
|
In March of 2017, activists all over the world celebrated the 30th anniversary of ACT UP. ACT UP was an international direct action advocacy group that was set up to help people with Human immunodeficiency virus (HIV) infections and acquired immune deficiency syndrome (AIDS), and more importantly to encourage legislation/policy, medical research and treatment for this devastating. Some people might say that there have been few advocacy efforts for a medical condition that have had as much impact, or had such a lasting legacy. Others, on the other hand, would suggest that a collective AIDS advocacy effort and a paralysing fear of the deadly condition at the time stimulated most of the action action that followed. Regardless of which opinion is correct, an analysis of the AIDS advocacy makes interesting food for thought. In today’s post, we will have look at what ACT UP did, what was the result of the overall AIDS advocacy movement, and we will discuss what the Parkinson’s (and neurodegenerative) community could learn from it.
|

Every week, the U.S. Centers for Disease Control and Prevention (CDC) publishes the Morbidity and Mortality Weekly Report (or MMWR).
It provides public health information and recommendations based on information collected by the CDC from all of the various state health departments. The material published in each report is provided as a public service and may be reprinted and used without permission.
On the 5th June 1981, the CDC published a MMWR, describing five cases of a rare lung infection (called Pneumocystis carinii pneumonia). This was an extremely rare, but opportunistic infection – it generally occurred in people with very compromised immune systems.
All of the five cases were young (29-36 years of age), and had previously been healthy, homosexual men living in the Los Angeles area. All of the men had additional unusual infections, which suggested to doctors that their immune systems were not working properly.
Two of the men had already died by the time the report is published.
One month later, on the 3rd July (1981), a second MMWR was published. This one mentioned further cases of Pneumocystis carinii pneumonia and cited 26 cases of a rare form of cancer known as Kaposi’s sarcoma, which is caused by a viral infection:

These two MMWRs were the first official reports mentioning what would go on to become known as the AIDS epidemic – a devastating, ongoing global health issue that has thus far claimed 35+ million lives.
It was also the very beginning of what would be an amazing story of patient advocacy. The one that would become the template for many future efforts. Part of that advocacy effort was called “ACT UP”, and in today’s post we will discuss what the movement was and how they achieved some amazing accomplishments.
But before we get to that, let’s start at the beginning:
What exactly is AIDS?
Acquired immune deficiency syndrome (or AIDS) is a progressive failure of the immune system – the body loses its ability to fight infections. AIDS is the most severe phase of an HIV infection. Without treatment, average survival period after infection with HIV is between 9 – 12 years.

What is HIV?
Very simply, Human immunodeficiency virus (or HIV) – as the name suggests – is a virus.
More specifically, it is a family of viruses.
Two types of HIV have been characterised: HIV-1 and HIV-2. HIV-1 is the virus that was initially discovered, and it is is the cause of the majority of HIV infections worldwide. HIV-2 is less infectious and primarily focused in West Africa. These two subtypes of HIV can be further broken down into numerous subgrouping (Click here to read more about these). HIV-1 can be divided into 4 different groups of which Group M can be further subdivided. And there are 8 known HIV-2 groups (A to H).

Source: Avert
HIV is a lentivirus.
These are RNA-based viruses, which can insert their genomic information into the DNA of the host cell that has been infected. HIV is made up of a viral envelope (or outer membrane) that surrounds an internal membrane called the capsid.
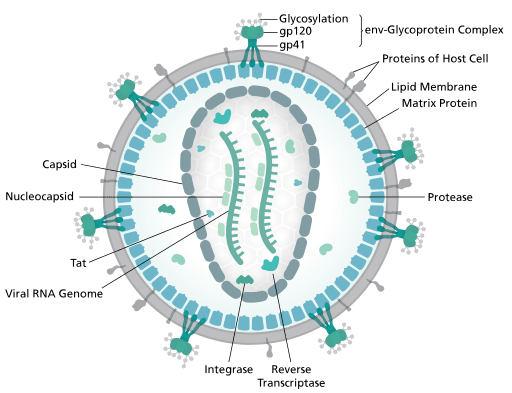
The structure of the HIV virus. Source: Wikipedia
The capsid protects two pieces of RNA, which provides 9 genes (the instructions for making different proteins) that are required for replication:

The structure of HIV RNA (9 genes highlighted in different colours). Source: Wikipedia
HIV infects a variety of cells associated with the immune system (such as T cells, macrophages, and microglial cells). The virus infects and then uses these cells to self replicate, which ultimately kills the cell. By attacking the cells of the immune system, this leaves an infected individual vulnerable to normally harmless infections.
How is the virus spread?
HIV can be spread by the transfer of bodily fluids, such as blood and semen.
Why is HIV so difficult to treat?
The virus has been very difficult to deal with because it has a very fast replication cycle (generating approximately 1010 viral particles (or virions) per day) and a high genetic mutation rate (approximately 3 x 10−5 per nucleotide base per cycle of replication). Random variations occur in the genomic material of the virus with each replication, resulting in a changing target over time.
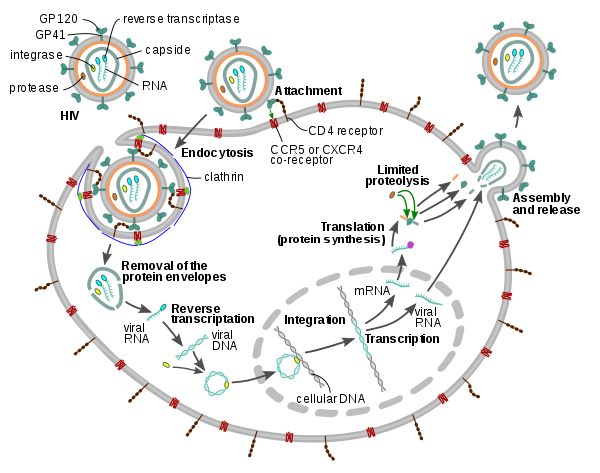
The cycle of replication of HIV. Source: Wikipedia
How many people are affected by HIV/AIDS?
According to the World Health Organization, over 35 million people have died of HIV/AIDS; and according UNAIDS, as of 2016, approximately 36.7 million people in the world were living with HIV (Source).
To put that in perspective for you, 36 million is equivalent to the entire population of Canada.
Currently, the majority of those infected with HIV live in Africa:
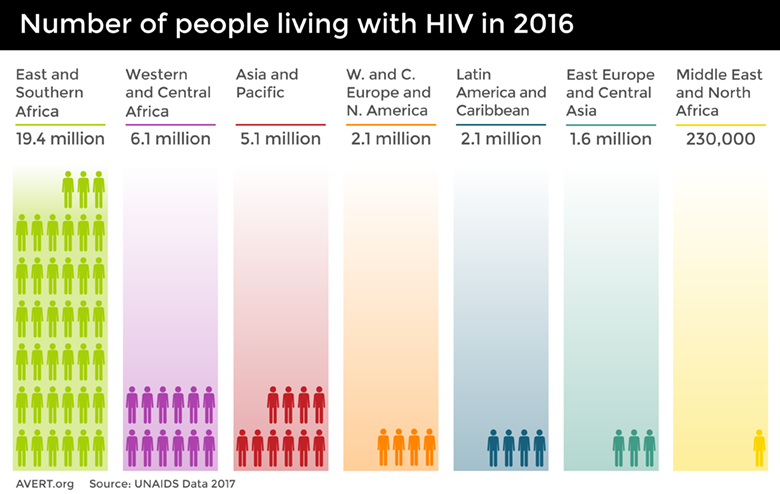
Source: Avert
Ok, in the intro you mentioned AIDS advocacy and ACT UP. What exactly is ACT UP?
1987 was a big year for the AIDS community.
The number of deaths attributed to AIDS in the US that year alone had reached 4,135 (including that of entertainer Władziu Valentino Liberace) – bringing the total number of known AIDS-associated deaths in the US to more than 20,000.

Liberace. Source: Telegraph
The average survival time for a person diagnosed with AIDS in 1987 was just 27 months. But that was to slowly start changing – 1987 was also the year that AZT (also known as Zidovudine, Retrovir® produced by Glaxo Wellcome) became the first anti-HIV drug to be approved by the FDA. The recommended dose was one 100mg capsule every four hours around the clock.

AZT. Source: Spin (a fascinating article)
And in March of 1987, at the Lesbian and Gay Community Services Center in New York city, an advocacy group called ACT UP was started.
“AIDS Coalition to Unleash Power” (or ACT UP) is “an international direct action advocacy group working to impact the lives of people with AIDS(PWAs) and the AIDS pandemic to bring about legislation, medical research and treatment and policies to ultimately bring an end to the disease by mitigating loss of health and lives” (Wikipedia).
One person in particular stands out in the formation of ACT UP: Larry Kramer.

Larry Kramer. Source: Hollywoodreporter
Frustrated with bureaucratic paralysis and the seeming apathy of society to the developing AIDS crisis, Kramer was wishing to engage in a more direct action approach to gain the attention for the affected community. These motives were the catalyst in the formation of ACT UP.
Three weeks after the formation of ACT UP, 250 members demonstrated in New York (at Wall Street and Broadway) demanding greater access to experimental AIDS drugs and for a coordinated national policy to fight the disease. The date was the 24th March, and 17 people were arrested.

First demonstration. Source: ACT UP
On the 1st June, ACT UP joined other national activist groups in civil disobedience at the White House in Washington, DC. In a perfect display of the AIDS-phobia that was emerging during this period, the police wore rubber gloves while arresting the protesters.
Three days later, when Northwest Orient Airlines announced that it was going to refuse passage to people with AIDS, an ACT UP protest erupted in the airline’s New York offices. Lawsuits were taken out against Northwest and the policy is quickly reversed.
Episodes like this continued.
Relentlessly.
(Click here for a history of examples)
ACT UP was also very provocative with their art work:

It is important to understand that ACT UP was not working in isolation, there were other AIDS advocacy groups involved in calling for change and action. But the in-your-face style of ACT UP certainly attracted a lot of attention.
Initially this attention grabbing effort by ACT UP was ignored by a lot of people – it was simply considered frustrated sick people yelling “Why don’t you care if I die?” in the faces of politicians. There was the belief that the affected people were angry and loud, but not really offering any solutions. But gradually these continuous activities caught the hearts and minds of the general public, particularly as it became apparent that the AIDS epidemic was just isolated to the gay communities.
In addition, a well considered agenda backing the activism started to develop from the ACT UP meetings. For example, in June 1989, ACT UP activists presented their National AIDS Treatment Research Agenda outlining 12 issues where they wanted to see reform in AIDS-related research (if you haven’t read it, you should. It makes for interesting reading – demonstrating how far we have/haven’t come).
All of this AIDS advocacy combined eventually had a major impact. The key accomplishments of the AIDS movement in the late 1980s/early 1990s resulted in:
- Patient-driven clinical trial designs: Patient activists got educated about the nuisances of clinical trials and in conjunction with physician and scientist allies set the NIH agenda for research and clinical trials
- Expanded access to new drugs: AIDS activists, in a race to save their own lives, reduced regulatory hurdles to accessing drugs that might
- Congressional funding for research: Funding for AIDS research at the NIH increased from $5.6 million in 1982 to $1.62 billion in 1998 (understand that $1.62 billion represented 12 percent of the entire NIH budget that year!).
- Congressional funding for care: In addition to research, Congress also invested in services for prevention, care and assistance for people living with HIV. In 1990 it provided an initial $200 million. By 1994, Congress had allocated $632 milllion through this act.
Most importantly, the life expectancy of someone living with HIV has improved. In 1996, the total life expectancy for a 20-year-old person with HIV was just 39 years. In 2011, the total life expectancy had increased to approximately 70 years (Source).
And these accomplishments are even more impressive when you put them into context, as they were initially achieved during a period of denial (“this is just a gay community problem”) and then a slowly emerging panic about the issue of AIDS (there were serious calls for labelling and quarantining of HIV-infected individuals – isolating them to slow the spread of the condition).
There are now books and films about the advocacy effort – one particularly interesting film is called “How to Survive a Plague” by David France. It is fascinating, but be warned that some of the content may upset some readers.

Source: Dvdsreleasedates
What does any of this have to do with Parkinson’s?
This post was not written with a ‘call to arms’ idea in mind regarding direct action advocacy.
In their interesting book, ‘Zero to One’ authors Peter Thiel and Blake Masters push the idea that there will only ever be one Steve Jobs, one Bill Gates, one Michael Jordan, one Barack Obama. Everyone else who follows and tries to replicate their success is a ‘me too’ who will not carry the same level of impact.
Source: Wikipedia
In addition, ACT UP achieved a great deal during the early years of the AIDS epidemic, but their in your face approach also isolated them in the eyes of many people. While their dire situation drew sympathy, the attacks on politicians and pharmaceutical company CEOs were viewed negatively by some. One has to question whether such an approach would work as effectively today.
What can be taken away from the ACT UP movement is the need for collectively, patient-focused effort. But this should not be isolated to just Parkinson’s.
The Parkinson’s foundation estimates that 10 million people around the world live with Parkinson’s (Source). Dementia affects close to 50 million people globally (Source). Without adding in the statistics for multiple sclerosis, motor neuron disease/ALS, etc, it is easy to see how neurodegenerative conditions can be collectively viewed as the ‘AIDS’ (or the cancer) of the modern era.
And given that age is the most common risk factor associated with neurodegenerative conditions like Parkinson’s and Alzheimer’s, and western societies are gradually getting older, there is a desperate need to really address the problem.
If theses conditions are going to be a burden on society in coming years, why is 10% of the NIH research budget not being dedicated to them now (as it was with AIDS).
And there in lies another aspect of the ACT UP/AIDS advocacy story that we haven’t discussed yet. I just wrote “as it was with AIDS” (past-tense). Success is a dangerous thing in the absence of an actual cure. One curious aspect of this story is that the AIDS advocacy effort has been so successful, that there are now calls to reduce funding for AIDS associated efforts and put the money to other more needed purposes. For example, earlier this year the White House budget for fiscal year 2018 proposed cuts to the CDC, including programs on HIV. It proposed cuts to the Ryan White HIV/AIDS Program – which is one of the US’s signature HIV treatment program, caring for over half a million people – AND an $800 million cut to global AIDS funding.
Such a scenario should be taken into account in the planning of outcomes for any future advocacy efforts.
So, what does it all mean?
This post was initiated by an discussion with a reader earlier in the year about the ACT UP movement (Thanks Paul). After editing an initial draft of it, however, I found myself reluctant to post it (it had nothing to do with research and felt like a rant). That draft post was resurrected though after recently listening to Ben Stetcher’s recent interview with Prof Ray Dorsey (Click here to listen to/read that excellent interview – and if you don’t already follow Ben’s website, you should! Read the interview with Prof Hilal Lashuel!).
This post is intended as a ‘food for thought’ discussion of how others have undertaken the task of advocacy for a particular medical condition. And the background reading for it has certainly made for some interesting summer reading. While I don’t think direct action is the answer (happy to be debated on this), I do believe that a more collective effort from the neurodegenerative community as a whole is necessary. And the Parkinson’s community could be proactive in initiating that movement.
As I say, food for thought – feel free to ignore.
Back to Parkinson’s research in the next post.
“If it fails, admit it frankly and try another. But above all, try something” – Franklin D. Roosevelt
The banner for today’s post was sourced from Wikipedia

Hi Simon,
I really, really liked this post. I found it particularly relevant in view of the recent tv programmes about the suffragettes and how they were almost ‘forced’ into becoming radicalised as they were ignored – not that I think one should become radical. Your ancestors were ahead of the game on that score. I think you wrote very well about an issue that a lot of us are airing in private. Dare I say apathy is a common feature of PD as well as fatigue, also prevalent in MS…………….
LikeLike
Hi Hilary,
Thanks for your comment – glad you liked the post.
Apathy could indeed be an aspect of the advocacy issue. But I also suspect that the NY HIV/AIDS community had a stronger sense of community than the current PD community. ACT UP had an advantage as it rose largely out of the gay community there, so there was already a sense of solidarity, and HIV/AIDS gave that community something to focus its energy on. The Parkinson’s community, on the other hand, are coming from all sorts of backgrounds. Finding unity here is definitely harder. But having said that, the suffragettes all came from different backgrounds as well. Maybe I need to do some reading on them…
Kind regards,
Simon
LikeLike
Thanks, Simon, this is fascinating. As PwP, we face a subtly different challenge. The AIDS crisis was driven by a short term urgency; people were dying within a matter of months, it was infectious, it was transmitted via bodily fluids. With the view of most politicians and decision makers usually only to the end of their current term, it was both urgent and important. It was very much a “today” issue, both urgent and important..
Parkinson’s is not killing people in a matter of months, not that it is unimportant – we can see that ourselves, The projections of prevalence outline the massive potential impact on public health, both people and budgets. From the viewpoint of politicians and decision makers, it’s a “tomorrow” issue; important, but not urgent.
The mega issue of tomorrow is climate change. Things must be done today to avoid the problems of the future. Yet somehow we have a consensus on action (almost….) which is both urgent and important.
So perhaps we need to learn from ACTUP and climate change activism.
LikeLike
Hi Kevin,
Thanks for the comment – as always an interesting one. I think Pamela’s example above of the suffragettes is a good one – they were not dying within months, but look at what they achieved. So how was their situation different? What is the missing ingredient that pushes a movement/issue into the public eye?
Kind regards,
Simon
LikeLike
This post posed an interesting question to me – how do we go from ‘zero to one’ for a Parkinsons cure strategy? As Simon points out, the ACTUP approach won’t be as effective a second time. But Parkinson’s as a disease has different characteristics, suggesting a different strategy would be a better advocacy fit in any case. People have Parkinsons for a long time, and it does not prompt fear in the same way as HIV.
LikeLike
Hi Paula,
Thanks for your comment. With all advocacy, there has to be a ‘why’. Why should anyone from outside of the Parkinson’s community stop and take notice/action? With HIV/AIDS, I actually suspect that the ‘why’ was more the fear of a deadly virus getting out of control (rather than the antics of ACT UP) that actually galvanised the action taken by policy makers.
The ‘why’ with neurodegeneration could be the demographics – for example, 1/3 of the Japanese population is now over the age of retirement. The burden on society from dementia, Parkinson’s, etc is going to be great as the western populations continue to age. Thus, the reason I suggest a collaborative effort by the neurodegenerative communities. Individually, the resources get divided, but together more can be done. Just one person’s opinion though.
Kind regards,
Simon
LikeLike
Wow. An awesome post Simon! Raises the deeply psychological warfare of Parkinson’s NOT being considered a ‘terminal’ disease…at least to me!
Who thought up that bloody saying ‘you don’t die with it, you die from it’? I’m gonna bring my hubby’s worn-out body to them and show them what it WILL say on his death certificate.
Great stuff….really happy you did post it!
LikeLike