
|
# # # # In cancer research, scientists have devised methods of extracting samples of blood from patients and then growing certain populations of cells in those samples. The isolated subpopulations of cells can then be manipulated in cell culture, before they are then injected back into the patient. This is a form of immunotherapy – artificially boosting the immune system to target specific disease-related pathology in the body. Recently, researchers have been exploring this alternative form of immunotherapy in the context of Parkinson’s… with some interesting results. In today’s post, we will look at review this new research and consider the implications in terms of future therapies for Parkinson’s. # # # # |
 Source: lls
Source: lls
Some time back, a friend in oncology (cancer) research said to me that “we are about to cure all blood cancers“. It should be noted that this optimistic friend is a “glass is completely full” type.
“How so?” I asked.
“CAR T-cell technology is amazing. Really coming into bloom” they responded.
“What is CAR T-cell technology?” I asked.
They explained that it is a kind of immunotherapy – a method of boosting the immune system to help us fight disease.
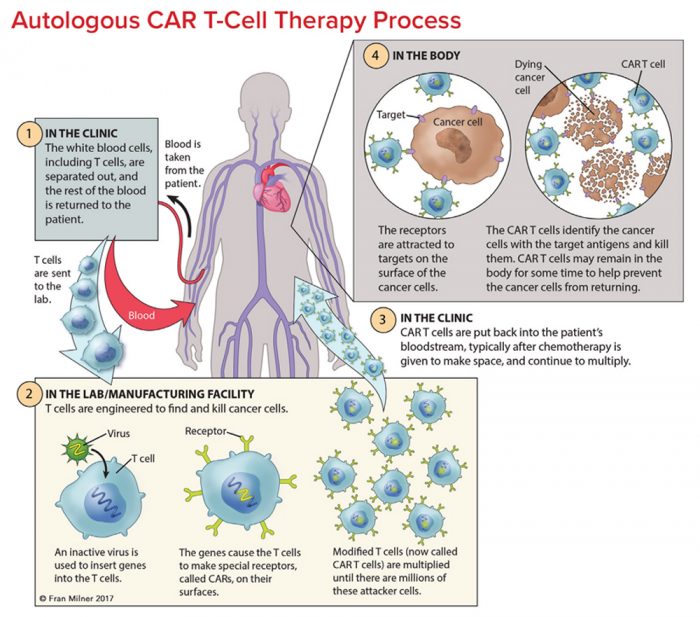
CAR T-cell approaches basically involve removing a sample of blood from a person with cancer, expanding specific populations of those cells in cell culture, genetically manipulating those cells, and then re-introducing them into the body. They also explained that there were lots of different versions of CAR T-cells, with all kinds of potential applications.
“Cool” I said, sounding enthusiastic, but only half understanding what they were saying. My friend is an immunologist, and my summary here is a one sentence version of a 30 minute sermon.
But they are correct.
CAR T-cell technology is achieving really impressive results in cancer (Click here and here to read more about this topic).
Interesting. What does this have to do with Parkinson’s?
Well, recently there have been a number of research groups experimenting with different versions of this technology, and they have been producing some interesting results.
Such as?
Such as this report published in April of this year:
 Title: Ex vivo expansion of dysfunctional regulatory T lymphocytes restores suppressive function in Parkinson’s disease.
Title: Ex vivo expansion of dysfunctional regulatory T lymphocytes restores suppressive function in Parkinson’s disease.
Authors: Thome AD, Atassi F, Wang J, Faridar A, Zhao W, Thonhoff JR, Beers DR, Lai EC & Appel SH
Journal: npj Parkinson’s Disease volume 7, Article number: 41 (2021)
PMID: 33986285 (This report is OPEN ACCESS if you would like to read it)
This report came from the lab of Prof Stanley Appel of Houston Methodist Hospital. At 87 years of age, Prof Appel is a legend in the field and is still extremely active in research focused on inflammatory processes involved in neurodegenerative conditions, like ALS and Parkinson’s.
 Prof Appel. Source: Robertseale
Prof Appel. Source: Robertseale
In this study, the Prof Appel and colleagues were interested in exploring what was happening with Treg cells in Parkinson’s.
What are Treg cells?
Regulatory T (Treg) cells are a really important part of the immune system. They are a type of immunosuppressive T-cell that help to sustain homeostatic balance in the immune system (during both healthy and diseased states). They basically maintain law and order in the immune system, not letting the immune system get too out of control.
They achieve this by enforcing a “dominant negative” regulation on other immune cells, particularly other T-cells.
What are T-cells?
Thymus-derived “T” cells are a type of leucocyte.
And what is a leucocyte?
This is going to take some explaining.
Leucocytes (or ‘white blood cells’) are the part of the blood system involved in protecting the body against both infectious disease and foreign invaders. While red blood cells carry important stuff like oxygen around the body, leucocytes roam the body attacking anything that looks like it doesn’t belong.
There are five types of leucocytes:
- Neurtophils
- Eosinophils
- Basophils
- Monocytes
- Lymphocytes
T-cells are a type of lymphocyte.
When your body is attacked by a pathogen (a disease causing agent like the common cold virus), it will elicit what is called an immune reaction. The presence of the virus inside the body will be detected by cells in the immune system and given that the virus will be clearly determined to be ‘not self’ (or not part of your body), an immune response will be initiated.
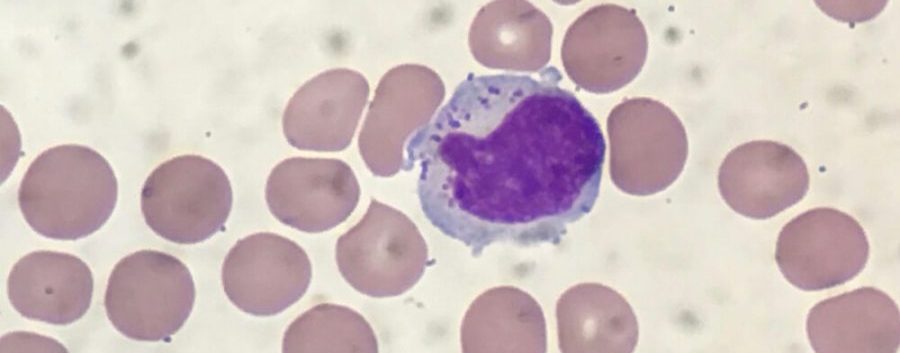
The cells that carry out the immune response are the lymphocytes.

That big cell in the middle is a lymphocyte. Source: ASH
There are basically three types of lymphocytes:
- B cells
- Natural killer cells (cool name right?)
- T cells
B cells, Natural killer cells and T cells are highly specialised blood cells that defend our body when things go wrong (which they inevitably do, it’s just the way life is!).
B cells are bone marrow-derived cells which produce Y-shaped proteins called antibodies that are used to label the invading pathogens (such as viruses), and alert other immune cells that these unwanted pathogens need to be disposed of. By sticking to pathogens, antibodies can also block them from doing their function.

Antibodies. Source: Astrazeneca
B cells do not kill pathogens, they just spend their short life producing antibodies which trap and neutralise them.
The killing of pathogens is left to the natural killer cells and T cells.
Natural killer cells were first noticed because of their ability to kill cancer tumor cells, but what made them particularly interesting was that their approach to killing: it occurred without any priming or prior activation. Natural killer cells are truly the sociopaths of the immune system – if they don’t like the looks of something, they just kill it (shoot first, ask questions later).
In the image below, you can see a large purple/blue cell (this is a natural killer cell) making contact with lots of other cells.
 A NK cell. Source: Dana-Faber
A NK cell. Source: Dana-Faber
Thymus-derived T cells also kill cells, but they do it in a more specialised fashion. T cells are ‘primed’ (by antigen presenting cells) to target very specific pathogens. They are the precision, tactical weapons of the immune system.
T cells can be identified by the presence of a T-receptor on their surface. This T-receptor identifies antigens (a molecule capable of inducing an immune response) and binds to them, which activates the T cell. Each T cell targets a specific antigen.
And the rest of this post is going to focus on T cells.
|
# RECAP #1: Blood cells have very specific functions. Red blood cells carry oxygen to all of the tissues of the body, while white blood cells are involved in the immune response to pathogens and damage. Lymphocytes are white blood cells that target pathogens. There are three basic groups of lymphocytes: B cells produce antibodies to label pathogens, while Natural killer cells indiscriminately destroy anything they don’t like. The third group, T cells, target very specific pathogens (or disease causing agents). # |
Is it time to explain what Treg cells are now?
Yes.
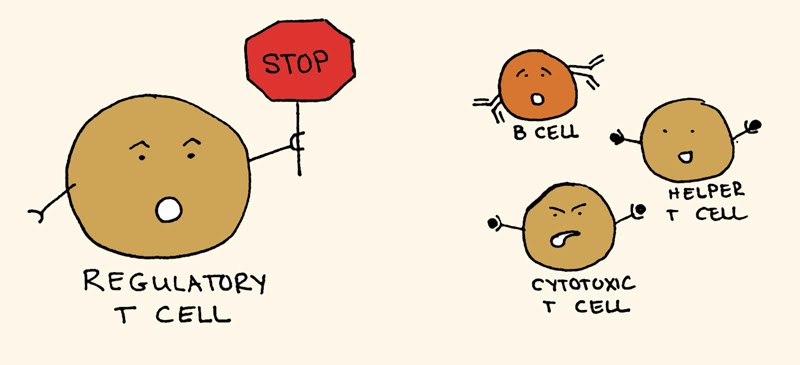
There are three basic types of T-cells:
- Cytotoxic T-cells – which directly terminate cells containing antigens by binding to them and killing them.
- Helper T-cells – which facilitate the production of antibodies by B-cells and also produce substances that activate other T-cells.
- Regulatory T-cells – which actively suppress the responses of B-cells and other T-cells.
Regulatory T-cells (or Treg cells) are the cells that maintain law and order in the immune system. They do this by enforcing a dominant negative regulation on other immune cells, particularly other T-cells.
Think of T-cells as the inquisitive neighbours curious about and snooping around a local crime scene, and then imagine that Treg cells are the police telling them “nothing to see here, move along”.
 Tregs maintaining order. Source: Keywordsuggestions
Tregs maintaining order. Source: Keywordsuggestions
Treg cells are particularly important for calming down over excited Helper T cells and Cytotoxic T cells (often referred to in combination as T-effectors). The normal situation in your body is to have a balance between Helper T cells/Cytotoxic T cells and Treg cells. If there are too many excited Helper T cells and Cytotoxic T cells, there is increased chances of things going wrong (an example of this would be autoimmunity – where the immune system starts to attack the body itself).
 A delicate balance between healthy and autoimmune disease. Source: Researchgate
A delicate balance between healthy and autoimmune disease. Source: Researchgate
One caveat here, however, is that too many Treg cells is not a good situation either, as they can leave the immune system too suppressed and individuals are therefore vulnerable to infection. Obviously a delicate balancing act is required.
And this brings us back to Prof Appel’s report:
Title: Ex vivo expansion of dysfunctional regulatory T lymphocytes restores suppressive function in Parkinson’s disease.
Authors: Thome AD, Atassi F, Wang J, Faridar A, Zhao W, Thonhoff JR, Beers DR, Lai EC & Appel SH
Journal: npj Parkinson’s Disease volume 7, Article number: 41 (2021)
PMID: 33986285 (This report is OPEN ACCESS if you would like to read it)
In this study, Prof Appel and colleagues wanted to investigate what was happening to Treg cells in Parkinson’s.
They started by collecting blood from 29 people with Parkinson’s and 25 unaffected individuals (who acted as controls). The individuals with Parkinson’s were from varying stages of disease progression (H&Y1 n = 4, H&Y2 n = 16, H&Y3 n = 5, H&Y4 n = 4).
When the samples were analysed, the investigators found a significant alteration in the T-cell populations that is consistent with a pro-inflammatory shift. They noted a reduction in the T-effector cell population (CD4 + CD25-) in Parkinson’s samples (compared to controls), but an increase in pro-inflammatory signals.
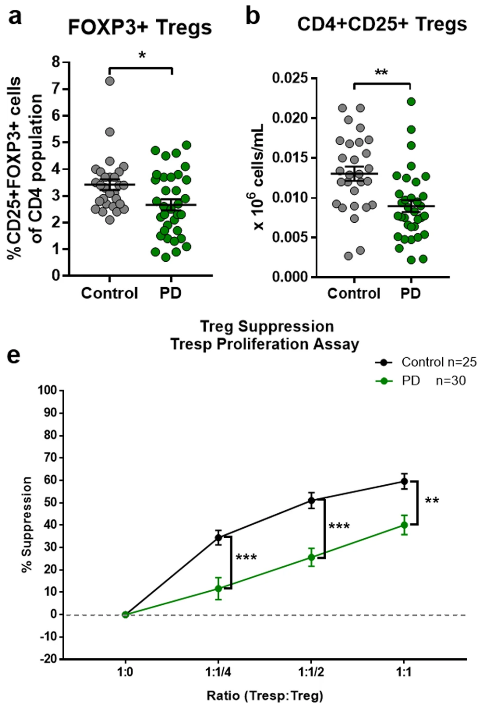
When they looked at Treg cells – the cells in charge of maintaining inflammatory homeostasis – the researchers found a significant decline in the number of Treg cells, which resulted in a significant reduction in the immune suppression ability of the PD samples:
This reduction in function of the Treg cells was playing a role in the increase in pro-inflammatory signals (like the cytokine Tumor necrosis factor or TNF) in the PD blood samples:

Interesting. What else did they find?
Next, the researchers questioned whether they could possibly restore Treg suppressive function in the PD samples by growing the cells in cell culture with proliferating T cells.
The investigators found no difference in the ability of the Treg cells to be expanded in cell culture (the PD samples grew at the same rate as the control samples). But the really interesting observation was that this co-culture of Treg and proliferating T cells resulted in an increase in suppression ability in both the control and PD samples. The control Treg cells had a 59% suppressive capacity at baseline, which increased to 79% suppression after the cells were expanded. And the PD Tregs enhanced their baseline suppression level of 42% all the way up to 84% (see panel C in the image below):

The researchers concluded their study by suggesting that expanding Treg cells in culture could “provide a potentially meaningful therapeutic strategy for cell-based immunomodulatory therapies for diseases with acute or chronic pro-inflammatory insults such as Parkinson’s“.
Has anyone else ever reported this result in Parkinson’s?
Not the expansion part (as far as I am aware – happy to be corrected on this).
But other research groups have observed reductions in Treg cells and their suppressive abilities (Click here, here, and here to read other examples).
|
# # RECAP #2: Regulatory T cells (a type of T cell) are involved in the regulation and suppression of other immune cells. Recent research indicates a reduction in the number and suppressive function of Treg cells in people with Parkinson’s. Expansion of those cells in cell culture appears to restore the suppressive properties of the Treg cells, opening the possibility of a novel therapeutic strategy for immunomodulation. # # |
Are any other neurodegenerative conditions affected by Treg dysfunction?
Yes, it would appear that Alzheimer’s is in a similar situation to Parkinson’s.
Last year Prof Appel and collaborators published this report:
 Title: Restoring regulatory T-cell dysfunction in Alzheimer’s disease through ex vivo expansion.
Title: Restoring regulatory T-cell dysfunction in Alzheimer’s disease through ex vivo expansion.
Authors: Faridar A, Thome AD, Zhao W, Thonhoff JR, Beers DR, Pascual B, Masdeu JC, Appel SH.
Journal: Brain Commun. 2020 Jul 20;2(2):fcaa112.
PMID: 32954348 (This report is OPEN ACCESS if you would like to read it)
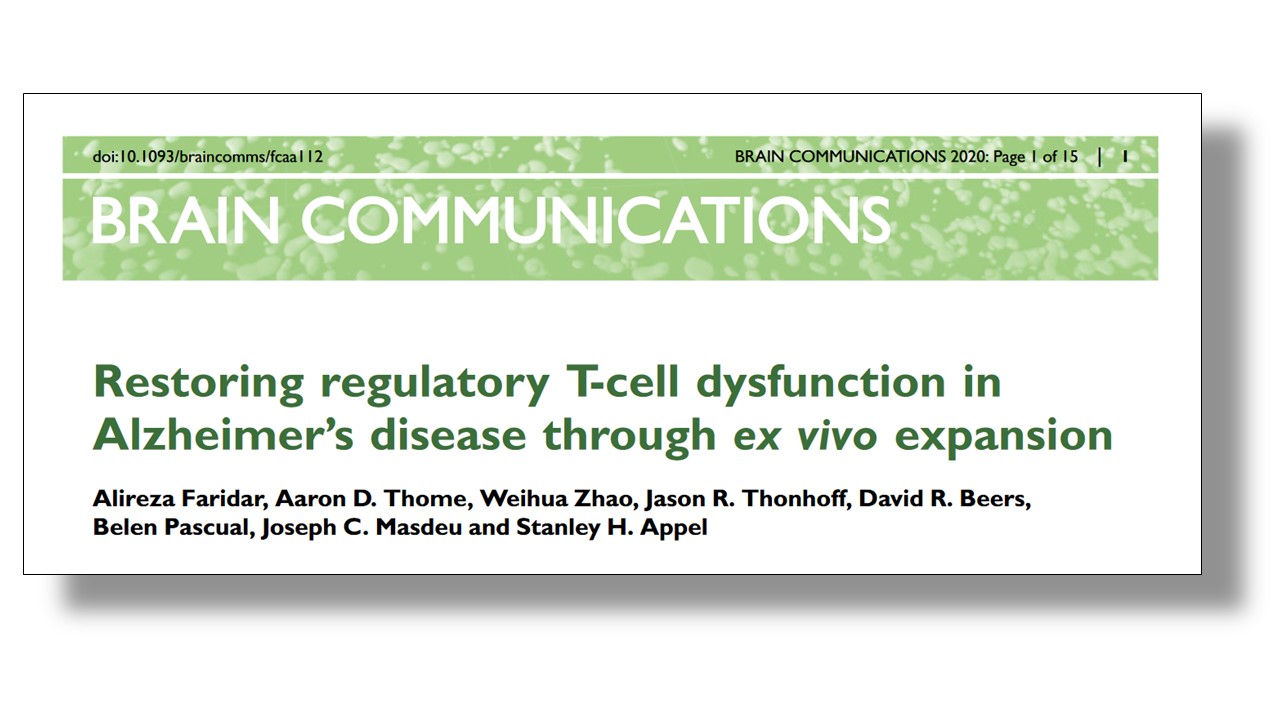
In this study, the researchers took blood samples from 46 people with Alzheimer’s, 42 people with mild cognitive impairment, and 41 unaffected individuals who served as controls. When they analysed the blood samples, the investigators found that the suppressive function of Treg cells was compromised in the Alzheimer’s samples, but not the mild cognitive impairment and control samples.
And again, following expansion of the Treg cells in cell culture, the suppressive properties of the Treg cells increased in all three groups:
 There has also been an analysis of Treg cells (again, by Prof Appel and colleagues) in blood collected from individuals affected by Amyotrophic Lateral Sclerosis (or ALS; also known as motor neuron disease):
There has also been an analysis of Treg cells (again, by Prof Appel and colleagues) in blood collected from individuals affected by Amyotrophic Lateral Sclerosis (or ALS; also known as motor neuron disease):
 Title: Endogenous regulatory T lymphocytes ameliorate amyotrophic lateral sclerosis in mice and correlate with disease progression in patients with amyotrophic lateral sclerosis.
Title: Endogenous regulatory T lymphocytes ameliorate amyotrophic lateral sclerosis in mice and correlate with disease progression in patients with amyotrophic lateral sclerosis.
Authors: Beers DR, Henkel JS, Zhao W, Wang J, Huang A, Wen S, Liao B, Appel SH
Journal: Brain. 2011 May; 134(Pt 5):1293-314.
PMID: 21596768 (This report is OPEN ACCESS if you would like to read it)
This paper is interesting for several reasons. First, the researchers reported that Treg cells are decreased in the blood of people with rapidly progressing ALS (compared to slow progressing cases or unaffected controls):
 Second, they demonstrated that the transfer of T cells from normal wild-type mice into a genetically engineered mouse model of ALS increased survival.
Second, they demonstrated that the transfer of T cells from normal wild-type mice into a genetically engineered mouse model of ALS increased survival.
And third, this study has led to a series of clinical trials, and the results of the first have been published:
 Title: Expanded autologous regulatory T-lymphocyte infusions in ALS: A phase I, first-in-human study.
Title: Expanded autologous regulatory T-lymphocyte infusions in ALS: A phase I, first-in-human study.
Authors: Thonhoff JR, Beers DR, Zhao W, Pleitez M, Simpson EP, Berry JD, Cudkowicz ME, Appel SH.
Journal: Neurol Neuroimmunol Neuroinflamm. 2018 May 18;5(4):e465.
PMID: 29845093 (This report is OPEN ACCESS if you would like to read it)
This was a very small Phase I study that was exploring whether infusions of expanded Treg cells back into individuals with ALS was safe and tolerable during early and later stages of the condition. Three participants were involved in the study, which involved taking Treg cells from each individual, expanding the cells in culture, and then reintroducing the cells back into the participant four times over 2-4 months (Click here to read more about the details of the study). The researchers found that the infusions of expanded Treg cells slowed the progression rates of all three participants.
This result has led to a Phase IIa double-blind, placebo-controlled trial that is currently ongoing. This new study involves 12 participants, who will be randomised into a treatment or placebo group. For the first 6 months of the study, a double blind study will be conducted, with some of the participants receiving a control infusion (rather than their expanded Treg cells). The second 6 months of the study will be an open-label extension in which all participants will receive their own expanded Treg cells (Click here to read more about this study).
Interesting. Are any biotech companies exploring this area?
Yes, one biotech company exploring expansion of cells and CAR T technology is Carisma Therapeutics.
![]()
While the company has not posted anything on their website’s pipeline page, Alzheimer’s and Parkinson’s have been mentioned as conditions that the company is interested in exploring (Source).
Another biotech company – called AZTherapies– is developing engineered Treg cells with chimeric antigen receptors (CAR) to specifically target the CNS to neuroinflammation in neurodegenerative conditions, like Parkinson’s, Alzheimer’s, ALS and Multiple Sclerosis (Source).
![]() So yes, there are some biotech companies working in this space.
So yes, there are some biotech companies working in this space.
The CAR T cell technology you were talking about at the top of this post involved genetically manipulating immune cells before re-introducing them. Is anyone actually doing this in Parkinson’s?
It’s a great question, and the answer appears to be yes.
In addition to the research being carried out by AZTherapies (mentioned above), in 2017 the Michael J Fox Foundation funded a project proposed by researchers at the University of Pennsylvania to look at “developing a new therapy that aims to prevent alpha-synuclein clumps from forming by engineering additional genetic material into immune cells (T cells) in a patient” (Source).
So hopefully we will be hearing more about the results of that study in the not too distant future.
So what does it all mean?
The immune system is a wonderous beast.
It is a vast, complex universe inside each of us, that ceaselessly functions to keep each of us alive and kicking. It really fascinates me that we have advanced to a point in our technological development that we are harnessing and manipulating small components of that complicated defense system to help in the treatment of disease like cancer or conditions of the brain (like Parkinson’s).
The technology is still in its infancy for neurodegeneration, but it is encouraging to see researchers already applying it to Parkinson’s in an effort to better manage and understand the condition. And hopefully positive outcomes will flow from this research, so that one day I too will be able to share an optimistic outlook with my oncology researcher friend on the future of treatment in Parkinson’s.
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
The banner for today’s post was sourced from Stemcell

could the same strategy work for Lewy body dementia?
LikeLike
The immune system is indeed a wondrous beast- wondrous in keeping most of us healthy into old age, and a beast when it turns on us in PD, AD, ALS. Thank you for highlighting the critical role of this important cell type and its therapeutic potential.
LikeLike
I love this blog because you explain what is happening so anyone can read it and yet there is no condescension in how you write
LikeLiked by 1 person
Expansion protocol, from methods section – ‘Fresh media mix with rapamycin and IL-2 were added to the cells every 2–3 days. After 10–14 days of culture, the Tregs were harvested, ‘
Perhaps treatment with low dose rapamycin would provide similar benefit (and be much cheaper and easier).
Albumin increases Treg function – supply of ‘young’ albumin may be one of the mechanisms for the benefits of therapeutic plasma exchange and the Conboys’ blood dilution experiment (though they dispute that).
Natural products that have been shown to increase Treg function in experimental models include d-mannose, fucoidan, and diosgenin.
Hypoxia increases Treg function; it has been suggested that Aviv Clinics HBOT therapy mimics hypoxia.
https://www.popsci.com/story/health/anti-aging-treatment-oxygen/
LikeLike
Another great clear and realistic state of this very interesting area of research. Keep it coming Simon!
LikeLike