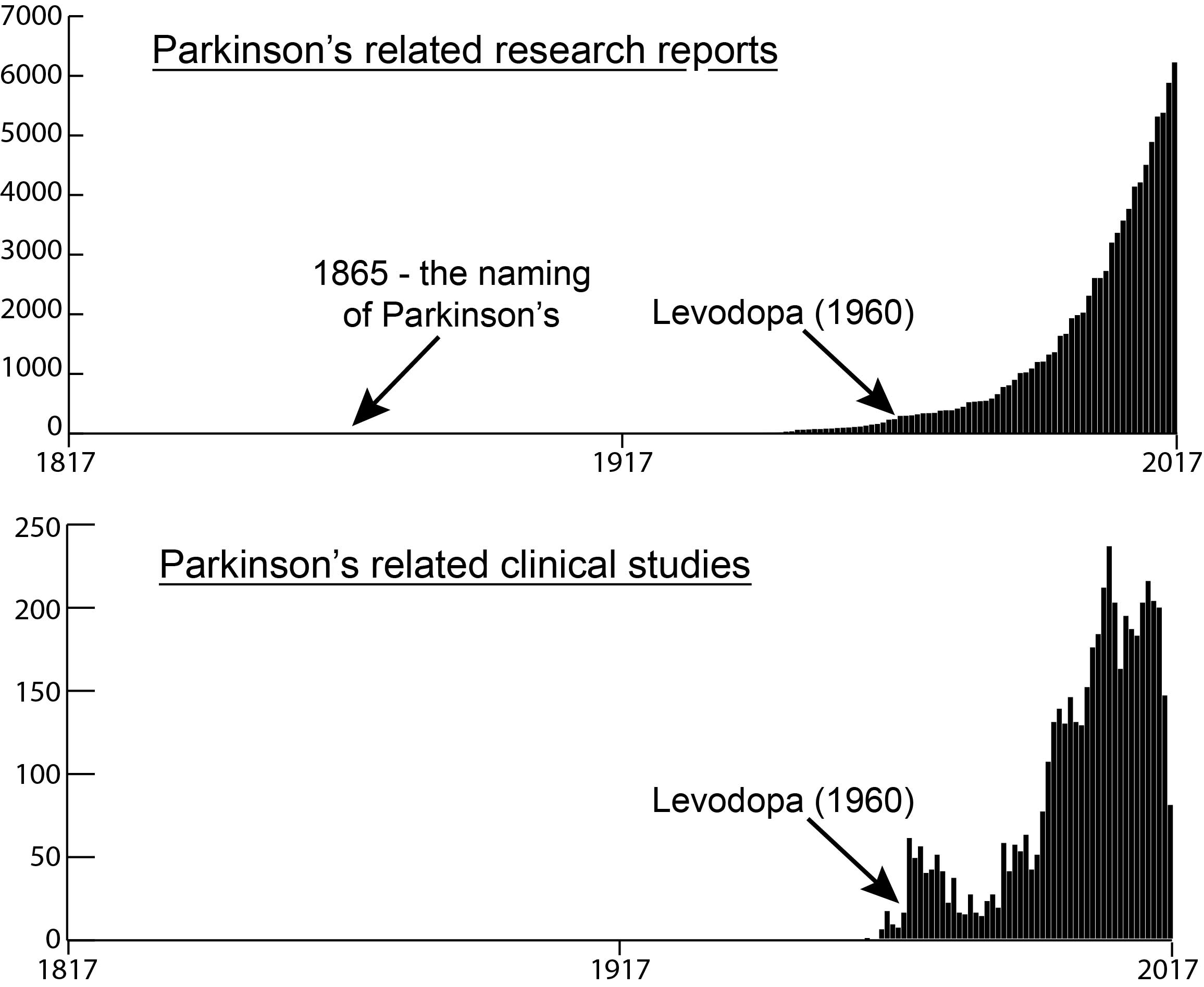
A viral theory for Parkinson’s disease has existed since the great epidemic of 1918. Recent evidence points towards several viruses potentially having some involvement in the development of this neurodegenerative condition. And recent evidence suggests that influenza in particular could be particularly influential.
In 1938, Jonas Salk and Thomas Francis developed the first vaccine against flu viruses. It could be interesting for epidemiologists to go back and see if regular flu vaccination usage (if such data exists) reduces the risk of developing Parkinson’s disease.
But until such data is published, however, perhaps it would be wise to go and get a flu vaccine shot.
The banner for today’s post was sourced from the HuntingtonPost