|
Many novel therapies are currently being clinically tested in Parkinson’s, and this week we heard the results of one clinical trial which provided some very interesting news. Intra-Cellular Therapies has been testing their drug, ITI-214 – which is a potent and selective phosphodiesterase 1 (PDE1) inhibitor. Inhibitors of PDE1 prevent the breakdown of protein called cyclic nucleotides (cAMP, cGMP). The results of the Intra-Cellular Therapies clinical trial suggest that in people with Parkinson’s, the drug not only improves symptoms, but also reduces dyskinesias. In today’s post we will discuss what PDE1 is, how PDE1 inhibitors work, and what the results of the clinical trial suggest.
|
Source: 2018.myana
Every year in October, the American Neurology Association (ANA) gather in one of the major US cities to share research regarding neurological condtions, like Parkinson’s. And while I did not attend the ANA meeting this year, I was keen to hear the results of one particular clinical study.
It was a trial conducted by a company called Intra-Cellular Therapies.
 And they were presenting the results of a Phase I/II trial of their experimental drug ITI-214.
And they were presenting the results of a Phase I/II trial of their experimental drug ITI-214.
What is special about ITI-214?
ITI-214 is a Phosphodiesterase inhibitor.
What is a phosphodiesterase inhibitor?
Phosphodiesterase inhibitors – as the label on the can suggests – inhibit Phosphodiesterases.
And, pray tell, what are Phosphodiesterases?
Phosphodiesterases are a diverse family of enzymes (there are 11 different types of Phosphodiesterases in humans) that are present inside every cell in your body. They play key roles in regulating levels of cAMP and cGMP.
And yes, I know what you are going to ask next:
Cyclic Adenosine MonoPhosphate (cAMP) and Cyclic Guanosine MonoPhosphate (cGMP) are what we call second messengers within a cell.
We have previously talked about the idea of receptors on the surface of cells (Click here to read a post on this). They function act like a ‘light switch’ – allowing for certain biological processes to be initiated or inhibited. All that a receptor requires to be activated (or blocked) is a chemical messenger – called a ligand – to come along and bind to it.
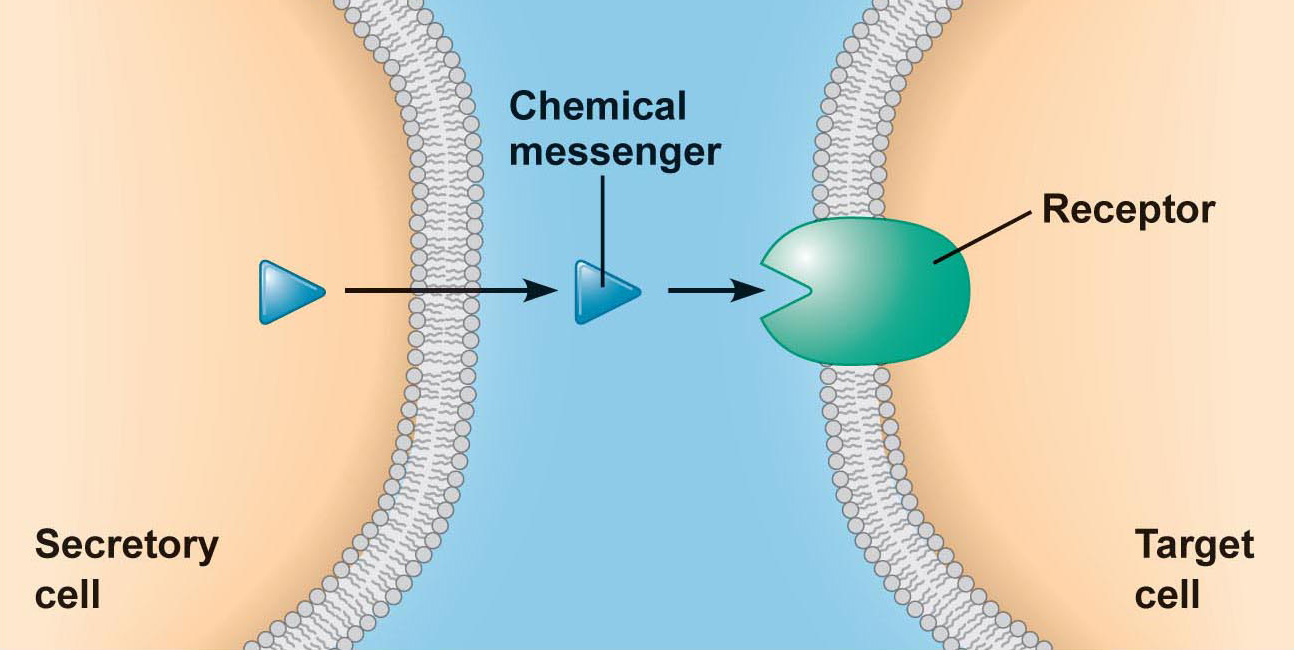 An example of a receptor on a cell. Source: Droualb
An example of a receptor on a cell. Source: Droualb
The ligand is considered a first messenger in the process of cellular signalling.
But what happens next?
After the receptor is activated, what actually happens inside the cell?
Well, this is where second messengers, like cAMP and cGMP come into the picture. cAMP and cGMP are the molecules that make stuff happen after a receptor is activated.
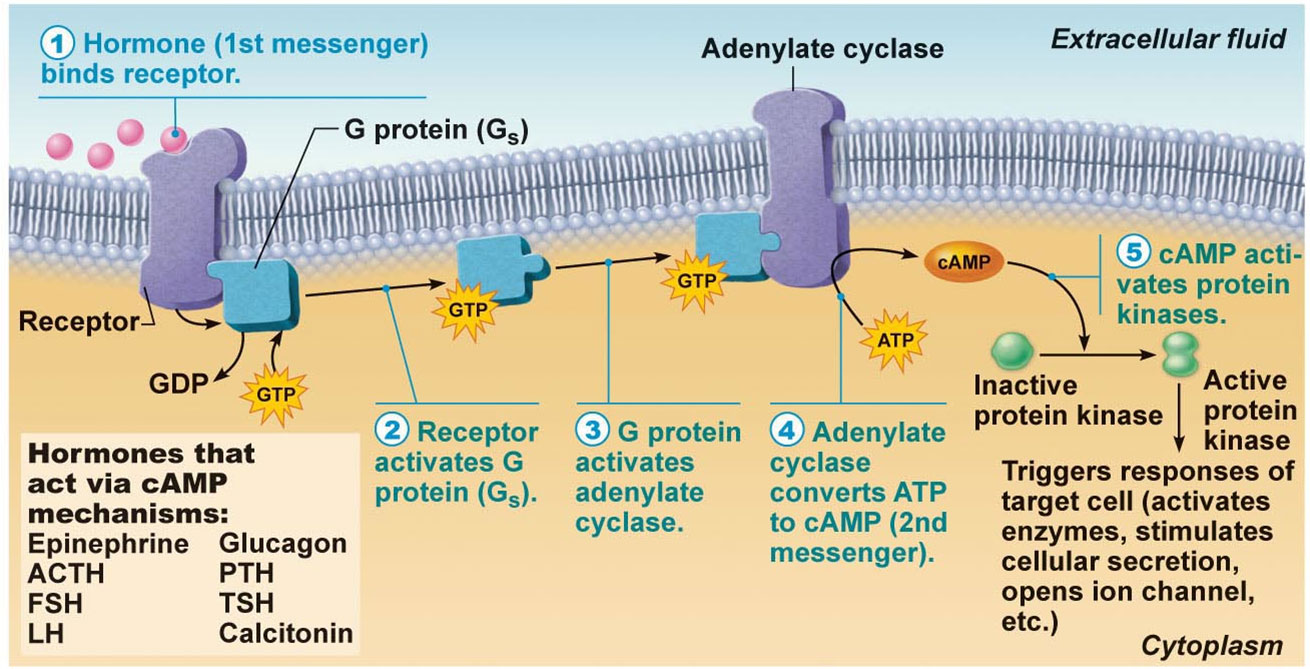
Source: Picmia
Second messengers, like cAMP and cGMP stimulate different biological pathways (based on which receptor has been activated). These pathways are control all sorts of cellular processes. For example, cAMP is known to reduce inflammation, reduce blood pressure, and be neuroprotective – in addition to a host of other properties:
 Some of the effects of cAMP activity. Source: Nutritionreview
Some of the effects of cAMP activity. Source: Nutritionreview
So how do Phosphodiesterases regulate levels of cAMP and cGMP?
As I mentioned above these Phosphodiesterase enzymes are involved in controlling levels of cAMP and cGMP. They do this by enzymatically breaking down one of the bonds (a phosphodiester bond) holding these messengers together.By breaking down this bond, cAMP and cGMP are rendered non-functional (potentially resulting in more inflammation and less neuroprotection).
 Binding of PDE to cGMP and cAMP. Source: Wikipedia
Binding of PDE to cGMP and cAMP. Source: Wikipedia
So, high levels of Phosphodiesterase = lower levels of cAMP and cGMP. And by blocking Phosphodiesterases, there is an increase in levels of cAMP and cGMP.
Thus, if you treat someone with a Phosphodiesterase inhibitor, levels of cAMP and cGMP increase, which results in more of that good stuff being able to occur, such as neuroprotection and reduced inflammation.
Sounds interesting. So what did the clinical trial results suggest?
Before we get to that, there is something else I need to explain.
You may recall that there are 11 different types of Phosphodiesterases, and each of them have different functions. Researchers have developed inhibitors (or blockers) for some of these different types of Phosphodiesterases and they are being tested for a variety of different medical conditions.
And one example of this is ITI-214 (the drug I mentioned near the top of this post). ITI-214 is an orally administered phosphodiesterase 1 inhibitor.
What does phosphodiesterase 1 do?
Phosphodiesterase 1 (PDE1) is interesting and unique when compared to the other 10 members of the phosphodiesterase family, because it is regulated by calcium.
When calcium levels go up, PDE1 becomes more activated.
And we have previously spoken at length about the potential role of calcium in Parkinson’s (Click here and here for previous posts on this topic), so there is already an interesting angle here with regards to PD.
In addition to this feature of PDE1, there has been a number of publications suggesting the potential of PDE1 inhibitors in the treatment of Parkinson’s (for an interesting OPEN ACCESS review of PDE1 inhibitors in neurological conditions – click here).
What other research has been conducted?
Well, when we look at the human brain, one of the regions with the highest levels of PDE1 is the striatum (Click here to read more about this). In humans, the striatum is made up of two areas: the caudate nucleus and the putamen. The striatum is where the dopamine producing neurons project their branches to and release dopamine. In Parkinson’s, these branches are severely reduced.

Dopamine neurons (in black) projecting their branches to the striatum. Source: MyBrainNotes
Given this high level of PDE1 in a region involved with Parkinson’s, researchers have been interested to determine what role PDE1 could be playing in this condition.
Has a PDE1 inhibitor ever been tested in model of Parkinson’s?
Yes. This report was published last year:

Title: Protective efficacy of phosphodiesterase-1 inhibition against alpha-synuclein toxicity revealed by compound screening in LUHMES cells.
Authors: Höllerhage M, Moebius C, Melms J, Chiu WH, Goebel JN, Chakroun T, Koeglsperger T, Oertel WH, Rösler TW, Bickle M, Höglinger GU.
Journal: Sci Rep. 2017 Sep 13;7(1):11469.
PMID: 28904388 (This article is OPEN ACCESS if you would like to read it)
In this study, the investigators screened 1,600 FDA-approved drugs for their efficacy to protect dopamine cells grown in cell culture from degeneration which was caused by very high levels of alpha synuclein – the protein that clusters (or aggregates together in Parkinson’s. When the researchers looked at the drugs that prevent degeneration the best, they identified dipyridamole (a non-selective phosphodiesterase inhibitor that is used as a medication for inhibiting blood clot formation) as the top drug.
They next conducted a systematic analysis of other phosphodiesterase inhibitors, in order to try and identify a specific phosphodiesterase inhibitor that could most potently rescue cells from alpha synuclein toxicity.
This was the result:
 Only PDE1 inhibition (Vinpocetine) reduced alpha synuclein toxicity. Source: Nature
Only PDE1 inhibition (Vinpocetine) reduced alpha synuclein toxicity. Source: Nature
A drug called Vinpocetine (a phosphodiesterase 1 inhibitor) was the only phosphodiesterase inhibitor that reduced alpha synuclein toxicity. Vinpocetine is a synthetic alkaloid derived from the periwinkle plant. It is synthesised from a molecule called ‘vincamine‘.
Vinpocetine is not FDA approved for therapeutic use.
The researchers validated Vinpocetine in cell culture conditions and found the neuroprotection was mediated by an increase of cGMP. They also found that Vinpocetine could rescued dopamine neurons in mice with very high levels of alpha synuclein.
The investigators concluded “inhibition of phosphodiesterase 1 in particular as promising target for neuroprotective treatment” for Parkinson’s.
And this research supported the findings of a previous study which demonstrated the rescue of a Parkinson’s neurotoxin rat model by Vinpocetine (Click here and here to read more about this).
Is Vinpocetine being clinically tested in Parkinson’s?
No, not that I am aware of (and I would be happy to be corrected on this matter).
But the phosphodiesterase 1 inhibitor ITI-214 has been clinically tested in Parkinson’s, right?
It has been tested in the a phase I/II trial, but it was a very short study – a larger and longer clinical evaluation of the drug is required.
So what were the results of the phase I/II study?
The trial was conducted by a biotech company called Intra-Cellular Therapies.
It was a Phase I/II randomised, double-blind, placebo-controlled study evaluating multiple ascending doses of ITI-214 in 40 people with idiopathic Parkinson’s (the spontaneous form of the condition that has no obvious causal component, such as genetics). Click here to read more about the details of the study.
The participants – all with mild to moderate Parkinson’s (Hoehn and Yahr staging score of 1-3 assessed in the “ON” state) – were allowed to maintain their normal PD treatment. They were randomly assigned to either placebo or one of five different doses of ITI-214 (1, 3, 10, 30, and 90 mg) which were orally administered once daily for 7 days.
The primary outcome of the study was to evaluate the safety and tolerability of ITI-214 in people with Parkinson’s, and it appears to have passed with flying colours. All of the randomised participants completed the study, and no serious adverse events were reported during the trial. And ITI-214 appears to be a safe drug as no clinically significant effects (compared to placebo) were reported on vital signs such as cardiovascular measures.
The researchers also investigated the efficacy of ITI-214 for its abiity to improve motor and non-motor symptoms of PD using multiple tests. The company reports that motor performance was improved in the “On” state by ITI-214 (compared to placebo) as assessed by the clinician-based MDS-UPDRS (Movement Disorder Society Unified Parkinson’s Disease Rating Scale). ITI-214 reduced both total scores on the MDS-UPDRS, as well as 2 subscales (Part III – the motor scores – and Part IV – motor complications, such as dyskinesias). And this effect on dyskinesias was also observed using the UDysRS (Unified Dyskinesia Rating Score). Improvements were also reported in increased total ‘ON’ time and ‘ON’ time without dyskinesias as rated by the participants themselves (using the Hauser Patient Motor Diary).
This study was very short (only 7 days of treatment), but it will be interesting to see the full data of the study once they are published – these results were simply provided in the press release. These initial findings are very encouraging though. And Intra-Cellular Therapies has indicated that they are very encouraged by them as well: “The favorable safety profile and clinical signals in this trial support the advancement of the ITI-214 development program in Parkinson’s” (Source)
We will be looking for news of the initiation of a larger and longer Phase II/III trial in the not-too distant future.
So what does it all mean?
A biotech company called Intra-Cellular Therapies has presented the results of a Phase I/II clinical trial that suggest their novel drug ITI-214 – a phosphodiesterase-1 inhibitor – is having an effect in people with moderate Parkinson’s. Until the full results are published, I am reluctant to get too excited, but I have to admit that these results are very interesting, for one simple reason:
ITI-214 represents a very novel approach to treating Parkinson’s.
If a much larger and longer Phase II/III clinical trial can replicate the results of the Phase I/II trial, then we could have a very interesting new treatment for PD. And it may also potentially tell us something about the underlying biology of Parkinson’s (remember PDE1 only becomes activated when calcium levels increase).
To get a better handle on this latter point, however, it would be very useful if Intra-Cellular Therapies were to publish some of their preclinical research in Parkinson’s models for us to consider – and the SoPD would be very happy to highlight it all here. My only concern with this drug is the lack of published preclinical research (Click here, here and here to read the only published material I could find – none of it directly PD related).
So, we will be looking forward to the initiation of a larger and longer Phase II/III clinical trial of ITI-214 in Parkinson’s and the opportunity to read some of the preclinical research.
That’s not too much to ask for is it? Christmas is coming.
EDITOR’S NOTE: Intra-Cellular Therapies is a publicly traded company. That said, the material presented on this page should under no circumstances be considered financial advice. Any actions taken by the reader based on reading this material is the sole responsibility of the reader. Intra-Cellular Therapies has not requested that this material be produced, nor has the author had any contact with the company or any associated parties. This post has been produced for educational purposes only.
The banner for today’s post was sourced from Nutraingredients-usa

Wow, what an amazing combination of answers to questions I was already wondering about, and things I never suspected but really needed to know.
My partner (who has PD) has been using vinpocetine for the past year or so, but only as a way to direct more blood to the head area, so as to offset some of the effects of neurogenic orthostatic hypotension (nOH), which has developed as a consequence of her being in the later stages of PD. I have also been using it myself with complete success to dissolve otoliths (through increased blood flow to the head area, in order to carry away calcium faster than the stones can form). These were causing me to have Benign Positional Paroxysmal Vertigo – a condition that resolved within a day of starting vinpocetine at 10mg twice daily, and which starts to return whenever I miss one or two consecutive doses.
[By the way, for those reading this who may have nOH, be warned that vinpocetine can cause a slight overall *lowering* of blood pressure, and for that reason those with nOH are often advised *against* using it. But we reasoned that since it selectively dilates the vasculature that leads to the head *specifically*, allowing more blood to flow to the *brain*, it could actually help to *reduce* the faintness that results from nOH. I mean, the circulation through the brain should be proportional to pressure, but also *inversely* proportional to *resistance*, right? In fact, I *suspect* that the slight lowering of blood pressure at the cuff is *due* to the additional blood that flows to the head. This is entirely our own idea, and I don’t have any studies supporting it, but it makes sense to us and we believe that it has been helpful to my partner. Still, be warned, using vinpocetine is contrary to the usual advice that someone with nOH would receive. And if anyone can present an argument that the above reasoning is wrong, we’d appreciate hearing it!]
While I knew that vinpocetine worked to enhance circulation to the head area by inhibiting PDE1, I have learned so much more about *how* it does that from this article. That cyclic AMP and cyclic GMP play a role not only in blood vessel dilation, but also in combating inflammation, was not known to me. Nor did I realize that PDE1 worked by inhibiting the action of cGMP and cAMP, and that therefore vinpocetine’s inhibition of PDE1 prevents the PDE1 from inhibiting cAMP and cGMP, resulting in enhanced anti-inflammatory effects and vascular dilation.
But the completely unexpected information was that the increase in cGMP activity caused by vinpocetine reduces the toxicity of alpha synuclein. That was a real revelation, and great to hear, since my partner has been using it for a year now while having no idea of that benefit. And I had no idea that the striatum had higher than normal levels of PDE1, making it more sensitive to the effects of vinpocetine. Although, I kind of suspect that the *heart* of the PD inflammatory process is in the substantia nigra, where the dopaminergic cells bodies are located, rather than in the striatum, where their axons terminate.
From the linked Nature article, it seems that this effect occurs through a reduction of aggregated forms of alpha synuclein. This leads me to wonder how this effect compares to similar reductions attained through the use of EGCg (mentioned for that ability in the article), baicalin and curcumin. Are their preventive effects against AS aggregation synergistic or redundant with those of vinpocetine?
I also have to wonder: what does this new drug ITI-214 have that vinpocetine does *not* have? Aside from a monetizable drug patent, I mean. Why reinvent what already exists? Is this new drug better somehow?
Also, given that PDE1 only becomes activated when calcium levels increase, I’m wondering then if *atherosclerosis* causes PDE1 to activate, removing some of the antiinflammatory benefits of cAMP and cGMP, and thus contributing to a worsening of PD in patients with atherosclerosis. If so, then this could mean that vinpocetine would have additional benefit for atherosclerotic PD patients.
This article was really helpful to us; thank you so much for writing it.
LikeLike