
|
This week a new research report was released that got a few readers concerned. The article published in the journal Neuropsychopharmacology suggested that there may be an association between early onset Parkinson’s and Attention Deficit Hyperactivity Disorder (or ADHD). In today’s post, we will discuss what ADHD is, look at what the results of the study are proposing, and we will try to calm some nerves by explaining that while the results are very interesting (if they can be replicated and validated in a larger data set), the association only affects a very small number of individuals.
|

Source: Huffington Post
It may come as a bit of a surprise, but one of the most popular pages on this website deals with Attention Deficit Hyperactivity Disorder (or ADHD – click here to read that post).
I am not sure why this is the case.
At the time of writing that particular post, there was very little in the way of any associations between Parkinson’s and ADHD. But this week the number of views for that ADHD post went through the roof.
This increase in activity probably had less to do with my amazing prose and more to do with the release of this research report:
Title: Increased risk of diseases of the basal ganglia and cerebellum in patients with a history of Attention-Deficit/Hyperactivity Disorder
Authors: Curtin K, Fleckenstein AE, Keeshin BR, Yurgelun-Todd DA, Renshaw PF, Smith KR, Hanson GR.
Journal: Neuropsychopharmacology. 2018 Sep 12.
PMID: 30209407
The release of this report has been led to all kinds of media headlines (Click here and here for examples), and some panicked emails to SoPD HQ from concerned readers (particularly parents).
For those who don’t have time to read on, here is the short version of what today’s post is going to say: the results of the study are interesting, but the observed association only affects a very small number of individuals. And until the results are replicated and validated in a much larger study, there is little reason to panic.
And now for the ridiculously long version of this post – let’s start with the obvious first question:
What is ADHD?
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental condition that begins in childhood and persists into adulthood in approximately 60% of affected individuals (the degree of this can vary greatly between individuals).
The symptoms – Inattention, hyperactivity (restlessness in adults), disruptive behavior, and impulsivity – can be rather difficult to define. For example, it is hard to set a threshold at which normal levels of inattention or hyperactivity become an issue. For a diagnosis of ADHD, these symptoms must appear before the individual reaches twelve years of age. They must also be present for more than six months, and cause problems in at least two settings (e.g. school, home, etc).

Identifying ADHD. Source: Braintrainuk
Diagnosing ADHD can be problematic, even beyond the variability that it seen between cases. There are two different classification criteria that are used for diagnosis:
- the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V)
- the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10)
According to the DSM-IV criteria, ADHD affects about 5–7% of children, while the ICD-10 criteria puts this figures closer to 1–2%. Either way, a large number of individuals are believed to be affected by the condition – in 2015 it is estimated approximately 51.1 million people had ADHD worldwide (source).
There are currently believed to be three subtypes of ADHD:
- Predominantly inattentive (ADHD-PI or ADHD-I),
- Predominantly hyperactive-impulsive (ADHD-PH or ADHD-HI)
- Combined type (ADHD-C)
The subtypes generally relate to the level of hyperactivity or inattention in the individual.
And to confuse the situation further, ADHD (in children at least) appears to occur with other conditions in about two-thirds of cases. These conditions can include: epilepsy, Tourette’s syndrome, autistic spectrum disorder, anxiety disorders, learning disabilities, obsessive–compulsive disorder, sleep disorders, and oppositional defiant disorder and conduct disorder (Source).
Mood disorders (especially bipolar disorder and major depressive disorder) are particularly common in males affected by ADHD. And adolescents and adults with ADHD are at increased risk of substance abuse.
How is ADHD treated?
Treatment tends to involve a combination of behavioural therapy and medication.
Medication for ADHD can often include stimulants such as methylphenidate (also known as Ritalin).

Ritalin. Source: Wikipedia
Methylphenidate acts by blocking a protein called the dopamine transporter (or DAT), which is involved with reabsorbing the chemical dopamine back into the cell after it has performed its function.

Source: Nature
By blocking the dopamine transporter (or DAT), more dopamine is left floating around in between neurons where it can act upon receptors. On average, ritalin treatment results in a 3–4 times increase in dopamine (and norepinephrine) in the striatum and prefrontal cortex.
Now in most people, ritalin tends to make them more active and anxious. In people with ADHD, however, ritalin will make them less hyperactive and more attentive. There is evidence to suggest that people with ADHD have reduced dopamine activity in the prefrontal cortex of their brains. The prefrontal cortex (the red area in the image below) is where we do a lot of thinking and where we decide what to focus our attention on.

The prefrontal cortex. Source: Neuropsychotherapist
By giving ritalin to people with ADHD, we are increasing the levels of dopamine (and other catecholamines like Norepinephrine) in the prefrontal cortex (PFC), which helps them to focus their attention. But as we said above, if we give ritalin to normal individuals, they become anxious and become more active. This indicates that there is a ‘Goldilocks’ balancing act to the use of ritalin.
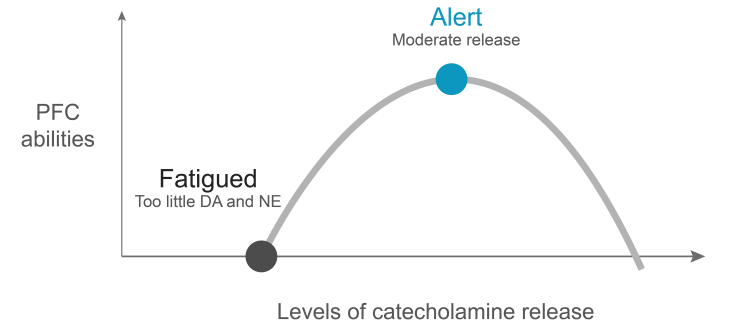
Source: Psychopharmacologyinstitute
Click here to read more about the neurobiology of ADHD.
Since dopamine is reduced in the Parkinsonian brain and ritalin increases dopamine, has anyone ever tested ritalin in people with Parkinson’s?
Yes.
A clinical trial of ritalin in Parkinson’s was set up and run in 2006 (Click here to read more about that trial). The results of the trial were published in 2007:
Title: Effects of methylphenidate on response to oral levodopa: a double-blind clinical trial.
Authors: Nutt JG, Carter JH, Carlson NE.
Journal: Arch Neurol. 2007 Mar;64(3):319-23.
PMID: 17353373 (This article is OPEN ACCESS if you would like to read it)
In this study, the researchers recruited 12 people with Parkinson’s and examined their response to ritalin (0.4 mg/kg) – given 3 times per day – in conjunction with their normal anti-Parkinsonian medication (L-dopa). They then tested the subjects with either ritalin or a placebo control and failed to find any clinically significant augmentation of L-dopa treatment from the co-administration of ritalin.
Ok, so what is this new research report that has people concerned?
This week the journal Neuropsychopharmacology released this report:
Title: Increased risk of diseases of the basal ganglia and cerebellum in patients with a history of Attention-Deficit/Hyperactivity Disorder
Authors: Curtin K, Fleckenstein AE, Keeshin BR, Yurgelun-Todd DA, Renshaw PF, Smith KR, Hanson GR.
Journal: Neuropsychopharmacology. 2018 Sep 12.
PMID: 30209407
In this study, the researchers collected medical records from the Utah Population Database and they conducted a retrospective cohort study.

Monument Valley at the Arizona-Utah border. Source: Mygrandcanyonpark
What is a retrospective cohort study?
Also called a ‘historic cohort study’, a retrospective cohort study is a longitudinal analysis of a sample of the population typically using data constructed from databases (such as healthcare records). It differs significantly from a prospective cohort study, which selects a population and follows them over time (which would be a better way of establishing an association). The weakness of the retrospective cohort study is that the study was not pre-planned and thus must use datasets that were not designed for the question being asked.
That said, sometimes you just have to use the tools that you have, and a large dataset can provide interesting insights.
Next, the investigators took a broad diagnostic definition of ADHD (ICD-9 diagnosis codes 314.0-314.2, 314.8, 314.9), which included attention-deficit disorder (ADD or ICD-9 314.00) which is a form of ADHD without the hyperacitivity, and they searched for the medical records of anyone who had been given one of these diagnoses.
They also applied a strict criteria to clean up their dataset:
- No prior diagnosis (before 1996) of Parkinson’s or any other form of parkinsonism, basal ganglia disease, or essential tremor (ICD-9 codes 332.0, 332.1, 333.0, 13 333.1)
- Born in 1950 or later and aged 20 years or older on December 31st, 2011
- No history of substance abuse (105,493 individuals excluded)
- A diagnosis of HIV infection, which can result in Parkinson’s-like symptoms (1550 individuals excluded – Click here to read a previous SoPD post about this)
They then matched each of these ‘ADHD’ records with 5 sex- and aged-matched subjects with no history of ADHD diagnosis (non-ADHD).

Man, it is just me, or is Utah beautiful? (Big Cottonwood Canyon). Source: Usnews
So what did their analysis find?
From a starting source of medical records (between 1996-2011) of 1.9 million individuals, the investigators found 31,769 people with a diagnosis of ADHD (after applying their criteria). These were matched by 158,790 non-ADHD individuals.
Similar to Parkinson’s, ADHD was diagnosed more often in men than women (57.3% vs. 42.7%, respectively), and consistent with Utah’s low level of tobacco-use the non-ADHD subjects had similar “no personal tobacco-use history” as the ADHD subjects, 29,032 (94.5% vs 91.4%, respectively).
They then followed up the medical records of these two groups (ADHD and non-ADHD) until December 31, 2016, and they noted down any diagnosis of adult-onset diseases of the basal ganglia and cerebellum (which included “Parkinson’s, secondary parkinsonism, other degenerative diseases of the basal ganglia, and essential tremor”).
Of the 31,769 individuals in the ADHD group, 56 went on to have a diagnosis of Parkinson’s.
That represents 0.18% of the total group.
And it compared to just 96 (or 0.06%) of the 158,790 individuals in the control group (non-ADHD).
The researcher concluded that this difference (0.18% vs 0.06%) represents a 2-3x increase in the risk of developing Parkinson’s. But please note again that only 56 of the 31,769 individuals in the ADHD group went on to develop PD – the vast majority (99.82%) of the ADHD group were unaffected.

Thinking about moving to Utah. Source: Kimptonhotels
Now given this curious trend, the researchers decided to dig a little further into the data and they found something else:
Of the 31,769 individuals in the ADHD group, 4,960 people who were prescribed stimulant medications. And interestingly, of these stimulant treated individuals, 19 were subsequently diagnosed with Parkinsons. And this represents 0.38% of the group, which is obviously higher than the 0.06% in the non-ADHD control group, and the 0.14% of the ADHD group that have not been administered stimulant medication.
While it is very interesting that stimulant treatment could be associated with an increased incidence of Parkinson’s within this particular group of individuals, it is important to note that only 19 people were affected out of the 4,960 that received stimulant treatment – meaning 99.62 of the individuals treated with stimulants were unaffected.
And the even researchers who conducted the study are very quick to point out that “the study results should be considered preliminary” (Source). And they suggest that parents should not panic and rush to judgement. Regarding stimulants, Prof Glen Hanson of the University of Utah Health (and the senior scientist on the report) points out that “I believe the treatment is still a benefit, especially for children who cannot control their ADHD symptoms”.
So how do we explain this possible association?
Well, firstly, the result needs to be replicated using other medical record databases before we can call this an association.
If they are validated, then I guess the question can be asked, but at present the short answer will most likely be:
We really don’t know.
And the situation is made more difficult because we are talking about a possible association between two difficult to define conditions. The between-individual variation of symptoms/features is very large for both ADHD and Parkinson’s – they are both extremely heterogeneous conditions.
One possibility is that the very small number of affected individuals (those with ADHD who went on to develop Parkinson’s) have a genetic variant that increases their risk of PD. Given that this current study was only using medical records, genetic testing was not possible.
Most cases of juvenile Parkinsonisms (diagnosis under the age of 20 years of age) and many cases of early-onset Parkinson’s (diagnosed under the age of 50 years of age) are associated with a genetic risk factor. There are approximately 23 genes that have been associated with increased risk of Parkinson’s, and they are referred to as the PARK genes. Genes are regions of DNA that provide the instructions for the production of proteins. Approximately 10-20% of people with Parkinson’s have a genetic variation in one or more of these PARK genes (we have discussed these before – click here to read that post).
And in 2014, it was suggested that genetic variations in the PARK2 gene (also known as PARKIN) contribute to the genetic susceptibility to ADHD. PARK2 is a gene called PARKIN. Mutations in PARKIN can result in an early-onset form of Parkinson’s. The PARKIN gene produces a protein which plays an important role in removing old or sick mitochondria (we discussed this in our previous post – click here to read that post).

Title: Genome-wide analysis of rare copy number variations reveals PARK2 as a candidate gene for attention-deficit/hyperactivity disorder.
Authors: Jarick I, Volckmar AL, Pütter C, Pechlivanis S, Nguyen TT, Dauvermann MR, Beck S, Albayrak Ö, Scherag S, Gilsbach S, Cichon S, Hoffmann P, Degenhardt F, Nöthen MM, Schreiber S, Wichmann HE, Jöckel KH, Heinrich J, Tiesler CM, Faraone SV, Walitza S, Sinzig J, Freitag C, Meyer J, Herpertz-Dahlmann B, Lehmkuhl G, Renner TJ, Warnke A, Romanos M, Lesch KP, Reif A, Schimmelmann BG, Hebebrand J, Scherag A, Hinney A.
Journal: Mol Psychiatry. 2014 Jan;19(1):115-21.
PMID: 23164820 (This article is OPEN ACCESS if you would like to read it)
In this report, the researchers conducted a DNA sequencing study on 489 young subjects with ADHD (average age 11 years old) and 1285 control individuals. They then replicated the study with a similar sized population of people affected by ADHD and control subjects (386 people with ADHD and 781 controls).
In both studies they found that certain deletions and replications in the PARKIN gene appears to be associated with ADHD – two of the genetic variations were found in 335 of the 875 (38%) ADHD cases and none in 2026 healthy controls (from both sets of studies).
So perhaps there could be a genetic explanation, but I have to be emphasized here that I am only speculating. The results of the Utah study need to be replicated using other medical record databases before we can make any conclusions or generate any hypotheses that could be tested.
So what does it all mean?
ADHD is a delicate topic.
It involves kids.
And kids usually involve parents/family/carers.
Being a parent, I fully understand the worry that is associated with anything to do with one’s child. Even when junior is healthy (and by this I mean, a head and a heart – everything is a bonus), there is always other kid-related stuff to worry about.
When I first saw the report of the Utah study I was very reluctant to even put it on the SoPD twitter account because I knew that it would be taken out of context and I figured that was only going to stress already stressed parents further.
But as the media noise about the study increased, it became apparent that more sober minds needed to say something.
Thankfully many of them have. For example, Prof. David Dexter, the Deputy Director of Research at Parkinson’s UK has pointed out that:
“While this study reveals a number of interesting possibilities, it’s important to stress that the increased risk identified is relatively small in people with ADHD, rising more markedly when individuals with the disorder take stimulant medications, such as Ritalin. Even in the 4,960 records of people with ADHD who were prescribed stimulant medications in this study, only 19 were subsequently diagnosed with Parkinson’s. We need to see larger studies in other populations before we can be sure that the connection is real, and to understand what is driving the relationship between the two conditions.” (Source)
I am adding my less sober (it’s Friday night!) voice to the discussion with this post.
The results of the Utah study are interesting, and the researchers should be congratulated on their efforts (it was a mammoth study). But the possible association between ADHD and Parkinson’s appears to only affects a small number of individuals and (again) the results need to be replicated and validated before we start making any conclusions.
It will also be interesting to follow up this study cohort and see if the number of cases of PD increases further with time as these individuals age. But it would be even better to conduct a proper, well designed prospective cohort study that would follow a large cohort over time and record if any associations actually exist.
Ok, I’ve said my piece – and to all the concerned parents out there, try to sleep a little easier tonight.
EDITORIAL NOTE: The information provided by the SoPD website is for information and educational purposes only. Under no circumstances should it ever be considered medical or actionable advice. It is provided by research scientists, not medical practitioners. Any actions taken – based on what has been read on the website – are the sole responsibility of the reader. Any actions being contemplated by readers should firstly be discussed with a qualified healthcare professional who is aware of your medical history. PLEASE speak with your medical physician before attempting any change in an existing treatment regime.
The banner for today’s post was sourced from stressmanagement

Thanks Simon. I always enjoy your amazing prose. Congrats on your new assignment!
LikeLike
Thanks Diana – glad you liked it!
LikeLike