
|
Biotech firm Denali announced the dosing of the first person in their Phase Ib clinical study of their experimental treatment for Parkinson’s called DNL201. DNL201 is an inhibitor of a Parkinson’s-associated protein called Leucine-rich repeat kinase 2 (LRRK2). In Parkinson’s, there is evidence that LRRK2 is over activate, and by inhibiting LRRK2 Denali is hoping to slow the progression of Parkinson’s. In today’s post, we will discuss what LRRK2 is, what evidence exists for DNL201, and what the new clinical trial will involve.
|

Founded in 2013, by a group of former Genentech executives, San Francisco-based Denali Therapeutics is a biotech company which is focused on developing novel therapies for people suffering from neurodegenerative diseases. Although they have product development programs for other condition (such as Amyotrophic Lateral Sclerosis and Alzheimer’s disease), Parkinson’s is their primary interest.
And their target for therapeutic effect?
The Parkinson’s-associated protein called Leucine-rich repeat kinase 2 (or LRRK2).
What is LRRK2?
Also known as ‘Dardarin‘ (from the Basque word “dardara” which means “trembling”), LRRK2 is an enzyme that has many functions within a cell – from supporting efforts to move things around inside the cell to helping to keep the power on (involved with mitochondrial function).
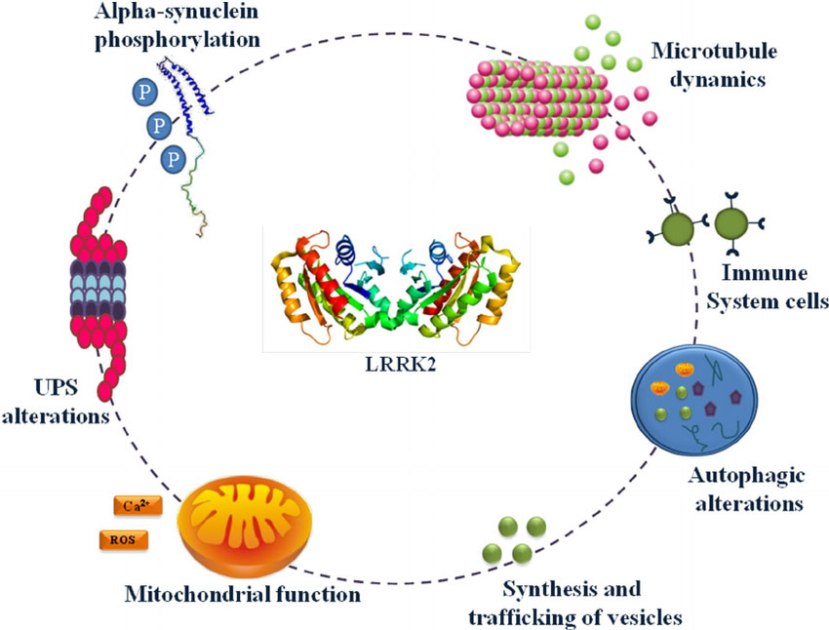
The many jobs of LRRK2. Source: Researchgate
The gene that provides the instruction for making the LRRK2 enzyme resides on the 12th chromosome, in an area of DNA referred to as ‘PARK8’ (one of the Parkinson’s disease-associated genetic regions). The LRRK2 gene is located within the PARK8 region, and it is made up of many different sections, each of which is involved with the different functions of the eventual protein.
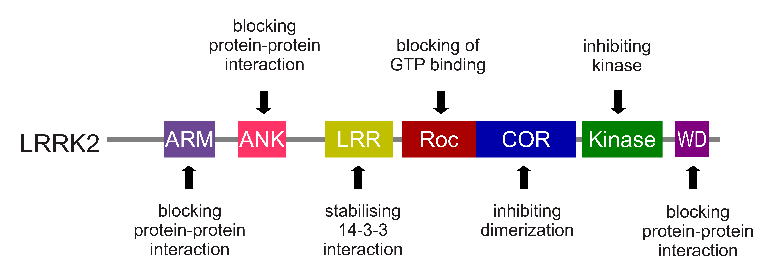
The regions and associated functions of the LRRK2 gene. Source: Intechopen
Genetic mutations within the LRRK2 gene are recognised as being some of the most common with regards to increasing ones risk of developing Parkinson’s disease (they are present in approximately 1-2% of all cases of Parkinson’s).
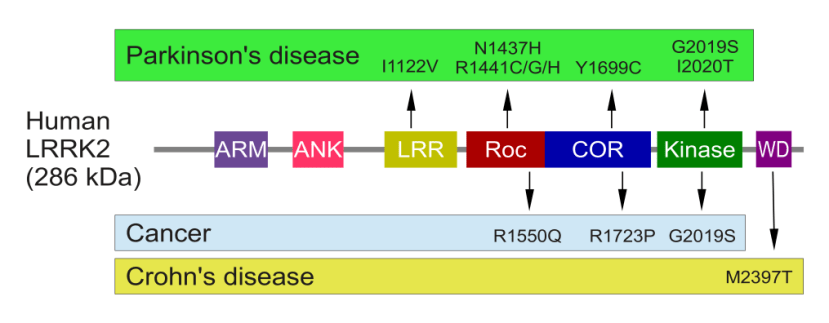
The structure of Lrrk2 and where various mutations lie. Source: Intech
As the image above suggests, mutations in the PARK8 gene are also associated with Crohn’s disease (Click here and here for more on this) – though that mutation is in a different location to those associated with Parkinson’s. And one particularly common Parkinson’s-associated LRRK2 mutation – called G2019S – is also associated with increased risk of certain types of cancer, especially for hormone-related cancer and breast cancer in women – Click here to read more about this. If you have a G2019S mutation, it is good to be aware of this association and have regular check ups.
The G2019S mutation (the name designates its location on the gene) is the most common LRRK2 mutation. In some populations of people it can be found in 40% of people with Parkinson’s (Click here to read more about this). But what is interesting about this mutation is that it gives rise to a LRRK2 enzyme that is hyperactive.
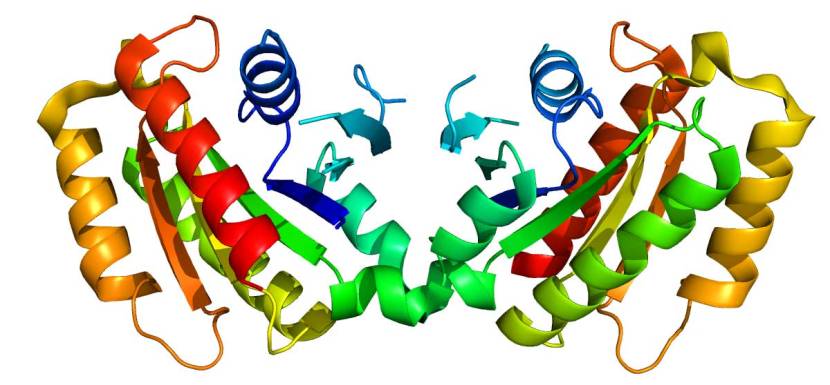
The structure of LRRK2 protein. Source: Wikipedia
As a protein, LRRK2 interacts with many different types of other proteins, and you can imagine that in a finely balanced environment like the cells that a mutant ‘hyperactive’ form of LRRK2 is going to cause problems. The consequences of this constantly active form of LRRK2 protein is believed to be the cause of cell death in LRRK2-associated Parkinson’s.
So how are Denali trying to stop this hyperactive form of LRRK2?
They are developing drugs called LRRK2 inhibitors. These are compounds that bind to the protein and prevent it was doing its job.
Their first drug, DNL-201, is a selective, orally-available, brain-penetrant, reversible small molecule LRRK2 inhibitor.
Do we know if DNL-201 works in models of Parkinson’s?
Yes. There have been two peer-reviewed publications involving the GNE-7915 inhibitor (which I am assuming is DNL-201).
First, in February of 2017:
 Title: Effects of LRRK2 Inhibitors on Nigrostriatal Dopaminergic Neurotransmission.
Title: Effects of LRRK2 Inhibitors on Nigrostriatal Dopaminergic Neurotransmission.
Authors: Qin Q, Zhi LT, Li XT, Yue ZY, Li GZ, Zhang H.
Journal: CNS Neurosci Ther. 2017 Feb;23(2):162-173.
PMID: 27943591 (This article is OPEN ACCESS if you would like to read it)
In this study, the researchers wanted to evaluate the effects of three types of LRRK2 inhibitors (LRRK2-IN-1, GSK2578215A, and GNE-7915) on dopamine release in the brains of mice. They found that LRRK2-IN-1 decreased levels of dopamine release, while GSK2578215A and GNE-7915 did not. They next assessed the effects of the inhibitors in two mouse models of LRRK2-associated Parkinson’s (genetically engineered mice; one group contained the human LRRK2 gene with the G2019S mutation, and the other group had the human LRRK2 gene with the R1441G variant). In both mouse models, GNE-7915 was found to enhances dopamine release and improve cell function, while GSK2578215A had no effect. Thus the investigators concluded the GNE-7915 should be “validated for further therapeutic development for PD”.
And this was done in a study that was published in November 2017:
 Title: LRRK2 G2019S-induced mitochondrial DNA damage is LRRK2 kinase dependent and inhibition restores mtDNA integrity in Parkinson’s disease.
Title: LRRK2 G2019S-induced mitochondrial DNA damage is LRRK2 kinase dependent and inhibition restores mtDNA integrity in Parkinson’s disease.
Authors: Howlett EH, Jensen N, Belmonte F, Zafar F, Hu X, Kluss J, Schüle B, Kaufman BA, Greenamyre JT, Sanders LH.
Journal: Hum Mol Genet. 2017 Nov 15;26(22):4340-4351.
PMID: 28973664
In this study, the researchers wanted to assess the impact of the LRRK2 G2019S mutation has on mitochondrial DNA. You may recall from previous posts that mitochondria are small bean-shaped structures that act as the power stations of each cell. They help to keep the lights on. Without them, the party is over and the cell dies.

Mitochondria and their location in the cell. Source: NCBI
A curious feature of these little structures is that they have their own DNA – separate from the DNA in the nucleus of the cell within which they live. Damage to mitochondrial DNA can cause the mitochondria to die, and as they die so too does the cell.
The researchers found that by producing high levels of LRRK2 G2019S mutant protein, they caused increased levels of damage to mitochondrial DNA. Interestingly, they only saw this effect in dopamine neurons, and not neurons from other regions of the brain such as the cortex. By introducing high levels of normal LRRK2 protein, the investigators could not rescue the mitochondrial DNA damage.
Amazingly, treatment of the dopamine cells producing high levels of LRRK2 G2019S mutant protein with the LRRK2 inhibitor GNE-7915, either prevented or restored mitochondrial DNA damage back to normal levels. These investigators concluded by suggesting that “blocking or reversing mitochondrial DNA damage via LRRK2 inhibition or other therapeutic approaches may be useful to slow PD-associated pathology”.
And it should also be noted that none of the researchers involved in these two studies were associated with Denali Therapeutics (to my knowledge).
OK, so what is the new Denali Phase Ib study all about?
In April 2017, Denali filed an investigational new drug application (or IND) with the FDA for the testing of DNL-201 in humans. They then initiated a three-part Phase I clinical trial of the drug in 122 healthy volunteers in the United States in June 2017. That Phase I study was completed in late 2017, and the results of that study were announced in August of this year (Click here to read the press release). The results suggested that the drug is safe and the company began planning for further clinical evaluation of this new treatment.
In October of this year, Centogene and Denali Therapeutics announced a strategic collaboration in order to help with recruiting individuals with LRRK2 genetic variants for the coming clinical trials (Click here to read more about this)

This week, Denali Therapeutics announced the initiation of the next step in their clinical testing of DNL-201, with the first participant in the Phase Ib study being dosed (Click here to read the press release).
This study is a 28-day, randomized, placebo controlled Phase 1b clinical trial in people with mild to moderate Parkinson’s, with and without genetic LRRK2 mutations (Click here to read more about the details of the study). The purpose of the study is to evaluate safety, tolerability, pharmacokinetics (the effect of body on the drug) and pharmacodynamics (the effect of drug on the body) of DNL-201. In addition, the researchers will be evaluating target and pathway engagement – using different biomarkers – following multiple oral doses of DNL201 (or placebo). There will also be an assessment of certain clinical endpoints.
The 30 participants enrolled in the study will be randomized to receive either a low dose of DNL201, a high dose of DNL201, or placebo. Both the participants and investigators will be blind to who is receiving which treatment, and the results of the study should be available before the end of 2019.
Why are they testing people with and without LRRK2 genetic mutations?
I am not sure, but it could have something to do with a research report published earlier this year:
 Title: LRRK2 activation in idiopathic Parkinson’s disease
Title: LRRK2 activation in idiopathic Parkinson’s disease
Authors: Di Maio R, Hoffman EK, Rocha EM, Keeney MT, Sanders LH, De Miranda BR, Zharikov A, Van Laar A, Stepan AF, Lanz TA, Kofler JK, Burton EA, Alessi DR, Hastings TG, Greenamyre JT
Journal: Science Translational Medicine 25 Jul 2018: 10 (451), eaar5429.
PMID: 30045977
In this study, the investigators looked at LRRK2 activity on sections of postmortem brain from 7 individuals who had passed away with idiopathic (or spontaneous) Parkinson’s and compared them with section of brain from 8 healthy controls. Idiopathic Parkinson’s is any form of Parkinson’s that can not be immediately associated with a particular causal factor. Most forms of Parkinson’s are idiopathic, while individuals with Parkinson’s that results from genetic mutations are considered non-idiopathic.
The researchers used sections of brain from an area called the midbrain, which contains a region called the substantia nigra – the area of the brain where the dopamine-producing cells reside. These cells are particularly affected in Parkinson’s, with approximately 50% of them being lost by the time of diagnosis.
 The dark pigmented dopamine neurons in the substantia nigra are reduced in the Parkinson’s brain (right). Source:Memorangapp
The dark pigmented dopamine neurons in the substantia nigra are reduced in the Parkinson’s brain (right). Source:Memorangapp
To the surprise of the researchers the remaining dopamine neurons of the cases of idiopathic Parkinson’s showed about a 4-6 fold increase in markers of LRRK2 activity (compared with the control brains). This finding suggested to the researchers that normal LRRK2 protein becomes highly activated in Parkinson’s.
 Control brains (top) have low levels of LRRK2 activity (shown in red and gray in the center and right panels), while Parkinson’s brains (bottom) have high levels. The far left panels show dopamine neurons in blue. Source: STAT
Control brains (top) have low levels of LRRK2 activity (shown in red and gray in the center and right panels), while Parkinson’s brains (bottom) have high levels. The far left panels show dopamine neurons in blue. Source: STAT
Interestingly, this increase in LRRK2 levels was not isolated to neurons in the idiopathic Parkinson’s brain. Microglia – the resident immune cells in the brain – also exhibited twice the normal levels of LRRK2 activity.
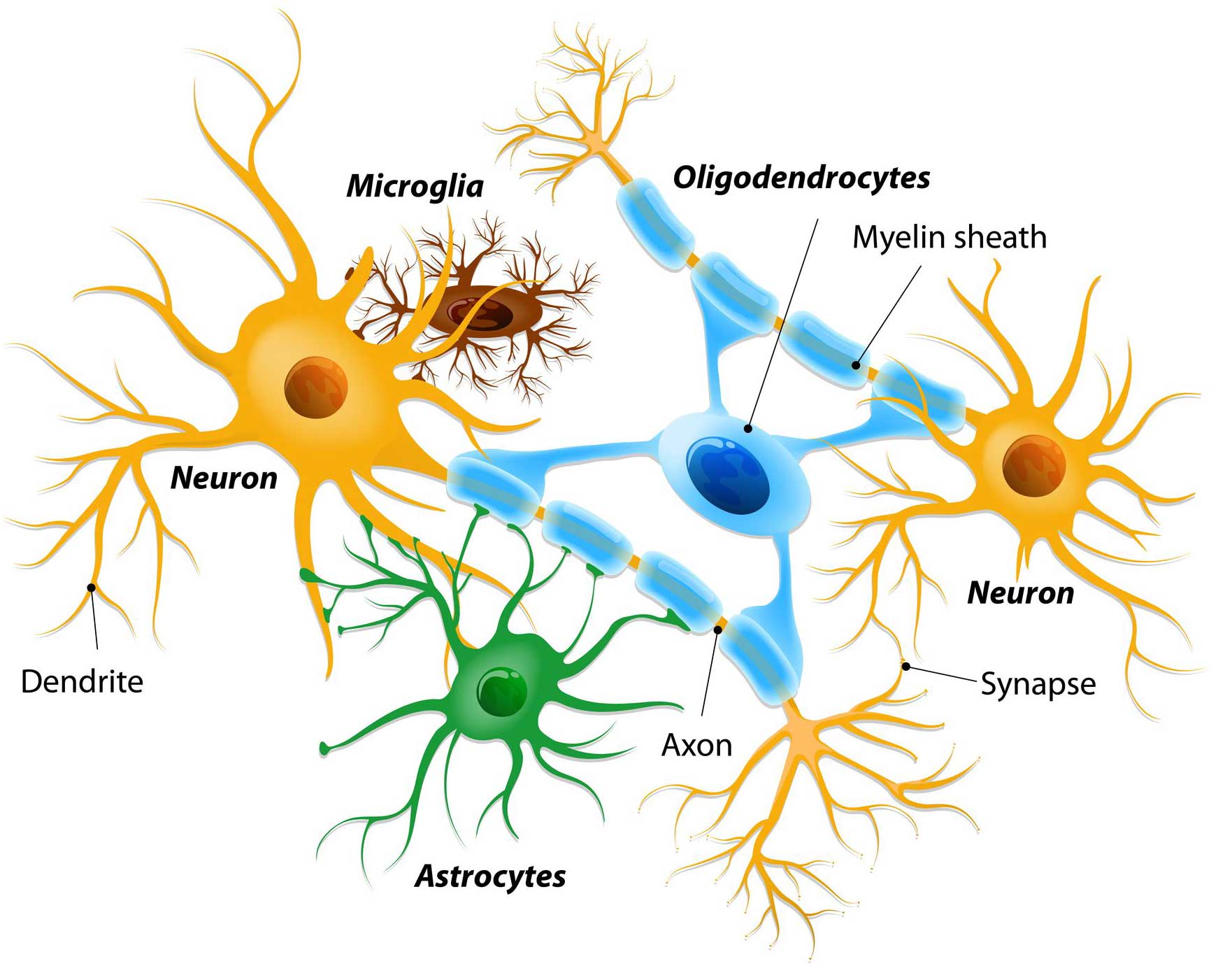 Different types of cells in the brain. Source: Dreamstime
Different types of cells in the brain. Source: Dreamstime
Next, the investigators looked at what happens to LRRK2 activity levels in an animal model of Parkinson’s – specifically, a model that involves a pesticide toxin (called Rotenone – Click here to read a previous SoPD post on pesticides). When they looked at dopamine neurons in animals treated with rotenone, the researchers observed a 10-fold increase in certain markers of LRRK2 activity. They also reported disruption of cellular waste disposal (or autophagy) markers caused by rotenone treatment.
The researchers then looked at a second animal model of Parkinson’s – this one involving very high levels of normal human alpha synuclein protein (caused by injection of carefully genetically engineered viruses), and again, the researchers observed a 10-fold increase in certain markers of LRRK2 activity.
In a third test, the researchers caused oxidative stress on cells and observed an increase in LRRK2 activity, which could be reduced by treatment with anti-oxidants.
All of these results collectively suggest that the role of LRRK2 in Parkinson’s is potentially a lot greater than we previously thought. By using many of the factors associated with the development of Parkinson’s – such as exposure to pesticides, aggregated alpha synuclein protein, and oxidative stress – the researchers observed increased levels of LRRK2 activity.
Thus, it may be that Denali are interested in determining if their LRRK2 inhibitor (DNL-201) can work in people with Parkinson’s with and without genetic LRRK2 mutations.
It kind of goes without saying, but it would be great if it works in both groups!
Indeed. Ok, so what does it all mean?
No, we’re not summing up just yet.
You see, Denali have another drug in clinical development that could be very interesting to test in Parkinson’s.
In March of this year, Denali announced the initiation of a clinical study evaluating the RIPK1 inhibitor (Click here to read the press release).
What is RIPK1?
Receptor‐interacting protein kinase‐1 (RIPK1) is an enzyme involved in a variety of cellular pathways related to both cell survival and death (particularly inflammation-based pathways – click here to read more about RIPK1).
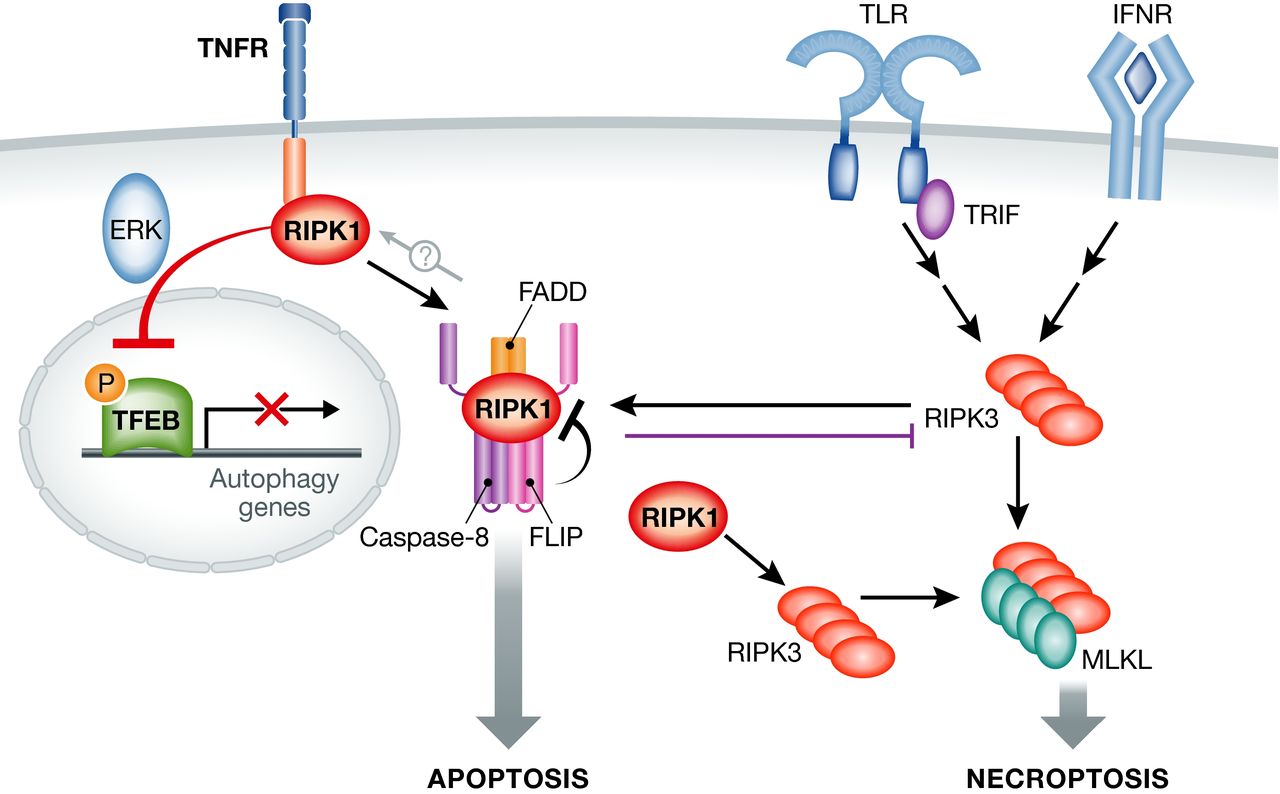 The RIPK1 involvement in two cell death pathways. Source: Embo
The RIPK1 involvement in two cell death pathways. Source: Embo
In March of this year, Denali initated a Phase I clinical trial of their RIPK1 inhibitor (DNL747) in the Netherlands (Click here to read more about the details of that study). In October, the company announced a broad collaboration for the RIPK1 inhibitor programme with the Pharma company Sanofi (Click here to read the press release).
![]() And then in November, Denali announced positive results from the Phase I study which indicated engagement and inhibition of RIPK1, at doses that were both safe and well tolerated (Click here to read more about this).
And then in November, Denali announced positive results from the Phase I study which indicated engagement and inhibition of RIPK1, at doses that were both safe and well tolerated (Click here to read more about this).
In November, the company intiated Phase Ib clinical trials to evaluate DNL747 in people with Alzheimer’s (Click here to read more about this trial) and in people with amyotrophic lateral sclerosis (ALS or motor neurone disease – Click here to read more about this trial). In their previous press release, Denali also suggest that they are exploring the idea of testing DNL747 in multiple sclerosis, but they do not mention Parkinson’s (Click here to read the press release).
The argument for RIPK1 inhibition in Alzheimer’s and ALS is strong (Click here and here to read examples of research supporting this idea), but very little is known about RIPK1 is Parkinson’s.
So why would DNL747 be interesting for Parkinson’s?
DNL747 is based on a highly specific and brain-penatrant inhibitor of RIPK1 called Necrostatin-1 (Nec-1s, R-7-Cl-O-Nec-1). And while little known about RIPK1 in Parkinson’s, there have been several reports suggesting that Necrostatin-1 has some interesting properties in models of Parkinson’s (Click here, here and here to read some examples).
Most of the PD models tested thus far have been based on neurotoxins, which may not be considered very disease-appropriate, but RIPK1 has also been reported to interact with interact with Parkinson’s-associated proteins such as PARKIN and LRRK2 (Click here and here for examples of this).
It would be interesting to see more RIPK1 research in the context of Parkinson’s.
So what does it all mean?
This week we learned that a new clinical trial was initiated by the biotech firm Denali. The study represents an exciting new step in the development of a novel class of drugs for Parkinson’s: LRRK2 inhibitors
This new trial will test the safety and tolerablity of the drug in people with Parkinson’s (with and without LRRK2 genetic mutations). The study will not be long enough to determine if the drug is working (slowing the progression of Parkinson’s), but it will tell us if it is safe and functioning (reducing levels of LRRK2) in the target population.
And if this treatment is successful in Parkinson’s, there could be the potential for its use in other conditions. For example, LRRK2 inhibition has been shown to reduce secondary brain injury caused in models of stroke (Click here to read an example of this). Increased levels of LRRK2 following brain injury appear to be associated with more damage, while inhibition of LRRK2 reduces the amount of damage. Thus, there could be secondary markets for LRRK2 inhibitors as therapies for other forms of brain damage.
One question that still remains unaddressed within the field of LRRK2 inhibitors is what (if any) effect these drugs (like DNL-201) have on LRRK2’s sibling LRRK1 (which we discussed in a previous post – Click here to read that post). It would be interesting (and indeed ultimately necessary) to address this matter to determine if DNL-201 is affecting LRRK1. Given the level of interet in this field, however, I am sure that researchers are addressing this issue, and we look forward to seeing the fruits of their labour.
EDITOR’S NOTE: Denali Therapeutics and Sanofi are publicly traded companies. That said, the material presented on this page should under no circumstances be considered financial advice. Any actions taken by the reader based on reading this material is the sole responsibility of the reader. Denali Therapeutics and Sanofi have not requested that this material be produced, nor has the author had any contact with the companies or any associated parties. This post has been produced for educational purposes only.
The banner for today’s post was sourced from Denali

Simon, Thank you for sharing more good news! You mention “This new trial will test the safety and tolerablity of the drug in people with Parkinson’s (with and without LRRK2 genetic mutations). The study will not be long enough to determine if the drug is working (slowing the progression of Parkinson’s), but it will tell us if it is safe and functioning (reducing levels of LRRK2) in the target population.” Based on your review of the studies to date, would one assume that benefit could be derived from taking the drug for one month?
LikeLike