|
This week a group of scientists have published an article which indicates differences between mice and human beings, calling into question the use of these mice in Parkinson’s disease research. The results could explain way mice do not get Parkinson’s disease, and they may also partly explain why humans do. In today’s post we will outline the new research, discuss the results, and look at whether Levodopa treatment may (or may not) be a problem. |

The humble lab mouse. Source: PBS
Much of our understanding of modern biology is derived from the “lower organisms”.
From yeast to snails (there is a post coming shortly on a snail model of Parkinson’s disease – I kid you not) and from flies to mice, a great deal of what we know about basic biology comes from experimentation on these creatures. So much in fact that many of our current ideas about neurodegenerative diseases result from modelling those conditions in these creatures.
Now say what you like about the ethics and morality of this approach, these organisms have been useful until now. And I say ‘until now’ because an interesting research report was released this week which may call into question much of the knowledge we have from the modelling of Parkinson’s disease is these creatures.
You see, here’s the thing: Flies don’t naturally develop Parkinson’s disease.
Nor do mice. Or snails.
Or yeast for that matter.
So we are forcing a very un-natural state upon the biology of these creatures and then studying the response/effect. Which could be giving us strange results that don’t necessarily apply to human beings. And this may explain our long history of failed clinical trials.
We work with the best tools we have, but it those tools are flawed…
What did the new research report find?
This is the study:
Title: Dopamine oxidation mediates mitochondrial and lysosomal dysfunction in Parkinson’s disease
Authors: Burbulla LF, Song P, Mazzulli JR, Zampese E, Wong YC, Jeon S, Santos DP, Blanz J, Obermaier CD, Strojny C, Savas JN, Kiskinis E, Zhuang X, Krüger R, Surmeier DJ, Krainc D
Journal: Science, 07 Sept 2017 – Early online publication
PMID: 28882997
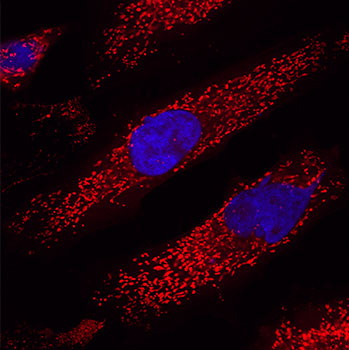
The researchers who conducted this study began by growing dopamine neurons – a type of cell badly affected by Parkinson’s disease – from induced pluripotent stem (IPS) cells.
What are induced pluripotent stem cells?