
|
Novel therapies are increasing being developed to focus on specific subtypes of Parkinson’s. The hope is that if they work on one type of Parkinson’s, then maybe they will also work on others. Many of these new experimental treatments are focused on specific genetic subtypes of the condition, which involve having a specific genetic variation that increases one’s risk of developing Parkinson’s. Increasing amounts of data, however, are accumulating that some of the biological pathways affected by these genetic variations, are also dysfunctional in people with sporadic (or idiopathic) Parkinson’s – where a genetic variation can not explain the abnormality. In today’s post, we will review some new research that reports reductions in a specific Parkinson’s-associated biological pathway, and discuss what it could mean for future treatment of the Parkinson’s. |
 Source: Medium
Source: Medium
I was recently at a conference on Parkinson’s research where a prominent scientist reminded the audience that just because a person with Parkinson’s carries certain genetic risk factor (an error in a region of their DNA that increases their risk of developing Parkinson’s), does not mean that their Parkinson’s is attributable that genetic variation. Indeed, lots of people in the general population carry Parkinson’s associated genetic risk factors, but never go on to develop the condition.
And this is a really important idea for the Parkinson’s community to understand: Most of the genetics of Parkinson’s deals with ‘association’, not with ‘causation’.
But that begs the question ‘if we do not know that these errors in our DNA are causing Parkinson’s, then why should we be trying to develop therapies based on their biology?’
It is a fair question (it is also a very deep and probing question to start a post off with!).
The genetics of Parkinson’s has been extremely instructive in providing us with insights into the potential underlying biology of the condition. We have learnt a great deal about what many of the biological processess thatare associated with these genetic risk factors, and (yes) various experimental therapies have been developed to target them.
These novel treatments are clinically tested in the hope that they will have beneficial effects not just on individuals carrying certain genetic risk factors, but also on the wider Parkinson’s community.
And recently, there has been increasing evidence supporting this possibility. Some of the biological pathways associated with these genetic mutations appear to also be abnormal in people with Parkinson’s who do not carry the genetic variation.
What do you mean?
Recently this report was published:
 Title: Reduced sphingolipid hydrolase activities, substrate accumulation and ganglioside decline in Parkinson’s disease.
Title: Reduced sphingolipid hydrolase activities, substrate accumulation and ganglioside decline in Parkinson’s disease.
Authors: Huebecker M, Moloney EB, van der Spoel AC, Priestman DA, Isacson O, Hallett PJ, Platt FM.
Journal: Mol Neurodegener. 2019 Nov 8;14(1):40.
PMID: 31703585 (This report is OPEN ACCESS if you would like to read it)
In this study the researchers wanted to investigate glycosphingolipids in the Parkinsonian brain.
I’m sorry. Glyco…sphingo…what?
Glycosphingolipids (or GSLs) are a subtype of glycolipids that contain sphingosine.
And what does any of that actually mean?
A glycolipids is basically a lipid in the cell membrane (the walls of cells) with a carbohydrate (or chain of carbohydrates) attached.
Ok sure, and what does any of that actually mean?
Lipids are molecules that form the building blocks of many of the structures in living cells, such as the membrane that surrounds the cell and keeps everything inside. As you can see in the image below, there are two layers of lipids (yellow) making up the cell membrane.

Structure of the cell membrane, wth glycoproteins (violet). Source: Thinglink
Scattered about the outer surfact of the cell membrane, located in between all of those lipids are proteins that will have carbohydrates attached. These are called glycoproteins.
But hang on a second. Above you were talking about glycolipids, not glycoproteins. What’s the difference?
The primary difference between the two is that with glycoproteins the carbohydrates attach to a protein, while with glycolipids the carbohydrates attach to lipids in the membrane (it’s a slightly more complicated than that, but don’t worry about it for now).
 The main difference between glycolipids and glycoproteins. Source: vle
The main difference between glycolipids and glycoproteins. Source: vle
Interestingly, these carbohydrate chains are only present on the exterior surface of the membrane. The interior surface is devoid of any carbohydrates.
What do these chains of carbohydrates do?
They have many functions, from acting as an adhesive (by linking neighbouring cells together, these chains help maintain the integrity of the tissue) to helping the immune system determine what is ‘self’ (or part of the body) versus what is foreign (and needs to be disposed of).
Focusing on glycolipids for the purpose of today’s post: there are two different types of glycolipids: Glyceroglycolipids and Glycosphingolipids (aka sphingoglycolipids or GSL). The latter is the important one for todays discussion.

Can you spot the difference? Glyceroglycolipids and Glycosphingolipids. Source: Wikipedia
Glycolipids share a common basic structure, and it’s the bits added on that determine the difference between Glyceroglycolipids and Glycosphingolipids. Those added on bits are not important for today’s post (Glycosphingolipids are characterised by the presence of a sphingosine structure, but please don’t ask what that means – that would be a whole different post).
But the way that these glycolipids are disposed of is important for today’s post.
On a fairly regular basis, a small region of the external surface of the cell membrane is brought inside the cell. This is a process called endocytosis. It occurs when the cell consumes resources from the outside world in order to find what it needs to function and survive. It also serves as a means of recycling glycoproteins, etc on the outer membrane after they have done their job.
As a section of cell membrane is brought into the cell it forms a vesicle (a small spherical bag of stuff) that is referred to as an endosome.
 Source: Socratic
Source: Socratic
Once the endosome is inside the cell and detached from the rest of the membrane, it will bind with another vesicle which is called a lysosome. A lysosome is a small bag that is full of digestive enzymes, which help to break down the contents of the endosome. This process will provide the cell with the basic components that it needs to function normally.
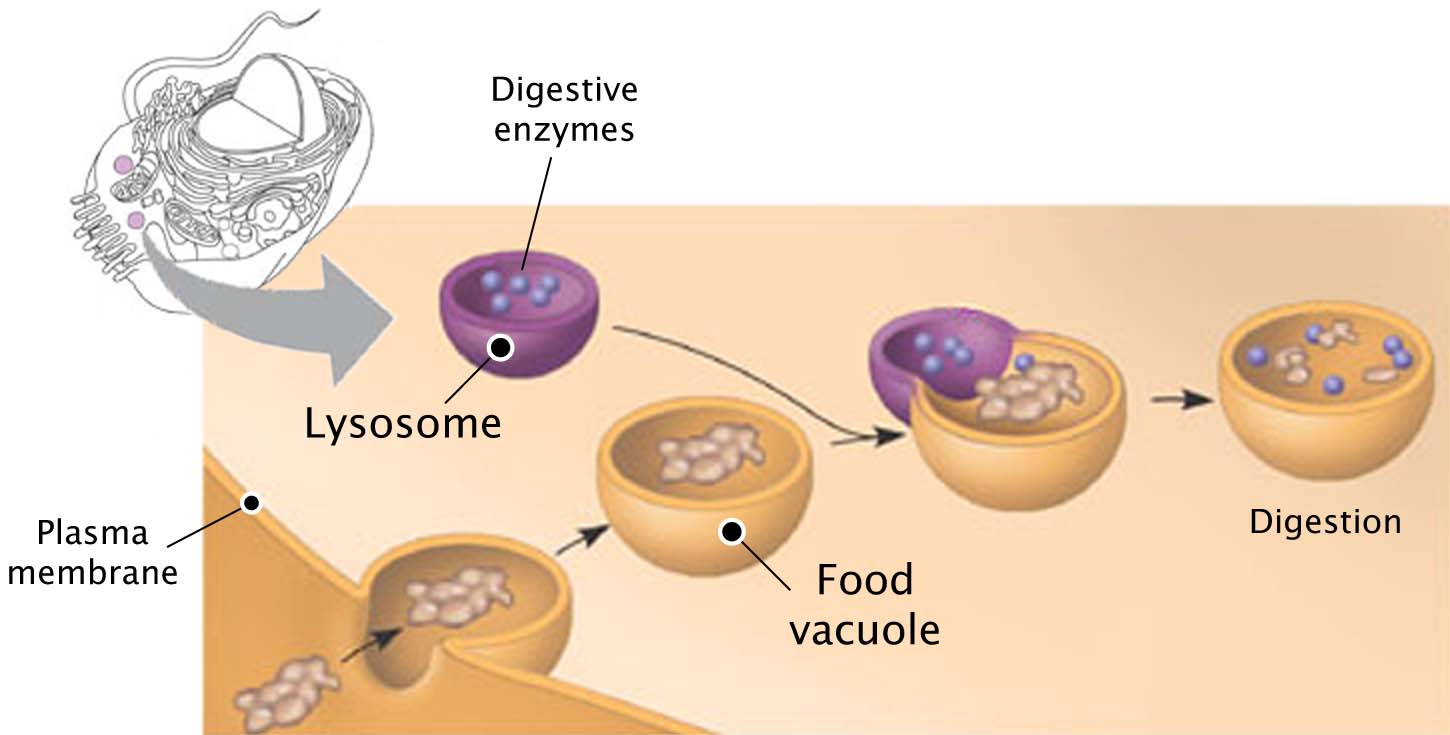 How lysosomes work. Source: Prezi
How lysosomes work. Source: Prezi
Think of the commercial products that you use for washing your clothes.
The reagents that you put into the washing machine with your clothes contain a multitude of enzymes, which help to break down the dirty, bacteria, flakes of skin, etc that cling to your clothes.
 Enzymatic degradation. Source: Samvirke
Enzymatic degradation. Source: Samvirke
Each enzyme breaks down a particular protein, fat or such like. This is very similar to the collection of enzymes in the lysosome. All of them are needed to break down all of the contents of the endosome… there is even a specific enzyme for breaking down glycoshingolipids.
And this is where we come back to the research report mentioned above.
In that research report, the investigators were interested in what happens to glycosphingolipids in the brains of people with Parkinson’s.
You see, if glycosphingolipids are not broken down properly, they start to accumulate and cause trouble.
What enzyme breaks down glyco…sphingo..whatevers?
Glucocerebrosidase (also known as GCase) is an enzyme in the lysosome that is involved in breaking down of glycosphingolipids. And the instructions for making the enzyme glucocerebrosidase are provide by a region of DNA (or a gene) called GBA1 (also known as simply GBA).
|
RECAP #1: Glycosphingolipids are a type of molecule on the outer surface of cells that needs to be broken down and recycled by an enzyme inside of cells called GCase. The instructions for making the GCase enzyme come from a region of DNA called GBA1.
|
Ok, moving on. Time for a Pub quiz question: Take a stab in the dark at which gene in your DNA is one of the most commonly affected genes in Parkinson’s?
GBA1?
Bingo!
According to the Michael J Fox foundation webpage on GBA1 “up to 10 percent of people with PD in the United States carry” a genetic variant in the GBA1 gene. It is one of the most common genetic risk factors associated with increasing ones chances of developing Parkinson’s.
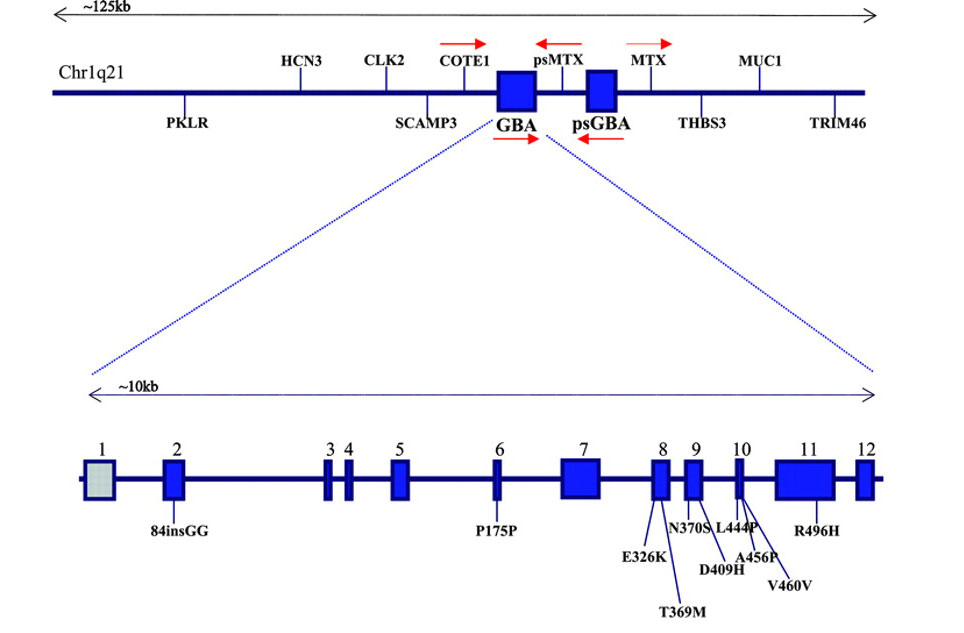 The GBA1 gene and mutations associated with Parkinson’s. Source: Neurology
The GBA1 gene and mutations associated with Parkinson’s. Source: Neurology
GBA1 is a rather large gene and there are numerous genetic variants spread across its length. The most common mutations are located in positions N370S and L444P (see blue boxes 9 & 10 in the image above).
Given that genetic variants in the GBA1 gene are so common in the Parkinson’s community, a great deal of research is being conducted on this particular gene. And in recent years this research effort has received a significant boost.
In 2016, American investment banker named Jonathan Silverstein was diagnosed with early onset Parkinson’s at 49 years of age. He has subsequently discovered that he carries a GBA1 mutation (Click here to read more about his story). In 2017, Mr Silverstein declared war on GBA1 associated Parkinson’s and established the Silverstein Foundation.
The foundation has just one mission: “to actively pursue and invest in cutting edge research with the goal of discovering new therapies for the treatment of Parkinson’s Disease in GBA mutation carriers”.
 Jonathan Silverstein. Source: DenisonMag
Jonathan Silverstein. Source: DenisonMag
The Silverstein Foundation has invested heavily in research focused on GBA-associated Parkinson’s research.
|
RECAP #2: Genetic variations in the GBA1 gene are some of the most common genetic risk factors associated with increasing ones chances of developing Parkinson’s. The Silverstein Foundation is funding research into GBA1-associated Parkinson’s.
|
That’s great for the small number of people with GBA-associated Parkinson’s, but what about the rest of the Parkinson’s community?
So this is where we return to the report we are reviewing today.
You see, there is accumulating evidence that people with Parkinson’s who have no genetic risk factors associated with Parkinson’s appear to have reduced levels of GCase activity.
What?
Many people diagnosed with Parkinson’s have lower levels of GCase enzymatic activity, even though they do not have a known genetic variation associated with Parkinson’s.
And this recent research report we looking at in today’s post highlights this idea. In their study, the researchers collected postmortem tissue 18 people who passed away with Parkinson’s (only 4 of whom had a GBA genetic mutation). These were compared with brains from 20 individuals who passed away without any signs of Parkinson’s (controls).
The researchers began there analysis by looking at the the levels of GBA1 and GBA2 in the substantia nigra (this is the region of the brain where the dopamine neurons reside – these are a group of cells severely affected in Parkinson’s).
What is GBA2?
GBA2 is an enzyme very similar to GBA1 but rather than residing in the lysosome (like GBA1), GBA2 floats freely inside the cell. It mops up any GSLs that may have broken loose somewhere in the system.
Ok, and what kind of results did the researchers find?
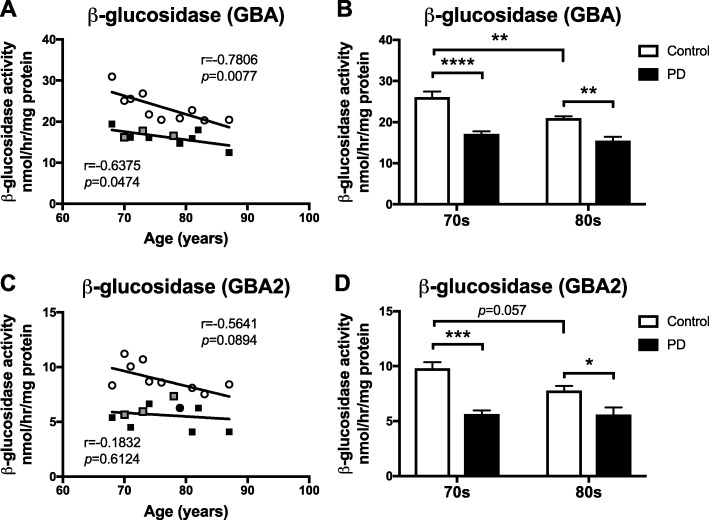
They reported that both GBA1 and GBA2 levels were reduced in the substantia nigra region of people with Parkinson’s (compared to controls). In addition, there was a general reduction in both with ageing – the older samples had lower levels compared to younger samples (in panels A & C in the image below, white circles are control samples, black squares are PD samples, and grey squares are PD with GBA mutation samples).
 Source: PMC
Source: PMC
Note that the levels of GBA1 are very similar between people with GBA-associated Parkinson’s (grey squares in panel A) and people with Parkinson’s, but no genetic variations (black squares).
Other lysosomal proteins were found to be reduced in people with Parkinson’s. For example, α-galactosidase was more than 50% reduced in the substantia nigra region of people with Parkinson’s (compared to controls).
 Source: PMC
Source: PMC
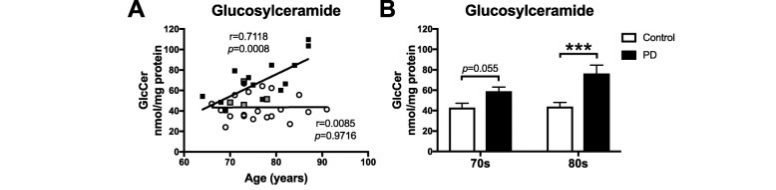
As a result of these reductions, the researchers found that GSLs were eleveated in the substantia nigra region of people with Parkinson’s (compared to controls). For example, glucosylceramide levels were significantly increased:
 Source: PMC
Source: PMC
One of the strengths of this study was that many of the results were replicated in additional samples from an independent postmortem tissue bank.
Given all of these differences, the investigators next asked whether these differences could be used as biomarkers. Could they detect similar patterns in the blood or cerebrospinal fluid of people with Parkinson’s? (cerebrospinal fluid is the liquid that the brain sits in). The analysed blood and cerebrospinal fluid samples and found significant increases in levels of GSLs like lactosylceramide in the cerebrospinal fluid, but not in the blood samples. Such findings could serve as useful biomarkers for Parkinson’s.
The researchers concluded their study by suggesting that ‘the diminished activities of these lysosomal hydrolases, the glycosphingolipid substrate accumulation, and the reduced levels of complex gangliosides are likely major contributors to the primary development of the pathology seen in PD and related disorders with age‘.
|
RECAP #3: Significant reductions in GCase activity are seen not only in the Parkinsonian brain, but also in normal ageing brains. Increases in the levels of material that GCase is supposed to digest are also observed. Differences in various proteins in blood and cerebrospinal fluids could potentially serve as biomarkers for Parkinson’s.
|
So summing up – what does it all mean?
What?
No wait, we’re not there yet.
All of this research reinforces the need for a series of clinical trials that are currently being conducted for Parkinson’s. All of these trials are all seeking to either increase the activity of the enzyme GCase or reduce various GSLs (glycosphingolipids).
The first of these clinical trials involves a clinically available drug called Ambroxol:

Ambroxol. Source: Skinflint
Ambroxol is a commonly used treatment for respiratory diseases (the respiratory system being the lungs and related components required for breathing). Ambroxol promotes the clearance of mucus and eases coughing. It also has anti-inflammatory properties, reducing redness in a sore throat. It is the active ingredient of products like Mucosolvan, Mucobrox, and Mucol.
Researchers believe that Ambroxol could help with Parkinson’s in two ways:
1. Ambroxol is believed to triggers exocytosis of lysosomes (Source). Exocytosis is the process by which waste is exported out of the cell (the opposite of ‘endocytosis’ which we discussed above). Lysosomes are the bags of digestive that rubbish and waste is put into inside a cell for recycling. By encouraging lysosomes to undergo exocytosis and spit their contents out of the cell – digested or not – Ambroxol allows the cell to remove waste effectively and therefore function in a more normal fashion.

Exocytosis. Source: Socratic
2. Ambroxol has been shown to increase levels of the enzyme glucocerebrosidase in the brain (Source).
Thus, by administering Ambroxol to people with Parkinson’s, researchers are hoping to raise levels of the enzyme glucocerebrosidase to help digest proteins and increase the excretion of this waste from cells. This would ideally keep cells healthier for longer and slow down the progression of Parkinson’s.
There are two sets of clinical trials testing Ambroxol in Parkinson’s in two different “Londons” (London, UK and London, Canada).
 London, Canada. Source: Pinterest
London, Canada. Source: Pinterest
The first study (named AiM-PD) was a phase IIA Prospective, Single-Centre, Open Label Clinical Trial to evaluate the safety, tolerability and pharmacodynamic effects of Ambroxol in Parkinson’s (Click here to read more about this trial). This trial was funded by the Cure Parkinson’s Trust, the Van Andel Research Institute(USA), and the John Black Charitable Foundation. It was testing the safety of slowly increasing doses of Ambroxol in Parkinson’s.
The study has been conducted over a 6 month period, on 20 people with Parkinson’s (critically 10 people with the GBA variant and 10 people with out a GBA mutation – Click here to read more about it). The results of this study are about to be published.
The second study is being conducted by the Lawson Health Research Institute (and the Weston Foundation) in Canada, and it is a phase II, 52 week trial of Ambroxol in 75 people with Parkinson’s Dementia (Click here to read more about this trial). In this randomised, double blind study, two doses of Ambroxol will be tested – a high dose (1050 mg) and a low dose (525 mg) – as well as a placebo treated group.
The results of this second trial will be available towards the end of 2021.
In addition to the Ambroxol trials, readers will be interested to know that the biotech company Sanofi Genzyme is conducting a series of clinical trials that are focused on a drug that will reduce glycosphingolipids/GSL levels.
![]()
The phase II trial, called MOVE-PD, is testing the efficacy and safety of a drug called Venglustat (also known as GZ/SAR402671 – Click here to read more about this clinical trial).
Venglustat is a glucosylceramide synthase inhibitor.
Glucosylceramide synthase is an enzyme involved in the production of glucocerebroside (which is the stuff that the enzyme GCase breaks down). Thus, by blocking glucosylceramide synthase, Sanofi Genzyme are hoping to reduce the amount of protein that can not be broken down by the GCase enzyme. The MOVE-PD study will enrol more than 200 patients worldwide (Click here to read more on this).
|
RECAP #4: Numerous clinical trial programs are attempting to boost GCase activity in people with GBA-associated Parkinson’s, as well as people with sporadic Parkinson’s (not associated with any known genetic variations). |
Interesting. So what does it all mean?
There is increasing evidence that some of the Parkinson’s-associated biological pathways – that are affected by specific genetic mutations – are also abnormal in people with idiopathic Parkinson’s (that is Parkinson’s with no known genetic risk factor). This is intriguing results as they support the idea that treatments being developed for GBA-associated Parkinson’s may also potentially have beneficial effects in people with sporadic Parkinson’s. In addition, such findings are enhancing our understanding of the underlying biology of Parkinson’s.
In today’s post we have looked at the GCase/GBA pathway, but we have also seen evidence for the LRRK2 pathway being dysfunctional in idiopathic Parkinson’s as well (Click here to read a previous SoPD post on this topic). And there too, a novel class of drugs is being developed (LRRK2 inhibitors) which may potentially be useful in idiopathic Parkinson’s as well as people with LRRK2-assoociated Parkinson’s.
The ongoing clinical trials of these various experimental treatments are testing this idea by incuding people with and without the respective genetic risk factors. As these clinical trials report their results over the coming few years, we should be able to address some fundamental questions regarding the nature of Parkinson’s.

All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like!
EDITOR’S NOTE – The author of this post is an employee of the Cure Parkinson’s Trust, which is a supporter of the AiMPD Ambroxol clinical trial program. The trust has not requested the production of this post, but the author considered it interesting and important to share with the Parkinson’s community.
In addition, the information provided by the SoPD website is for educational purposes only. Under no circumstances should it ever be considered medical or actionable advice. It is provided by research scientists, not medical practitioners. Any actions taken – based on what has been read on the website – are the sole responsibility of the reader. Any actions being contemplated by readers should firstly be discussed with a qualified healthcare professional who is aware of your medical history. While some of the information discussed in this post may cause concern, please speak with your medical physician before attempting any change in an existing treatment regime.
The banner for today’s post was sourced from kranzcom

Very informative!
LikeLike