
|
# # # # Sugar provides an easy and immediate source of energy for our bodies. It also helps to make things taste good, and we probably eat too much of it as a result. Recently researchers have reported a curious association between Parkinson’s and sugar: People with Parkinson’s consume more sugar In today’s post, we will review some of this new research and speculate on the potential implications of the findings. # # # # |
Today’s post needs music and the video above feels appropriate.
I have a rather sweet tooth.
In fact, if we are being completely honest: I am definitely addicted to sugar.
 It started young for me Source: Mamanatural
It started young for me Source: Mamanatural
On any given day of the week, in the late afternoon, my brain will begin screaming at me to start the mass consumption of sugar. On good days, a single chocolate cookie can satisfy the urge. On a bad day, however,… well, let’s not talk about the bad days…
 An example of my bad days. Source: Madefromchocolate
An example of my bad days. Source: Madefromchocolate
Several years ago I tried a week of no processed sugar.
It was harder than you think, because sugar is basically in everything we eat in the modern western world. And I mean everything.
 Source: Youtube
Source: Youtube
But I was really shocked that on day two of my little experiment, I was having what felt like withdrawal symptoms in the late afternoon when my brain began “screaming at me to start the mass consumption of sugar“.
It was a real struggle to get through the week, but I made it. And to reward myself,… I had… a piece of… my favourite chocolate cake.
And I was shocked at how sugary it tasted! Sickly sweet.
But it didn’t take me long to get back into my bad old habits. 2 or 3 days perhaps.
We eat way too much sugar in western society and we could all do very well by eating a lot less of it (Source). And now recent research points towards people with Parkinson’s having a higher level of sugar intake.
What?!?
This is Prof Carolyn Sue of the University of Sydney:
Professor Caroline Sue. Source: DailyTelegraph
And recently she and her colleagues published this report:
 Title: Increased Added Sugar Consumption Is Common in Parkinson’s Disease.
Title: Increased Added Sugar Consumption Is Common in Parkinson’s Disease.
Authors: Palavra NC, Lubomski M, Flood VM, Davis RL, Sue CM.
Journal: Front Nutr. 2021 May 7;8:628845.
PMID: 34026805 (This report is OPEN ACCESS if you would like to read it)
In this study, the Prof Sue and her team wanted to better understand the dietary habits of people with Parkinson’s and to identify any associations of diet with clinical PD features. So they asked 103 individuals with Parkinson’s (and 81 unaffected “control” participants) to fill in a 145-item food frequency questionnaire.
The response to this questionnaire were then analysed, with food and nutrient intake being quantified. Particular consideration was given to micronutrients and macronutrients (such as energy, protein, carbohydrate, fat, fibre, and added sugar). Demographic data was also collected from the participants, such as age, gender, ethnicity, marital status, etc. And clinical details regarding their Parkinson’s was also added to the analysis.
Ok. What did they find?
There was no difference between the PD and control groups on measures like weight or body mass index. The Parkinson’s patients had higher rates of constipation, but this was expected (Click here to read a previous SoPD post on this topic).
Biochemical analyses found that the PD group had lower total cholesterol levels, lower high density lipoprotein levels, and lower albumin levels – but all of these measures were still within normal physiological ranges. The researchers also found no difference in total intake of vitamins and other macronutrients between the groups, and when they looked at food intake, they found no difference in daily energy intake between the PD group (1130.9 kJ/day) and the control group (10188.2 kJ/day).
BUT, the PD group did report higher total carbohydrate intake (278.8 g/day) in their questionnaire answers than the control group (232.2 g/day), and this was mainly due to a significantly higher level of daily total sugar intake (153.3 g/day in the PD group vs. 118.7 g/day; p = 0.003).
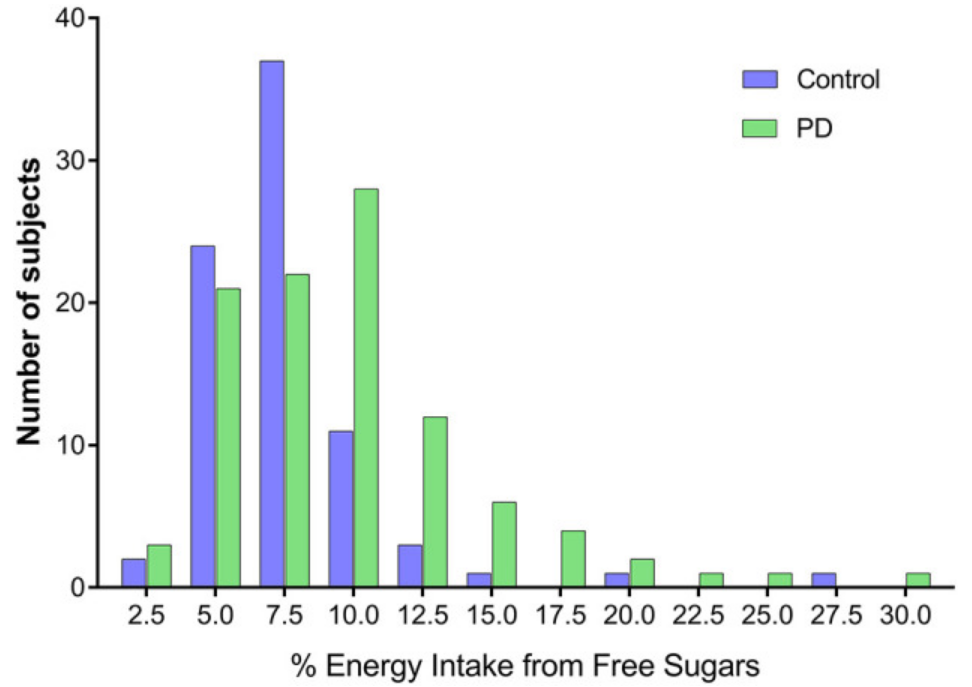
In agreement with this total sugar intake, the researchers also found that the PD group consumed more total free sugar (61.2 g/day) than the control group (40.6 g/day; p = 0.001), and almost twice as much total added sugar (52.9 g/day vs. 34.7 g/day; p = 0.001).
 Source: PMC
Source: PMC
Wow. What sort of foods were they eating?
The PD group got ~20% of free sugars from beverages (compared to just 10.4% for the control group), but the main sources of free sugars for both groups were things like “chocolate, jam/marmalade/honey, cordial, sugar, soft drinks, cake, cold breakfast cereal, and yoghurt”.
And no, the increase in sugar from beverages was not associated with alcohol intake. In fact, the PD group consumed less alcohol compared to the control group (8.9 g/day vs. 13.3 g/day).
I understand that diabetes and Parkinson’s are associated. Could that explain the increase?
Yes, there is a close relationship between PD and diabetes (Click here to read a previous SoPD post on this topic), but even when the researchers removed the participants with diabetes from their analysis, “PD patients still consumed significantly more carbohydrates, total sugar, added sugar and free sugar than healthy controls”.
Even when they removed the really high sugar intake participants from the analysis, the effect remained the same: The PD group was consuming more sugar.
Interesting. How did this increase in sugar affect their Parkinson’s symptoms?
When the researchers looked at the clinical data, they found that consuming more total sugars (than controls) was associated with:
- Experiencing chronic pain
- Cognitive decline
- Depression (curiously, depressed PD patients consumed less alcohol than non-depressed)
- Reporting of an impulse control disorder
Increased sugar consumption was also associated with an increase in other non-motor symptoms. These included poorer quality of life and increased constipation severity. It was also found to be associated with greater daily levodopa dose requirement.
Do they know what causes this effect?
There is currently no explanation for this increased sugar consumption in PD.
In the discussion of their report, Prof Sue and colleagues speculate on some possible answers. Such as, they note that “carbohydrates and sweets, through insulin, may increase brain dopamine” possibly as a compensatory mechanism for the reduced levels of dopamine in the brain due to PD. They also ask if food reward alterations could be present in PD, and that this might influence eating behaviour.
In addition, they ask if the consumption of more sugary foods could be “related to a decrease in taste function in PD patients“. A lot of individuals with PD have reduced sense of smell and this can affect the taste of food. Perhaps, a shift towards sweetness is making up for some loss of actual taste.
Alternatively, there could be a very human answer to this question: Given the association between high sugar intake and markers of disease severity (for example, more non-motor symptoms), this effect could simply be an example of comfort eating behaviour. It is possible.
Has anyone else ever reported this high intake of sugar effect before?
Yes, several studies have reported higher sugar intake in Parkinson’s (Click here to read an example).
A study published at the end of last year also reported an increase in fast acting carbohydrates (like sugar):
 Title: Increased intake of fast acting carbohydrates in patients with Parkinson’s Disease.
Title: Increased intake of fast acting carbohydrates in patients with Parkinson’s Disease.
Authors: Schäffer E, Schermann A, Zirbs F, Berg D.
Journal: Neurodegener Dis. Online ahead of print.
PMID: 34753131
In this study, the researchers were specifically interested in high-sugar content food products in a Parkinson’s cohort and they asked 221 people with PD (and 184 unaffected controls) to fill in a self-administered questionnaire.
They found that the PD group reported a significantly higher intake of chocolate. In the PD group, 14.0% of the participants consumed ≥3–4 bars of chocolate per week, compared to just 5.4% of control group. And high daily consumption of other sweets was reported in ~69% of the PD group, compared to just ~55% of the control group.
And of particular interest here is that males were the real offenders of this trend: When the researchers analysed the results based on gender, they found that the effect was not significant in females.
Curiously, when they looked at the PD group to see what differences there were between the high-sugar intake participants and the low-sugar intake individuals, they found that high-sugar intake was strongly associated with disease duration. That is to say, the intake of sugar went up with the longer people had the condition.
Could the sugar intake being playing a role in the progression of Parkinson’s?
Before we go any further, let’s be very clear – we are now speculating.
Obviously high sugar intake is bad for one’s health and it can have serious consequences. But in terms of potentially influencing Parkinson’s progression, one possibility could be the impact of glycation.
What is glycation?
Glycation is a non-enzymatic reaction between reducing sugars (such as glucose) and proteins (like alpha synuclein) or nuclei acids (think DNA/RNA). Glycation should be distinguished from another process called glycosylation, which is an enzyme-based reaction between sugars and proteins that approximately half of all proteins in a cell undergo.
Unlike glycosylation, glycation is more haphazard. And this uncontrolled activity has the effect of impairing the normal functioning of molecules and lead to the production of Advanced Glycation End product (or AGEs). AGEs are proteins or lipids that have become glycated.
This video discusses the basics of AGEs:
Glycation is known to affect the conformation and function of proteins such as hemoglobin (Hemoglobin is the protein molecule in red blood cells that carries oxygen from the lungs to the body’s tissues – Click here to read more about the glycation of this protein) and albumin (albumin is a protein made by the liver that plays an important in regulating blood volume – Click here to read more about the glycation of this protein).
Glycation generally occurs as a result of exposure to high amounts of sugar.

Source: Slowaging
And too much of it can result in the accumulation of a collection of AGEs (Click here to read a previous SoPD post on this topic).
What does glycation have to do with Parkinson’s though?
Well, recently researchers have been discovering that some of the biological pathways associated with Parkinson’s directly influence our body’s defense against glycation.
For example this study:
 Title: Glycation modulates glutamatergic signaling and exacerbates Parkinson’s disease-like phenotypes.
Title: Glycation modulates glutamatergic signaling and exacerbates Parkinson’s disease-like phenotypes.
Authors: Chegão A, Guarda M, Alexandre BM, Shvachiy L, Temido-Ferreira M, Marques-Morgado I, Fernandes Gomes B, Matthiesen R, Lopes LV, Florindo PR, Gomes RA, Gomes-Alves P, Coelho JE, Outeiro TF, Vicente Miranda H.
Journal: NPJ Parkinsons Dis. 2022 Apr 25;8(1):51.
PMID: 35468899 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers compared the impact glycation has on the Parkinson’s associated protein alpha synuclein.
In the brains of many people with PD, this protein started clumping together (or aggregating) and this accumulation of alpha synuclein is believed to influence the progression of Parkinson’s in some way (perhaps via causing cellular stress or maybe something more direct). It has previously been reported that glycated alpha synuclein can be found in the brains of people with Parkinson’s and that this modification can exaggerate the aggregation of this protein (Click here and here to read more about this).
The researchers took some genetically engineered mice that produce high levels of human alpha synuclein, and they treated them with the glycating agent methylglyoxal. They found that methylglyoxal-glycation enhanced motor, cognitive, olfactory, and colonic dysfunction in these mice (compared to untreated animals). In addition, they observed an increase in alpha synuclein aggregation in the brains of the methylglyoxal treated mice.
Interestingly, when the investigators looked closely at the brains of these mice, they found that methylglyoxal treatment mainly increased glutamatergic-associated proteins in the brain (such as NMDA, AMPA, glutaminase, VGLUT and EAAT1). Glutamate is a neurotransmitter, similar to dopamine, and the researchers discussed the possibility of anti-glutamatergic drugs holding potential promise as disease-modifying therapies for PD in the future (but this requires further exploration).
But this study demonstrates that glycation (resulting from high levels of sugar) could negatively impact a Parkinson’s associated protein which could have consequences on the progression of PD.
Again, however, we are just speculating here. On going research will hopefully expand on this and we will be enlightened in the not too distant future.
So what does it all mean?
Researchers have found that people with Parkinson’s have a high intake of sugar. The reasons for this association are not clear, but it appears to be associated with poorer quality of life and more severe symptoms.
One concerning take away from today’s post is the perception of a generally unhealthy diet in many members of the Parkinson’s community. As Prof Sue and colleagues wrote in the discussion of their report, “In 2015 the World Health Organisation (WHO) issued a recommendation that both adults and children reduce their intake of free sugars to <10% of total dietary energy to help reduce the non-communicable disease burden from unhealthy weight gain and dental caries. Notably, in this study, 28.2% of PD patients compared to 7.5% of HCs had >10% energy intake attributed to free sugars“.
Diet (like exercise) is one factor that patients can control and it has been reported to impact disease progression (Click here to read a previous SoPD post about this). Reducing sugar intake – even incrementally – should be an achievable goal, that may have positive benefits for the management of Parkinson’s.
ADDENDUM:
For those interested in this topic, a very good review has been published by the authors of one of the reports discussed above:
 Title: Parkinson’s Disease and Sugar Intake-Reasons for and Consequences of a Still Unclear Craving.
Title: Parkinson’s Disease and Sugar Intake-Reasons for and Consequences of a Still Unclear Craving.
Authors: Haas J, Berg D, Bosy-Westphal A, Schaeffer E.
Journal: Nutrients. 2022 Aug 8;14(15):3240. doi: 10.3390/nu14153240.
PMID: 35956417 (This review is OPEN ACCESS if you would like to read it)
Enjoy!
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
The banner for today’s post was sourced from DiabetesUK

Simon,
I wonder if there’s a more straightforward explanation for the higher sugar consumption observed in people with PD, particularly, as your article points out, there’s a association with disease duration and being males. Processed foods are notoriously high in sugar, but require little preparation and are therefore easier to consume. Eating healthily often requires food preparation, which becomes increasingly challenging as PD symptoms progress. For example, it now takes me twice as long to chop an onion or peel an avocado. I can see a situation where, as the disease progresses, patients rely more on easy to consume foods, such as fruits, packaged snacks and takeaway food, all of which are high in sugar. Older males may be particularly vulnerable to this since they are likely to have less food preparation experience.
Matthew
>
LikeLike
Hence why low carb and keto is the way to go with PD – ref Matt Phillips NZ
LikeLike
I think higher doses of levodopa are associated with PIGD / akinetic-rigid Parkinson’s – AKA the not as good as tremor dominant type.
LikeLike