
|
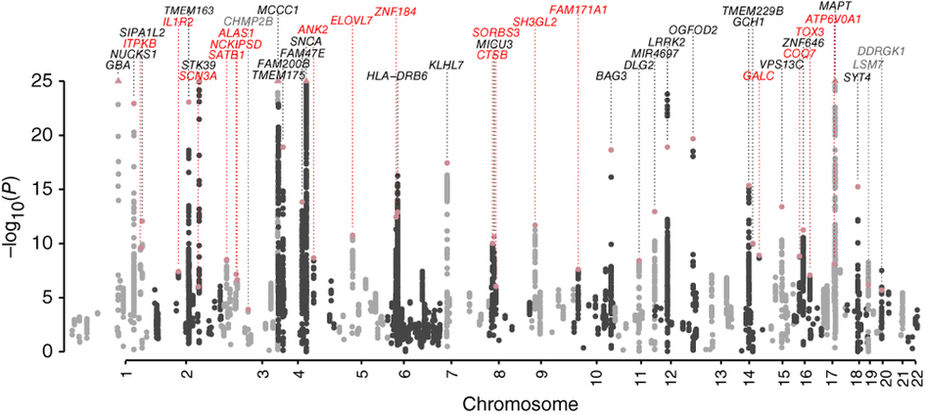
# # # # In Parkinson’s research, a great deal of the attention is focused on a handful of proteins that are associated with Parkinson’s. The majority of this knowledge has come from the discovery of genetic variations being apparent in some member of the PD community. The proteins (and biological pathways) underlying these genetic variations include alpha synuclein, LRRK2, PARKIN and GBA – all of which have been discussed on this website. But scientists have identified over 80 different regions of DNA that are associated with Parkinson’s and only recently have some of the proteins associated with these other regions of DNA been investigated. One of these proteins is particularly interesting. It’s called TMEM175. And recently published research has provided new insights into this protein. In today’s post, we will look at what is known about TMEM175 and discuss how biotech companies are therapeutically modulating it as a potential novel treatment for Parkinson’s. # # # # |
 Source: Sciencetrends
Source: Sciencetrends
Lysosomes are a key component of the waste disposal/recycling system of our cells.
They are small bags that are full of digestive enzymes that help to break down material inside of cells. Sometimes that material is newly imported from outside of the cell, while other times it may be old proteins that need to be disposed of.
Lysosomes provide the digestive enzymes for the job of breaking down the material.

How lysosomes work. Source: Prezi
We haver discussed lysosomes in previous posts in more depth (Click here to read that SoPD post) – but understand that they are an absolutely critical component of normal biological function inside of cells.
Got it. What do they have to do with Parkinson’s?






















{kind=link}
{kind=link}