|
# # # # It has been reported by multiple independent research groups that tetracycline-based antibiotic drugs (such as doxycycline) have exhibited neuroprotective properties in models of Parkinson’s. Translation of these preclinical findings into the clinic has, however, been difficult. In addition, concerns have been expressed that long-term use of such agents could bring forward the emergence of antibiotic resistance in the bacteria that they are used to control. Recently, researchers have investigated a different type of tetracycline-based molecule that has reduced antibiotic activity, crosses the blood-brain-barrier, and is pharmacologically safe. It is called chemically modified tetracycline 3 (or CMT-3). In today’s post, we will look at the research that has been done on tetracycline-based antibiotic drugs, discuss why we should not be testing antibiotics in Parkinson’s, and consider if CMT-3 could be different. # # # # |

Sir Alexander Fleming. Source: Biography
Sir Alexander Fleming is credited with discovering the antibiotic properties of penicillin.
But – as he himself notes – the discovery was a purely chance event. An accident, if you like.
After returning from a two week holiday, Sir Fleming noticed that many of his culture dishes were contaminated with fungus, because he had not stored them properly before leaving. One mould in particular caught his attention, however, as it was growing on a culture plate with the bacteria staphylococcus. Upon closer examination, Fleming noticed that the contaminating fungus prevented the growth of staphylococci.
In an article that Fleming subsequently published in the British Journal of Experimental Pathology in 1929, he wrote, “The staphylococcus colonies became transparent and were obviously undergoing lysis … the broth in which the mould had been grown at room temperature for one to two weeks had acquired marked inhibitory, bactericidal and bacteriolytic properties to many of the more common pathogenic bacteria.”
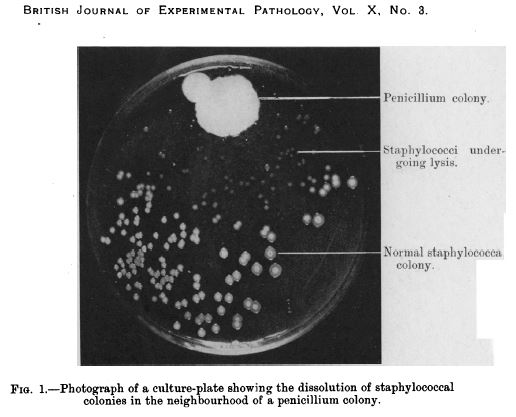
Penicillin in a culture dish of staphylococci. Source: NCBI
Fleming isolated the organism responsible for prohibiting the growth of the staphylococcus, and identified it as being from the penicillium genus.
He named it penicillin and the rest is history (Click here to read that history).
Fleming himself appreciated the serendipity of the finding:
“When I woke up just after dawn on Sept. 28, 1928, I certainly didn’t plan to revolutionise all medicine by discovering the world’s first antibiotic, or bacteria killer” (Source)
And this gave rise to his famous quote:
“One sometimes finds what one is not looking for” (Source)
While Fleming’s discovery of the antibiotic properties of penicillin was made as he was working on a completely different research problem, the important thing to note is that the discovery was made because the evidence came to a prepared mind.
Pasteur knew the importance of a prepared mind. Source: Thequotes
And this is the purpose of all the training in scientific research – not acquiring the keys to some special knowledge, but preparing the investigator to notice the curious deviation.
That’s really interesting, but what does any of this have to do with Parkinson’s?
Eight years ago, a group of Parkinson’s researchers made a serendipitous discovery:
While modelling Parkinson’s in some mice, they noticed that only two of their 40 mice that were given a neurotoxic chemical (6-OHDA) developed the motor features of Parkinson’s, while the rest remained healthy and unaffected. This result left them scratching their heads and trying to determine what had gone wrong.
Then it clicked:
“A lab technician realised the mice had mistakenly been fed chow containing doxycycline, so we decided to investigate the hypothesis that it might have protected the neurons.” (from the press release).
The researchers had noted the ‘curious deviation’ and decided to investigate it further.
They repeated the experiment, but this time they added another group of animals which were given doxycycline in low doses (via injection) and fed on normal food (not containing the doxycycline).
And guess what: both group demonstrated neuroprotection!
Interesting. What is doxycycline?
Doxycycline is an antibiotic that is used in the treatment of a number of types of infections caused by bacteria.
 Doxycycline. Source: Pharmaceutical-technology
Doxycycline. Source: Pharmaceutical-technology
Remind me again, what is an antibiotic?
Antibiotics are a class of drugs that either kill or inhibit the growth of bacteria. They function in one of several ways, either blocking the production of bacterial proteins, inhibiting the replication of bacterial DNA (nuclei acid in the image below), or by rupturing/inhibiting the repair of the bacteria’s outer membrane/wall.
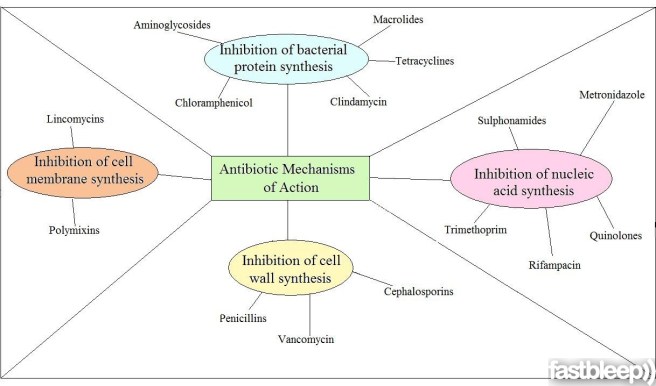
The ways antibiotics function. Source: FastBleep
So the researchers accidentally discovered that the a bacteria-killing drug called doxycycline prevented a neurotoxin from killing dopamine cells?
Basically, yeah.
How does that work?
Following their accidental discovery, the researchers followed up with a series of experiments to investigate and characterise the phenomenon further, and they published the results in this report:
Title: Doxycycline restrains glia and confers neuroprotection in a 6-OHDA Parkinson model.
Authors: Lazzarini M, Martin S, Mitkovski M, Vozari RR, Stühmer W, Bel ED.
Journal: Glia. 2013 Jul;61(7):1084-100. doi: 10.1002/glia.22496. Epub 2013 Apr 17.
PMID: 23595698
In the report of their research, the investigators noted that doxycycline significantly protected the dopamine neurons and their nerve branches (called axons) in the striatum – an area of the brain where dopamine is released – when 6-OHDA was given to mice. Both oral administration and peripheral injections of doxycycline were able to have this effect.
They also reported that doxycycline inhibited the activation of astrocytes and microglial cells in the brains of the 6-OHDA treated mice. Astrocytes and microglial cells are usually the helper cells in the brain, but in the context of disease or injury these cells can quickly take on the role of judge and executioner – no longer supporting the neurons, but encouraging them to die. The researchers found that doxycycline reduced the activity of the astrocytes and microglial cells in this alternative role, allowing the dopamine cells to recuperate and survive.
The researchers concluded that the “neuroprotective effect of doxycycline may be useful in preventing or slowing the progression of Parkinson’s“.
Was this the first time this neuroprotective effect of doxycycline has been observed?
Curiously, No.
We have known of doxycycline’s neuroprotective effects in different models of brain injury since the 1990s (Click here, here and here for more on this). In fact, in their research report, the researchers kindly presented a table of all the previous neuroprotective research involving doxycycline (the table runs for 2 pages).
|
# RECAP #1: An antibiotic called doxycycline was found to have neuroprotective properties in models of Parkinson’s. Similar results have been reported in other models of brain injury and neurodegeneration. # |
Is doxycycline the only antibiotic that exhibits neuroprotective properties?
No.
Doxycycline belongs to a family of antibiotics called ‘tetracyclines‘ (named for their four (“tetra-“) hydrocarbon rings (“-cycl-“) derivation (“-ine”)), and other members of this family have also been shown to display neuroprotection in models of Parkinson’s:
Title: Minocycline prevents nigrostriatal dopaminergic neurodegeneration in the MPTP model ofParkinson’s disease.
Authors: Du Y, Ma Z, Lin S, Dodel RC, Gao F, Bales KR, Triarhou LC, Chernet E, Perry KW, Nelson DL, Luecke S, Phebus LA, Bymaster FP, Paul SM.
Journal: Proc Natl Acad Sci U S A. 2001 Dec 4;98(25):14669-74.
PMID: 11724929 (This article is OPEN ACCESS if you would like to read it)
In this study, the researchers treated mice with an antibiotic called minocycline and it protected dopamine cells from the damaging effects of a toxic chemical called MPTP (or 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine). MPTP is also used in models of Parkinson’s, as it specifically affects the dopamine cells, while leaving other cells unaffected.
The researchers found that the neuroprotective effect of minocycline is associated a reduction in the activity of proteins that initiate cell death (for example, Caspace 1). This left the investigators concluding that ‘tetracyclines may be effective in preventing or slowing the progression of Parkinson’s ‘.
Importantly, this result was quickly followed by two other research papers with very similar results (Click here and here to read more about this). Thus, it would appear that some members of the tetracycline class of antibiotics share some of these neuroprotective properties.
So what did the researchers do next with doxycycline?
They continued to investigate the neuroprotective effect of doxycycline in different models of Parkinson’s. And these lines of research led to this research report:
 Title: Repurposing doxycycline for synucleinopathies: remodelling of α-synuclein oligomers towards non-toxic parallel beta-sheet structured species.
Title: Repurposing doxycycline for synucleinopathies: remodelling of α-synuclein oligomers towards non-toxic parallel beta-sheet structured species.
Authors: González-Lizárraga F, Socías SB, Ávila CL, Torres-Bugeau CM, Barbosa LR, Binolfi A, Sepúlveda-Díaz JE, Del-Bel E, Fernandez CO, Papy-Garcia D, Itri R, Raisman-Vozari R, Chehín RN.
Journal: Sci Rep. 2017 Feb 3;7:41755.
PMID: 28155912 (This article is OPEN ACCESS if you would like to read it)
In this study, the researchers wanted to test doxycycline in a more disease-relevant model of Parkinson’s. 6-OHDA is great for screening and testing neuroprotective drugs. But given that 6-OHDA is not involved with the underlying pathology of Parkinson’s, it does not provide a great measure of how well a drug will do against the disease itself. So, the researchers turned their attention to our old friend, alpha synuclein – the protein which forms the clusters of protein (called Lewy bodies) in the Parkinsonian brain.
What the researchers found was fascinating: Doxycycline was able to inhibit the disease-associated clustering of alpha synuclein.
In fact, by reshaping alpha synuclein into a less toxic version of the protein, doxycycline was able to enhance cell survival. The investigators also conducted a ‘dosing’ experiment to determine the most effect dose and they found that taking doxycycline in sub-antibiotic doses (20–40 mg/day) would be enough to exert neuroprotection. They concluded their study by suggesting that these novel effects of doxycycline could be exploited in Parkinson’s by “repurposing an old safe drug“.
Wow, has doxycycline ever been used in clinical trials for brain-related conditions before?
Yes.
From 2005-12,there was a 7 month clinical study to determine the safety and efficacy of doxycycline (in combination with Interferon-Beta-1a) in treating Multiple Sclerosis (Click here for more on this trial). The results of that study suggested that the combination of intramuscular Interferon Beta-1a and oral doxycycline treatment was safe and well tolerated, but larger studies were required to better determine efficacy (Click here to read more about this).
More importantly, the other antibiotic to demonstrate neuroprotection in models of Parkinson’s, minocycline (which we mentioned above), has been clinically tested in Parkinson’s.
This is the report of that trial:

Title: A pilot clinical trial of creatine and minocycline in early Parkinson disease: 18-month results.
Authors: NINDS NET-PD Investigators..
Journal: Clin Neuropharmacol. 2008 May-Jun;31(3):141-50.
PMID: 18520981 (This article is OPEN ACCESS if you would like to read it)
This research report was the follow up of a 12 month clinical study (Click here to read more about this). The researchers had taken two hundred participants with Parkinson’s and randomly assigned them into the three groups: creatine (an over-the-counter nutritional supplement), minocycline, and placebo (control). All of the participants were diagnosed less than 5 years before the start of the study. At 12 months, both creatine and minocycline were noted as not interfering with the beneficial effects of symptomatic therapy (such as L-dopa), but a worrying trend began with subjects dropping out of the minocycline arm of the study.
At the 18 month time point, approximately 61% creatine-treated subjects had begun to take additional treatments (such as L-dopa) for their symptoms, compared with 62% of the minocycline-treated subjects and 60% placebo-treated subjects. This result suggested that there was no beneficial effect from using either creatine or minocycline in the treatment of Parkinson’s, as neither exhibited any greater effect than the placebo.
In addition, the investigators suggested that the decreased tolerability of minocycline was a concern.
|
# # RECAP #2: In addition to improving neurotoxic models of Parkinson’s, doxycycline has also been reported to reduce the impact of Parkinson’s associated alpha synuclein clustering. A clinical trial of minocycline – similar to doxycycline – failed to demonstrate any beneficial effect in people with Parkinson’s, and it was associated with a higher drop-out rate. # # |
But that was minocycline, perhaps doxycycline is different. Where do I sign up for the next doxy clinical trial?
Well, theoretically speaking, there shouldn’t be a doxycycline trial.
Huh?!?
There’s a good reason why not.
In fact, if you look at the comments section under the González-Lizárraga et al (2017) research article, a cautionary message has been left by Prof Paul M. Tulkens of the Louvain Drug Research Institute in Belgium. He points out that:
“…using antibiotics at sub-therapeutic doses is the best way to trigger the emergence of resistance (supported by many in vitro and in vivo studies). Using an antibiotic for other indications than an infection caused by a susceptible bacteria is something that should be discouraged”
And he is correct.
We recklessly over use antibiotics all over the world at the moment and they are one of the only lines of defence that we have against the bacterial world. Long-term use (which Parkinson’s would probably require) of an antibiotic at sub-therapeutic levels will only encourage the rise of antibiotic resistant bacteria (possibly within individuals).
The resistance of bacteria to antibiotics can occur spontaneously via several means (for example, through random genetic mutations during cell division). With the right mutation (inferring antibiotic resistance), an individual bacteria would then have a natural advantage over their friends and it would survive our attempts to kill it with antibiotics. Being resistant to antibiotic would leave that bacteria to wreak havoc upon us.
Its the purest form of natural selection.

How bacteria become resistant to antibiotics. Source: Reactgroup
And antibiotic-resistant bacteria are fast becoming a major health issue for us, with the number of species of bacteria developing resistance increasing every year (Click here for a good review on factors contributing to the emergence of resistance, and click here for a review of the antibiotic resistant bacteria ‘crisis’).
But please don’t be upset on the Parkinson’s side of things. Prof Tulken adds that:
“If doxycycline really acts as the authors propose, the molecular targets are probably very different from those causing antibacterial activity. it should therefore be possible to dissociate these effect from the antibacterial effects and to get active compounds devoid of antibacterial activity This is where research must go to rather than in trying to use doxycycline itself.”
And he is correct again.
Rather than tempting disaster, we need to take the more prudent approach.
If researchers can isolate the neuroprotective elements of doxycycline and those same parts are separate from the antibiotic properties, then we may be able to generate novel experimental drugs for treating Parkinson’s.
And the good news is that researchers are already reasonably sure that the mechanisms of the neuroprotective effect of doxycycline are distinct from its antimicrobial action.
|
# # # RECAP #3: One problem with testing antibiotics like doxycycline in Parkinson’s is that it could encourage the rise of antibiotic-resistant bacteria (even at low doses). These treatments are one of the few lines of defense that we have against the bacterial world. We have to be careful in how we apply them. # # # |
So yet again we’re waiting for researchers to generate more “novel therapies” for Parkinson’s?
Well, we might not need to wait too long.
Que???
This week, a study was published that investigated an engineered version of doxycycline that possesses reduced antibiotic properties.
This is the report here:
 Title: CMT-3 targets different α-synuclein aggregates mitigating their toxic and inflammogenic effects.
Title: CMT-3 targets different α-synuclein aggregates mitigating their toxic and inflammogenic effects.
Authors: González-Lizárraga F, Ploper D, Ávila CL, Socías SB, Dos-Santos-Pereira M, Machín B, Del-Bel E, Michel PP, Pietrasanta LI, Raisman-Vozari R, Chehín R.
Journal: Sci Rep. 2020 Nov 20;10(1):20258.
PMID: 33219264 (This report is OPEN ACCESS if you would like to read it)
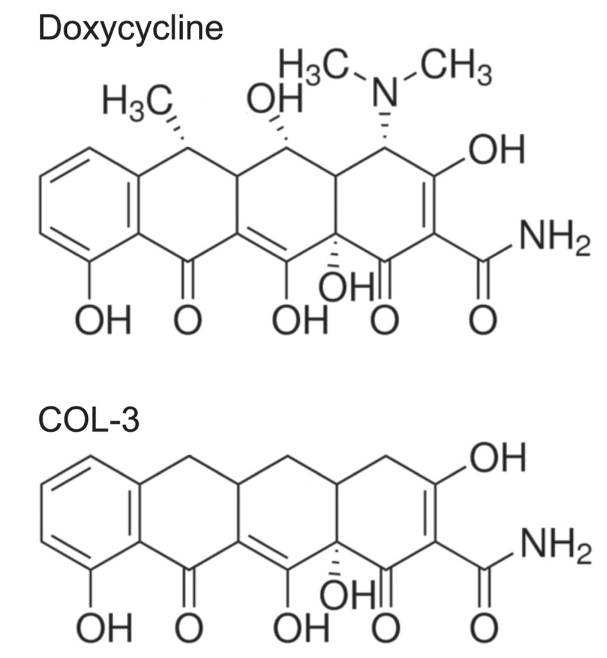
In this study, the researchers tested chemically modified tetracycline 3 (or CMT-3) – a derivative of doxycycline with reduced antibiotic activity – in models of Parkinson’s.
What is CMT-3?
CMT-3 (also known as COL-3, Incyclinide, and Metastat) was identified in experiments seeking to develop derivatives of doxycycline.
If you look at the structure of the molecules in the image below, you will notice that CMT-3 (labelled as COL-3) doesn’t have all of the “bits and bobs” attached to the top side of doxycycline. These bits and bobs are where the interaction with the bacterial ribosome occurs, resulting in the antibacterial effect. As CMT-3/COL-3 does not have them, there is reduced antibacterial activity.
 Source: Semanticscholar
Source: Semanticscholar
Is it just me, or from this angle does CMT-3 looks a bit like a weird little catapillar?
Quite a lot of research has been conducted on CMT-3, including several clinical trials which indicated that it was safe and well tolerated in humans. And a Phase I brain tumor study suggested that it can cross the blood brain barrier – the protective membrane surrounding the brain (Click here to read the results of that study).
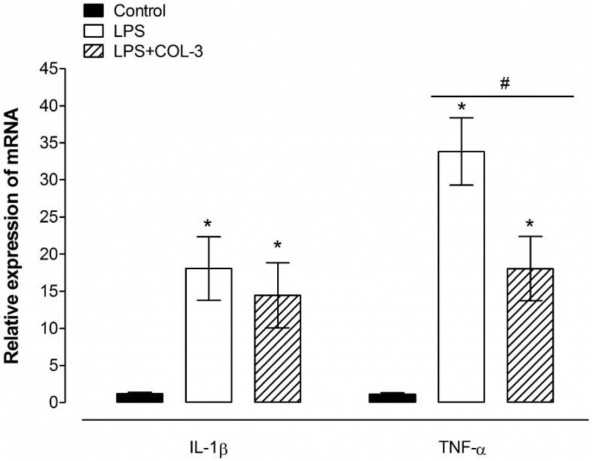
In addition to crossing the blood-brain barrier, CMT-3 also has good anti-inflammatory properties (dampening down the immune system when it gets excited about something). For example, this report found that CMT-3 inhibits the activation of microglia (microglia are the resident immune cells in the brain):
 Title: COL-3, a chemically modified tetracycline, inhibits lipopolysaccharide-induced microglia activation and cytokine expression in the brain.
Title: COL-3, a chemically modified tetracycline, inhibits lipopolysaccharide-induced microglia activation and cytokine expression in the brain.
Authors: Edan RA, Luqmani YA, Masocha W.
Journal: PLoS One. 2013;8(2):e57827.
PMID: 23469077 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers reported that COL-3 (CMT-3) inhibited microglial activation (brought on by lipopolysaccharide (LPS) treatment) and reduced levels of TNF-α (a messenger protein involved with encouraging inflammation in the body).
 The investigators also reported that COL-3 had limited and very selective anti-bacterial activity.
The investigators also reported that COL-3 had limited and very selective anti-bacterial activity.
Ok, so what did the recent study in models of Parkinson’s find? Did CMT-3 work as well as doxycycline?
It did.
The researchers reported that CMT-3 was as potent as doxycycline in its ability to inhibit the aggregation of alpha synuclein. Treatment with CMT-3 also led to the formation of non-toxic species of alpha synuclein (Click here to read a previous SoPD post about alpha synuclein species).
Interestingly, the researchers also tested minocycline and found that it completely failed to inhibit the aggregation of α-synuclein. Could this be why the clinical trial of minocycline clinical trial in Parkinson’s failed to show any positive outcome?
Interesting, what else did the researchers find?
Next they wanted to study the effect of CMT-3 on disassembling mature aggregates of alpha synuclein. The researchers compared CMT-3 with doxycycline, and curiously while they found that CMT-3 could disassemble preformed alpha synuclein aggregates, doxycycline could not do this.
And again, the results of this experiment indicated that CMT-3 could disassemble mature alpha synuclein aggregates into smaller fragments that were unable to seed any further aggregation. In addition, these disaggregated fragments were non-toxic and less inflammatory on microglial cells than other species of alpha synuclein.
Further analysis suggested that CMT-3 is binding to alpha synuclein protein via a mechanism similar to that proposed for EGCG (Click here to read an old SoPD post about EGCG).
The researchers concluded their study by writing “considering its very low antimicrobial activity and the concentration required for its neuroprotective action, long-term therapy with CMT-3 should not negatively affect human native microbiota. Nevertheless, more experimental evidence is required to support this hypothesis“.
Wow. Where can I get me some CMT-3?
This data needs to be independently replicated and expanded on before we start planning a clinical trial.
The researchers also stated in the discussion of their report: “Whether CMT-3 administration is able to prevent alpha-synuclein deposition into Lewy bodies or even disassemble α-synuclein fibrils in vivo, either in α-synuclein overexpressing PD mice models or in animals injected with alpha synuclein fibrils is unknown“. They also suggest that it would be interesting to evaluate CMT-3 on alpha synuclein protein that harbors mutations that are predisposed to increased risk of Parkinson’s (such as the A53T mutation).
It should also be noted that CMT-3 does not come without some cautionary issues.
In a 2001 clinical trial, three of 35 participants developed drug-induced lupus (an autoimmune condition – click here to read more about this trial). But CMT-3 is not the only doxycycline-based derivative to be implicated with this (minocycline induced autoimmune syndromes were described four of 82 patients, all occurring in young patients treated for acne – click here to read more about this).
So what does it all mean?
Tetracycline-based antibiotics (such as doxycycline) have been found to have neuroprotective properties in models of Parkinson’s, but long-term use of such medication is not feasible as it risks the rise of resistance in the very bacteria that these drugs are designed to protect us from.
Recently researchers have been investigating an engineered tetracycline-based molecule called “chemically modified tetracycline 3” (or CMT-3) in models of Parkinson’s. It has reduced antibiotic properties, accesses the brain, and possesses anti-inflammatory effects. In addition, new results suggest that CMT-3 can also inhibit the aggregation of alpha synuclein and disassemble mature alpha synuclein aggregates into smaller non-toxic fragments.
Further research is required on this molecule in the context of Parkinson’s, and if those results are supportive, CMT-3 might offer a more agreeable approach to clinically test on Parkinson’s than some of the other tetracycline-based antibiotics, like doxycycline.
We look forward to more research in this area.
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
EDITOR’S NOTE: Under absolutely no circumstances should anyone reading this material consider it medical advice. The material provided here is for educational purposes only. Before considering or attempting any change in your treatment regime, PLEASE consult with your doctor or neurologist. While some of the drugs discussed on this website are clinically available, they may have serious side effects. We therefore urge caution and professional consultation before any attempt to alter a treatment regime. SoPD can not be held responsible for any actions taken based on the information provided here.
The banner for today’s post was sourced from echelon.

Curiously I have always thought of doxy as an antimalarial. It had the advantage that you did not need to take it for 6 weeks after you left a malarial area, though had to be taken with food or it came up again “rapidly”. I wonder if the anti PD mechanism has anything in common with the several other antimalarials which have also shown promise such as quinine related drugs?
LikeLike
I was living overseas when I was diagnosed with PD and had been on doxy, as an anti-malarial and with non of the side-effects that some have, for 4 years by then. After Simon’s original post on doxy, and reaching out to the researchers, I decided I would carry on with it (I’ve been back in the UK 3 yrs). All I can say is my PD is very slow progressing.
LikeLike
Hi Rosie! I hope you are still able to receive messages on this thread! What is the dose of Doxy that you take each day? My eye doctor suggested that I take a low-dose of doxy daily for my dry eye disease/MGD. I’m debating whether it’s something I wanna move forward with and so in researching it, I discovered that there might be a positive effect of the Doxy on my Parkinson’s. Any information you can share is appreciated!
LikeLike
Hi Tracy,
I was on 100mg daily, as that was my prescription for taking doxy as an antimalarial, and also what was easily available. However, I stopped taking doxy about two years ago. Various reasons: ongoing issue of antibiotic resistance; realisation that long term antibiotics are not good for my gut microbiome; my supply line from Uganda had all but dried up (I always knew it would eventually). I was also aware that it seems to be the anti-inflammatory element of the drug that is neuroprotective, rather than the antibiotic element, so I now concentrate on an anti-inflammatory diet. Hope that helps in your search!
LikeLike
hi Rosie! Thank you so much for your response. Did you ever try the sub anti-microbial dose of 40 mg per day? Here is an NIH statement indicating how it works (https://www.ncbi.nlm.nih.gov/books/NBK555888/)
“Anti-inflammation
• Doxycycline hyclate can be taken at sub-acute doses of 40 mg daily for anti-inflammatory effects. The anti-microbial mechanism will not be in action at this sub-antimicrobial dose, sparing healthy bacteria and maintaining the body’s microbiome.”
This is the amount I am considering taking and this is the amount that has shown promise in some research used with Parkinson’s patients.
Hope you are doing well and that your progression is still slow!
LikeLike
Thanks for the info, Tracy, I’ll look into it.
LikeLike