
|
Dense spherical clusters of a protein – called Lewy bodies – are one of the classical hallmarks of the Parkinsonian brain. They are a common pathological feature, but curiously they are not present in all cases of Parkinson’s. For example, some individuals with certain forms of Parkinson’s associated with specific genetic mutations do not exhibit any Lewy bodies. Variations in a region of DNA called LRRK2 will increase one’s risk of developing Parkinson’s, but many of those who go on to develop LRRK2-associated Parkinson’s will have a complete absence of Lewy bodies in their brains. These cases have represented an enigma for the Parkinson’s research community and have been difficult to reconcile. Recently, however, researchers from the University of Pennsylvania have reported a different kind of protein clustering in these LRRK2-associated cases with “no Lewy bodies”. The accumulating protein is called Tau. In today’s post, we will look at what Tau is, review what the new research report found, and discuss what this discovery could potentially mean for the future treatment of Parkinson’s.
|
 Neuropathologists conducting a gross examination of a brain. Source: NBC
Neuropathologists conducting a gross examination of a brain. Source: NBC
At present, a definitive diagnosis of Parkinson’s can only be made at the postmortem stage with an examination of the brain.
Until that moment, all cases of Parkinson’s are ‘suspected’. When a neuropathologist makes an examination of the brain of a person who passed away with the clinical features of Parkinson’s, there are two characteristic hallmarks that they will be looking for in order to provide a final diagnosis of the condition:
1. The loss of specific populations of cells in the brain, such as the dopamine producing neurons in a region called the substantia nigra, which lies in an area called the midbrain (at the base of the brain/top of the brain stem). As the name suggests, the substantia nigra region is visible due to the production of a ‘substance dark’ molecule called neuromelanin in the dopamine neurons. And as you can see in the image below, the Parkinsonian brain has less dark pigmented cells in the substantia nigra region of the midbrain.
 The dark pigmented dopamine neurons in the substantia nigra are reduced in the Parkinsonian brain (right). Source:Memorangapp
The dark pigmented dopamine neurons in the substantia nigra are reduced in the Parkinsonian brain (right). Source:Memorangapp
2. Dense, circular clusters (or aggregates) of protein within cells, which are called Lewy bodies.
 A cartoon of a neuron, with the Lewy body indicated within the cell body. Source: Alzheimer’s news
A cartoon of a neuron, with the Lewy body indicated within the cell body. Source: Alzheimer’s news
A Lewy body is referred to as a cellular inclusion, as they are almost always found inside the cell body. They generally measure between 5–25 microns in diameter (5 microns is 0.005 mm) and thus they are tiny. But when compared to the neuron within which they reside they are rather large (neurons usually measures 40-100 microns in diameter).
 A photo of a Lewy body inside of a neuron. Source: Neuropathology-web
A photo of a Lewy body inside of a neuron. Source: Neuropathology-web
Do all Parkinson’s brains have Lewy bodies?
Funnily enough, no.
And this is where the wheels fall off the wagon in our understanding (and ‘definitive’ definition) of Parkinson’s.
What do you mean?
Recently this research report was published:
 Title: Alzheimer’s disease tau is a prominent pathology in LRRK2 Parkinson’s disease.
Title: Alzheimer’s disease tau is a prominent pathology in LRRK2 Parkinson’s disease.
Authors: Henderson MX, Sengupta M, Trojanowski JQ, Lee VMY.
Journal: Acta Neuropathol Commun. 2019 Nov 16;7(1):183.
PMID: 31733655 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers were interested in examining the postmortem brains of cases of Parkinson’s with no evidence of Lewy bodies. They focused their attention on samples that came from people with Parkinson’s who carried a genetic variation in their LRRK2 gene.
What is the LRRK2 gene?
Leucine-rich repeat kinase 2 (or LRRK2 – pronounced ‘lark 2’) is a regions of your DNA that provides the instructions for making a particular protein (the LRRK2 protein). These functional sections of your DNA that provide instructions for making proteins are called genes.
The LRRK2 gene is associated with Parkinson’s. In fact, it is also known as PARK8 (Click here to read more about PARK genes and the genetics of Parkinson’s). When certain errors or variations occur in the LRRK2 region of a person’s DNA, it increases that individuals risk of developing Parkinson’s
Also known as ‘Dardarin‘ (from the Basque word “dardara” which means “trembling”), LRRK2 protein is an enzyme. An enzyme is a protein that acts as a catalyst in living organisms. It regulates the rate of activity in a biological reaction. And LRRK2 is a busy enzyme as it has many functions within a cell – from supporting efforts to move things around inside the cell to helping to keep the power on (involved with mitochondrial function).
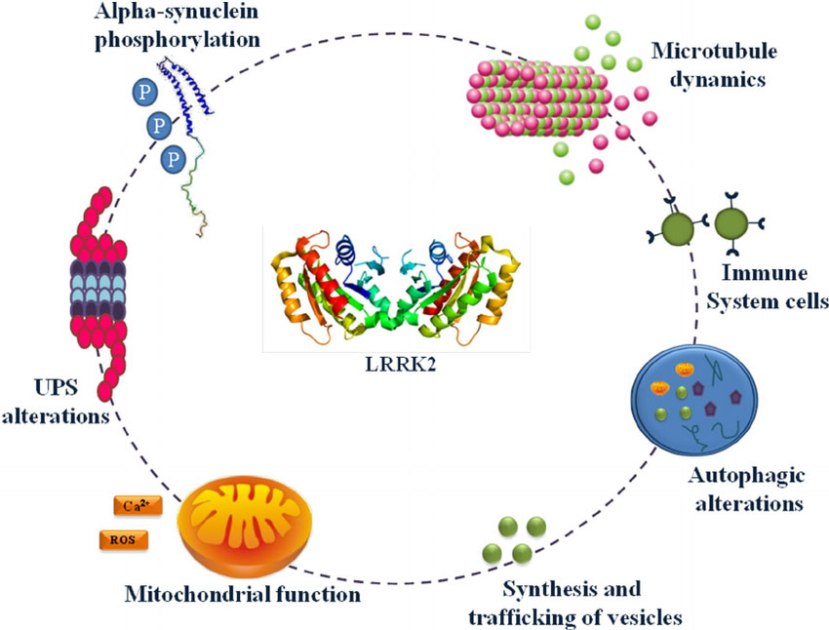
The many jobs of LRRK2. Source: Researchgate
The LRRK2 gene is made up of many different regions. Each of those regions is involved with the different functions of the eventual protein. As you can see in the image below, the regions of the LRRK2 gene have a variety of different functions:
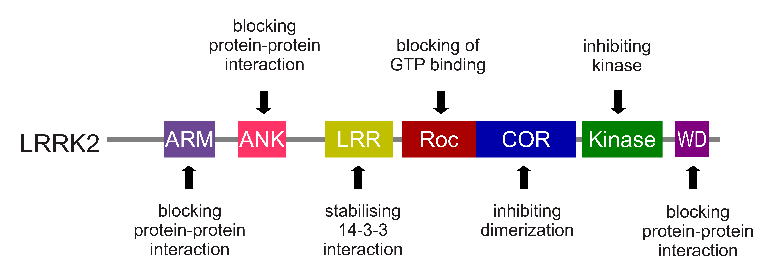
The regions and associated functions of the LRRK2 gene. Source: Intechopen
Genetic errors or variations within the LRRK2 gene are recognised as being some of the most common with regards to increasing ones risk of developing Parkinson’s – LRRK2 variants are present in approximately 1-2% of all cases of Parkinson’s.
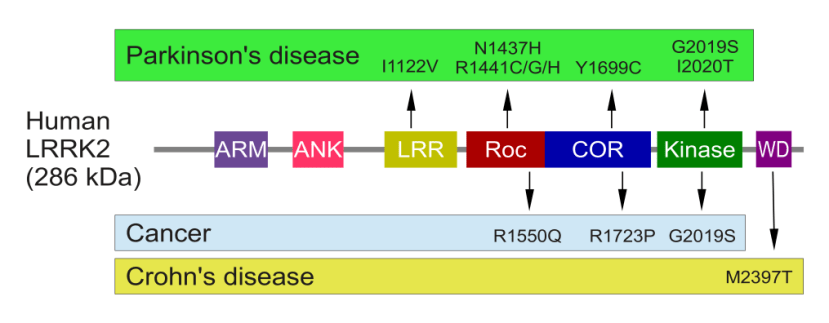
The structure of Lrrk2 and where various mutations lie. Source: Intech
As the image above suggests, mutations in the PARK8 gene are also associated with Crohn’s disease (Click here and here for more on this) – though that mutation is in a different location to those associated with Parkinson’s. And one particularly common Parkinson’s-associated LRRK2 mutation – called G2019S – is also associated with increased risk of certain types of cancer, especially for hormone-related cancer and breast cancer in women – Click here to read more about this. If you have a G2019S mutation, no reason to panic – but it is good to be aware of this association and have regular check ups.
The G2019S mutation (the name designates its location on the gene) is the most common LRRK2 mutation. In some populations of people around the world, the G2019S variation can be found in 40% of people with Parkinson’s (Click here to read more about this).
But what is interesting about this mutation is that it gives rise to a LRRK2 enzyme that is extremely hyperactive.
The structure of LRRK2 protein. Source: Wikipedia
As a protein, LRRK2 interacts with many different types of other proteins, and you can imagine that in a finely balanced environment like the cells that a mutant ‘hyperactive’ form of LRRK2 is going to cause problems. The consequences of this constantly active form of LRRK2 protein is believed to be influential in the cell death in LRRK2-associated Parkinson’s.
Thus, biotech companies have been looking for compounds that help to inhibit or modulate LRRK2 activity (Click here to read a previous SoPD post regarding an example of a biotech company – called Denali – which is taking this approach).

|
RECAP #1: Genetic mutations in a region of DNA called LRRK2 increase one’s risk of developing Parkinson’s. Drugs that inhibit LRRK2 are being developed as potential therapies for Parkinson’s. Many cases of LRRK2-associated Parkinson’s do not have any Lewy bodies in their brains.
|
Interesting. But you said above that the researchers were looking at postmortem brains from people with LRRK2 genetic mutations and no lewy bodies. How many people with LRRK2-associated Parkinson’s have no lewy bodies?
It varies between studies, but approximately 20–55% of the reported cases of LRRK2-associated Parkinsons that have been assessed at the postmortem stage have been found to have no apparent lewy bodies (Click here and here to read more about this).
In these cases, the number of dopamine neurons in the substantia nigra are severely reduced and the individual displays all the clinical symptoms of Parkinson’s, but there are no Lewy bodies.
So in this new study that we are reviewing in today’s post, the researchers were curious to examine the postmortem brains of people with LRRK2-associated Parkinson’s that have no evidence of Lewy body pathology. They wanted to analyse these brains for the presence of three proteins that are considered markers of the major neurondegenerative conditions alpha synuclein (a marker of Parkinson’s), beta amyloid (a marker of Alzheimer’s), and Tau.
What is Tau?
Have a look at this image:
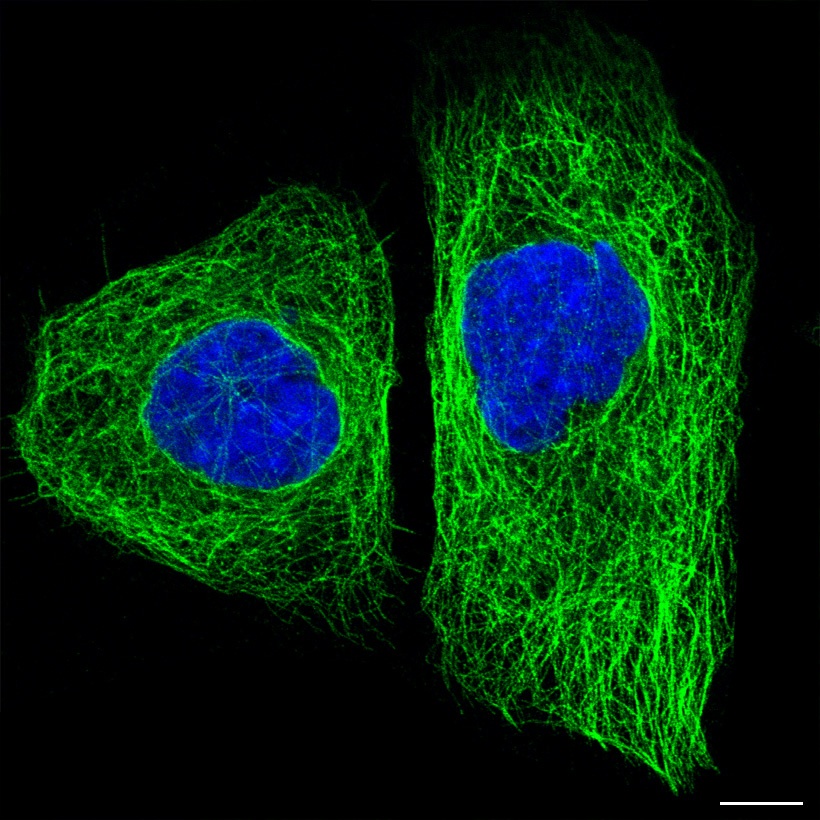
Tau protein (green) inside two cells. Source: The human protein atlas
In the image above you will see a fluorescent photo of two cells that have been labelled with two different dyes: one that highlights the nucleus (in blue) and another that stains the microtubules (in green). Everything else in the cell (membrane and all) is left invisible by this labelling process.
Pretty huh?
Pretty. But what are microtubules?
Microtubules are the highways and byways inside a cell.
They are structures inside of cells that are involved with both cellular and intracellular transportation. That is to say, these skeleton-like structures help cells move from place to place within the body (‘cellular transportation’), but they also aid in the movement of proteins from place to to within the cell (‘intracellular transportation’). On top of this, microtubules also play an important function in cell division.
The stability and maintenance of these microtubles relies on proteins like Tau.
Got it. Now what is Tau?
Tau is protein that is very abundant in the brain. It is generated from the RNA (the instructions for making protein) of the MAPT gene, located on chromosome 17 of your DNA.
Tau protein is a microtubule-associated protein – meaning it directly interacts with microtubules. It functions by stabilising these highways and byways inside a cell. Basically, this protein holds together the roads which allows vesicles (the small bags of material) to be moved around the cell (by transporter proteins like kinesin).
 TAU: a stabilising presence. Source: Hindawi
TAU: a stabilising presence. Source: Hindawi
So why is Tau interesting?
Because Tau is associated with both Parkinson’s AND Alzheimer’s disease.
In both conditions there is a build up of Tau protein, which accumulates and clusters (or ‘aggregates’) in a similar fashion to our old friend the Parkinson’s-associated protein alpha synuclein (Click here for a good review article on this topic).
 Tau protein in Alzheimer’s disease. Source: Dreamstime
Tau protein in Alzheimer’s disease. Source: Dreamstime
|
RECAP #2: Tau is a protein that accumulates in neurodegenerative conditions like Parkinson’s and Alzheimer’s. Its normal function is to stabilise the highways and byways inside a cell, aiding in the intracellular transportation of resources.
|
Interesting. So what did the researchers find in this new study?
The researchers collected samples of postmortem brain from 12 people who passed away with LRRK2-associated Parkinson’s and analysed them for levels of alpha synuclein, beta amyloid, and Tau. They found accumulating alpha synuclein protein – but no Lewy bodies – in 63.6% of the brains.
Of particular interest, the researchers found Tau protein pathology in 100% of the samples (and it was abundant in 91% of cases).
Curiously, samples from one postmortem case of an individual who had schizophrenia and a LRRK2 genetic mutation (G2019S) presented no accumulation of Tau protein. The aggregation of Tau seemed to be specific to the cases of LRRK2-associated Parkinson’s.
Wow. That is interesting. Did they investigate further?
Yes they did.
There are different forms of Tau protein which can be labelled. For example, there is a form of Tau that is specific to Alzheimer’s, but not other neurodegenerative conditions (like Progressive supranuclear palsy, corticobasal degeneration, or Pick’s disease).
When the investigators examined the samples from LRRK2-associated Parkinson’s brains, they found that the Alzheimer’s form of Tau was most prevalent.
And curiously, higher levels of this Alzheimer’s form of Tau was associated with higher levels of alpha synuclein protein, suggesting that “Tau and alpha synuclein pathology burden are associated“. But the researchers noted that “while both pathologies were abundant in many of the same regions, they were rarely in the same cell, suggesting that the association of these two pathologies is not through direct cross-seeding” – meaning that the investigators thought that the two aggregating proteins were acting individually.
Is this the first time a connection between LRRK2 and Tau has been found?
No.
Back in 2013, this research report was published:
 Title: LRRK2 phosphorylates novel tau epitopes and promotes tauopathy.
Title: LRRK2 phosphorylates novel tau epitopes and promotes tauopathy.
Authors: Bailey RM, Covy JP, Melrose HL, Rousseau L, Watkinson R, Knight J, Miles S, Farrer MJ, Dickson DW, Giasson BI, Lewis J.
Journal: Acta Neuropathol. 2013 Dec;126(6):809-27.
PMID: 24113872 (This report is OPEN ACCESS if you would like to read more about this)
In this study, the researchers demonstrated not only that LRRK2 and tau interact (LRRK2 phosphorylates multiple forms of tau), but also that high levels of LRRK2 protein in a mouse model of tauopathy increased the aggregation of tau protein.
In addition, it has been reported that LRRK2 could be affecting tau in other ways. For example, last year this report was published:
 Title: Lrrk promotes tau neurotoxicity through dysregulation of actin and mitochondrial dynamics.
Title: Lrrk promotes tau neurotoxicity through dysregulation of actin and mitochondrial dynamics.
Authors: Bardai FH, Ordonez DG, Bailey RM, Hamm M, Lewis J, Feany MB.
Journal: PLoS Biol. 2018 Dec 20;16(12):e2006265.
PMID: 30571694 (This report is OPEN ACCESS if you would like to read more about this)
In this study, the researchers found that in flies LRRK and Tau interact with each other and this activity can affect another protein called actin.
What is actin?
Do you remember we talked about microtubules above, near the top of this post?
Well, microtubules are a type of filament (a slender threadlike fibre inside of cells) – in fact they are the largest with a diameter of about 25 nanometers – and they are made of a protein called tubulin. Actin filaments are the smallest type of filament – diameter measuring only about 6 nm – and they are (as the label on the can suggests) made of a protein called actin.
Part of the function of Tau protein is to bind to actin and stabilise it.
But the researchers found that LRRK causes Tau to over stabilise actin, which results in a breakdown of the dynamic transportation of resources around a cell. In ability to move proteins around cells results in mitochondrial dysfunction (mitochondria are the power stations of cells), which promotes cellular stress and ultimately neurodegeneration.
The investigators found that both increasing and decreasing the levels of LRRK in flies resulted in enhances tau neurotoxicity.
It should be noted that all of the data from this research report was collected in flies (drosophila) which only have 1 LRRK gene (hence the use of just ‘LRRK’ here). Mice and humans have 2 LRRK genes, and it is yet to be determined if this result translates to humans.
Above you said that there are LRRK2 inhibitors being developed, but are there any treatments for tau aggregation?
Given its association with Alzheimer’s, there are quite a few experimental therapies being developed that target Tau.
For example, Gosuranemab (aka BIIB092, BMS-986168, IPN007) is a monoclonal anti-tau antibody. This is a type of immunotherapy, which involves boosting the immune system to target and remove particular proteins from the body – in this case aggregated Tau protein is being removed (Click here to read a previous SoPD post about immunotherapy).
First developed by a biotech called iPierian, which was bought in 2014 by the pharma company Bristol-Myers Squibb. In 2017, Biogen licensed Gosuranemab and has been developing it further.

There are currently 4 ongoing clinical trials, and of particular interest to us here is the PASSPORT study which is evaluating Gosuranemab in people with Progressive Supranuclear Palsy (or PSP) – a type of Parkinsonism (Click here to read more about this study).
Two other immunotherapies targetting Tau include ABBV-8E12 (aka C2N-8E12) being developed by C2N Diagnostics and AbbVie, and Semorinemab (aka R07105705) which is being progressed by Genentech and its parent pharma company Roche.
Gosuranemab and these other immunotherapies target extracellular Tau – meaning tau protein that is outside the cell. The theory being that aggregated Tau is being passed between cells and this is how the pathology/disease is spreading. But there are also small molecules being developed, which target intracellular aggregated Tau (protein within cells) and block any further clustering within the cell.
One example of this is ACI-3024 which is being developed by the biotech firm AC Immune and the pharma company Eli Lilly.
![]() ACI-3024 is an oral small molecule inhibitor of Tau aggregation, which is currently being clinically tested in Phase I safety/tolerability trial (Click here to read more about this). This drug is different to the immunotherapy approach as ACI-3024 can enter cells and blocks the aggregation of Tau.
ACI-3024 is an oral small molecule inhibitor of Tau aggregation, which is currently being clinically tested in Phase I safety/tolerability trial (Click here to read more about this). This drug is different to the immunotherapy approach as ACI-3024 can enter cells and blocks the aggregation of Tau.
And novel Tau-targetting molecules are regularly being proposed – for example, the biotech firm Oligomerix very recently identified another molecule that can inhibit the aggregation of Tau (Click here to read more about this).
![]() For those interested in reading more about experimental treatment approaches for Tau – click here to read a good recent review of experimental treatments under clinical development.
For those interested in reading more about experimental treatment approaches for Tau – click here to read a good recent review of experimental treatments under clinical development.
|
RECAP #3: Tau aggregation appears to be present in LRRK2-associated Parkinson’s brains (in the absence of Lewy bodies). Numerous biotech companies are developing therapies targetting Tau aggregation.
|
So what does it all mean?
For a long time the absence of Lewy bodies in the brains of some cases of Parkinson’s has been a complicating factor in our understanding of the condition. Now, however, there is evidence to suggest that an Alzheimer’s-associated protein (Tau) may be involved in a particular subtype of Parkinson’s (LRRK2-associated PD).
In addition to raising a lot of obvious questions as to how this circumstance of aggregated protein arises, this new data also suggests that our current notions of Parkinson’s may be rather basic (to put it politely). There has been much talk in the research community of needing to better subdivide “Parkinson’s syndrome” (a syndrome being a group of conditions that share common features).
With these new insight comes new opportunity, and it will be interesting for the LRRK2-associated Parkinson’s research community to take advance of some of the resources in the Tau research field (such as the imaging capabilities – click here for a useful review of Tau imaging) to better explore – and potentially treat – this subtype of Parkinson’s.
A combining of the two research fields may also yield beneficial treatment results, if by combining LRRK2 inhibition and some form of Tau dissaggregation treatment approaches, we can slow the progression of the condition. I am wildly speculating here, but current research efforts could explore such opportunities.
But first, independent replication of the current findings with a larger set of samples need to be presented before we get too carried away.

All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like!
The banner for today’s post was sourced from ActaNeuropath

Brilliant, super clear as always, next!
LikeLike
Thanks Martin, glad you liked the post.
More?
Ok.
LikeLike
thanks for making this basic research available to non-scientists
the recaps are good
Mac Green
LikeLike
I am especially interested in the Tau protein and PSP, When are the Passport results likely to be avaiable?
LikeLike
Thank you for the very interesting post Simon. I am surprised that the two varieties of the PD you described (alpha-SN and tau protein) are not treated as two distinct illnesses. It appears that the dopamine deficiency in these cases have very different causal underlying processes and very likely they will require different approached for treatment. If I recall it right immunotherapy targeting tau proteins in Alzheimer’s disease didn’t yield good results. It will be interesting to see if PD is going to be different.
Felix
LikeLike