
|
# # # # Novel therapeutic interventions are being proposed for Parkinson’s on a regular basis, with compelling data supporting their future development. The case is strengthened when a measure of target engagement is also involved – providing not only a potential therapy but also a biomarker as well. Recently, a biotech company called AcureX Therapeutics has been presenting just such a case, based on a biological mechanism involving the protein Miro1. In today’s post, we will discuss what Miro1 is and how it might be useful for future clinical trials. # # # # |

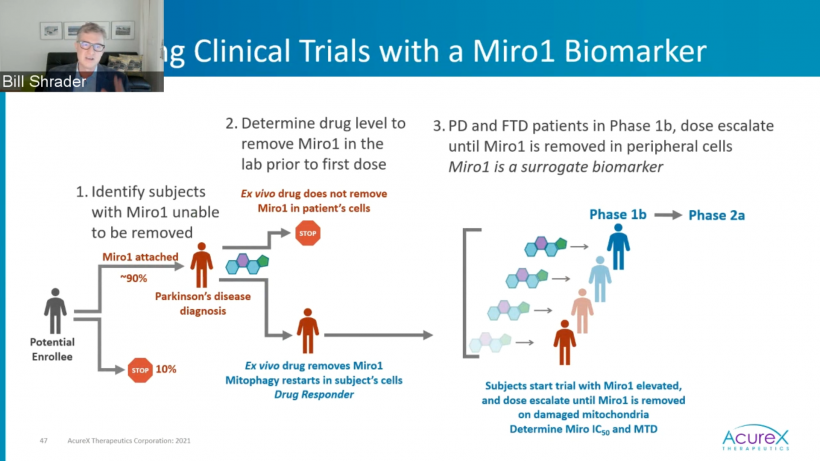
Watching the recent Michael J Fox Foundation‘s Progress in the PD Pipeline webinar (Wednesday 10th November, 2021), I was really impressed by the presentation by Dr Bill Shrader (co-founder and CEO/CSO of AcureX Therapeutics)
![]()
In particular, I really liked their approach to potential patient selection for future clinical trials of their lead drug candidate. It all revolves around the analysis of Miro1 as a biomarker.
What is Miro1?
Mitochondrial Rho GTPase 1 (or MIRO1) is a protein that sits on the outer surface of mitochondria.
We talk about mitochondria a lot on this website. They are the power stations of each cell, providing the energy that it needs to function. Mitochondria are believed to be ancient bacteria that were consumed by an equally ancient cell, and they formed a symbiotic relationship: The cells provide the food for mitochondria and the mitochondria turn that food into energy for the cells (Click here to read more about the evolution of mitochondria).
And it is a very intimate association. Without mitochondria, a cell would die.

Mitochondria and their location in the cell. Source: NCBI
The image above nicely displays a basic schematic of a mitochondrion (singular), and where mitochondria (plural) reside inside a cell.
Miro1 is a protein that attaches to the outer surface of these mitochondria.
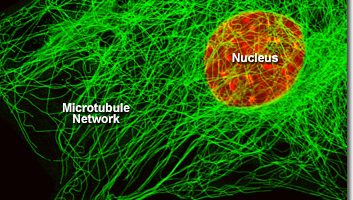
Functionally, Miro1 is a component of the complex of proteins involved with transporting mitochondria. Microtubules are the network of highways (or train tracks) inside of cells that are used to move things around.
In the image below you can see a single cell in which everything has been rendered invisible, except the nucleus (which has been stained red) and the microtubule networks (stained green):
 Source: Fsu
Source: Fsu
In order to move objects (like mitochondria) around on microtubules, mother nature invented motorproteins (such as myosins and kinesins) which crawl along the tracks, and also connector proteins (like Miro1):
 Source: Contentmanager
Source: Contentmanager
In this manner, Miro1 is a handle on the outer surface of mitochondria for the motorprotein complex to grab hold of.
|
# RECAP #1: Mitochondria are the power stations of cells, providing energy wherever and whenever it is required. Miro1 is a protein that attaches to the outer surface of these mitochondria and is involved with their transportation around the interior of cells. # |
Interesting. But what does Miro1 have to do with Parkinson’s?
Well, ten years researchers reported that Miro1 interacted with two major Parkinson’s-associated proteins: PINK and Parkin.
What are PINK and Parkin?
PTEN-induced putative kinase 1 (or PINK1) and Parkin are both ‘PARK genes’. Genetic variations within the regions of DNA that provide the instructions for making these protein (such regions are called genes) can put people at more risk of developing Parkinson’s – hence the label ‘PARK genes’.
But what do PINK1 and Parkin do?
Both proteins appear to have many different functions, but the primary role associated with them involves the process of mitophagy.
What is mitophagy?
Like you, me and all other things in the universe, mitochondria each have a use-by date.
With all their busy energy-production work, mitochondria get old and worn out (or damaged) with time. When mitochondria reach their use-by date and needs to be disposed of, they will begin to exhibit mitochondrial stress – the release of messenger molecules that state very clearly “these mitochondria need to be disposed of”. I say ‘very clearly’ because if left unattended, these mitochondria and their messenger molecules can make the cell very sick and ultimately kill it.
As a result, mother nature has devised mechanisms for disposing of mitochondria. We refer to the process removing sick/damaged mitochondria as mitophagy (a blending of the words mitochondria and autophagy). It involves the mitochondria being engulfed by a structure called a phagophore which is then infused with digestive enzymes from a lysosome, which help to break down the mitochondria.
 The process of mitophagy. Source: Circres
The process of mitophagy. Source: Circres
Like Miro1, PINK1 is a protein that also acts like a kind of handle on the surface of mitochondria. In normal, healthy mitochondria, the PINK1 protein attaches to the surface of mitochondria and it is slowly absorbed until it completely disappears from the surface and is degraded. In old, worn out, unhealthy mitochondria, however, this process is inhibited and PINK1 starts to accumulate on the outer surface of the mitochondria. Lots of PINK1 handles poking out of the surface of the mitochondria.
Now, if PINK1 is a handle, then Parkin is a flag that likes to hold onto the PINK1 handle. While exposed on the surface of mitochondria PINK1 starts grabbing the Parkin protein. This pairing is a signal to the cell that this particular mitochondrion (singular) is not healthy and needs to be removed. The pairing start the process that leads to mitophagy.

PINK1 and PARKIN in normal (right) and unhealthy (left) situations. Source: Hindawi
In the absence of normal PINK1 or Parkin proteins, there is no handle-flag system and the mitophagy process becomes slower/disrupted. Old/damaged mitochondria can start to pile up and exhibit mitochondrial stress. If they are not disposed of appropriately, the cell gets sick and ultimately dies.
 Mitophagy. Source: Frontiersin
Mitophagy. Source: Frontiersin
Interesting, but how are PINK1 and Parkin related to Parkinson’s?
People with particular genetic variations in the PINK1 or Parkin genes are vulnerable to developing an early onset form of Parkinson’s (generally before 40 years of age). It is believed that the dysfunctional disposal of (and accumulation of) old mitochondria may be part of the reason why these individuals develop the condition at such an early age.
Ok. Above you mentioned that Miro1 interacts with PINK1 and Parkin. How do they do that?
PINK and Parkin are not only involved with mitophagy, they are also involved with many other functions.
And this is where we come back to Miro1 .
In 2011, this report was published:
 Title: PINK1 and Parkin target Miro for phosphorylation and degradation to arrest mitochondrial motility.
Title: PINK1 and Parkin target Miro for phosphorylation and degradation to arrest mitochondrial motility.
Authors: Wang X, Winter D, Ashrafi G, Schlehe J, Wong YL, Selkoe D, Rice S, Steen J, LaVoie MJ, Schwarz TL.
Journal: Cell. 2011 Nov 11;147(4):893-906.
PMID: 22078885 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers reported that PINK and Parkin were responsible for the disposal of Miro1 protein.
As discussed above, Miro1 is a component of the complex of proteins involved with transporting mitochodria. It anchors the motor protein kinesin – a key protein in intra cellular transportation of objects – to the mitochondrial surface.
By getting rid of Miro1, PINK and Parkin release kinesin from the surface of mitochondria, which results in the halting of mitochondrial transportation. In this manner, PINK and Parkin are not only involved in mitophagy, but also involved with the transportation of mitochondria.
The lead researcher of this report was Assoc. Prof. Xinnan Wang, who now runs a research lab at Stanford Medical school.
 Dr Xinnan Wang. Source: Zuckermaninstitute
Dr Xinnan Wang. Source: Zuckermaninstitute
After identifying this interaction between Miro1, PINK and Parkin, Dr Wang’s team next asked what happens to Miro1 in people with Parkinson’s?
Their investigations led to the publication of this report:
 Title: Functional Impairment in Miro Degradation and Mitophagy Is a Shared Feature in Familial and Sporadic Parkinson’s Disease.
Title: Functional Impairment in Miro Degradation and Mitophagy Is a Shared Feature in Familial and Sporadic Parkinson’s Disease.
Authors: Hsieh CH, Shaltouki A, Gonzalez AE, Bettencourt da Cruz A, Burbulla LF, St Lawrence E, Schüle B, Krainc D, Palmer TD, Wang X.
Journal: Cell Stem Cell. 2016 Dec 1;19(6):709-724.
PMID: 27618216 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers collected skin cells (called fibroblasts) from people with and without Parkinson’s. They found that levels of Miro1 protein were normal in the Parkinson’s fibroblasts, when compared to healthy control cells.
When they investigators stressed the mitochondria in the cells, however, they noticed something really interesting.
Treating the mitochondria to a chemical called carbonyl cyanide m-chlorophenyl hydrazone (let’s just call it CCCP to keep things simple) for 6 hours causes Miro1 to be released and degraded in cells from healthy individuals. But – and here’s where this story starts to get interesting – when the researchers treated fibroblasts collected from 16 patients with Parkinson’s, they found that there was very little detaching and degrading of Miro1. Miro1 was holding on tightly to the surface of the mitochondria.
And the story got even more intriguing when the investigators noticed that Miro1 removal from mitochondria is delayed in cells collected from people with Parkinson’s who have a genetic variation in a third Parkinson’s-associated gene: LRRK2.
What is LRRK2?
Leucine-rich repeat kinase 2 (or LRRK2 – pronounced ‘lark 2’) – also known as ‘Dardarin‘ (from the Basque word “dardara” which means “trembling”) – is an enzyme that has many functions within a cell – from supporting efforts to move things around inside the cell to helping to keep the power on (involved with mitochondrial function).
 LRRK2 protein structure. Source: Wikipedia
LRRK2 protein structure. Source: Wikipedia
Genetic variations within the LRRK2 gene are recognised as being some of the most common with regards to increasing ones risk of developing Parkinson’s (LRRK2 variants are present in approximately 1-2% of all cases of Parkinson’s).
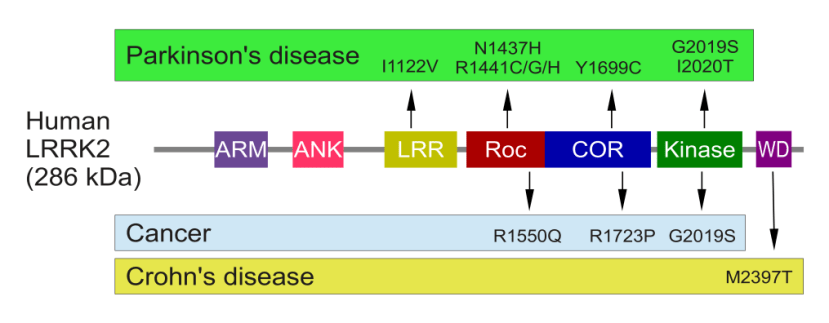
The structure of LRRK2 and where mutations lie. Source: Intech
As the image above suggests, mutations in the PARK8 gene are also associated with Crohn’s disease (Click here and here for more on this) – though that mutation is in a different location to those associated with Parkinson’s. And one particularly common Parkinson’s-associated LRRK2 mutation – called G2019S – is also associated with increased risk of certain types of cancer, especially for hormone-related cancers and breast cancer in women – Click here to read more about this. If you have a G2019S mutation, no reason to panic – but it is good to be aware of this association and have regular check ups.
The G2019S genetic mutation in LRRK2 leads to a hyperactive form of the protein, which in the carefully balanced environment of a cell is analogous to a bull of amphetamine in a china shop.
So Miro1 removal from mitochondria is delayed in Parkin, PINK and LRRK2-associated Parkinson’s?
Dr Wang and her team found that normal LRRK2 protein interacts with Miro1, and promotes the removal of Miro1 from the surface of mitochondria. But they observed that the Parkinson’s associated G2019S-LRRK2 form of the protein delayed the removal of Miro1. This delay consequently slowed the initiation of mitophagy.
Next, the researchers wanted to see what kind of affect reducing levels of Miro1 protein might have in cells with the G2019S-LRRK2 protein. Remarkably, partial reduction of Miro1 protein levels in G2019S-LRRK2 human neuron and fly (Drosophila) models of Parkinson’s restored mitophagy and protected cells from mitochondrial stress. It even rescued the motor issues that are observed in the fly models.
The researchers concluded their study suggesting that the LRRK2 and the PINK1/Parkin pathways function in parallel and converge on the interaction and degradation of Miro1, which led them to question whether “prolonged retention of Miro1 , and the downstream consequences that ensue, may constitute a central component of PD pathogenesis“.
Could Miro1 be some kind of central nexus that could be responsible for many cases of Parkinson’s?!?
But hang on a second, you suggested above that very few people with Parkinson’s have a PINK, Parkin or LRRK2 genetic variation. So how do the researchers explain this effect in everyone else with Parkinson’s?
That is a great question.
And in 2018, Dr Wang and her team published a report providing one possible explanation. This is the report here:
 Title: Alpha-synuclein delays mitophagy and targeting Miro rescues neuron loss in Parkinson’s models.
Title: Alpha-synuclein delays mitophagy and targeting Miro rescues neuron loss in Parkinson’s models.
Authors: Shaltouki A, Hsieh CH, Kim MJ, Wang X.
Journal: Acta Neuropathol. 2018 Oct;136(4):607-620.
PMID: 29923074 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers reported that the build up of Parkinson’s-associated alpha synuclein protein was correlated with increased levels of Miro1 protein. That is to say, the more alpha synuclein protein that was present in a post mortem brain from a person who passed away with Parkinson’s, the higher the level of Miro1 protein also detected in that brain. And this finding was replicated in cells which were genetically engineered to produce high levels of alpha synuclein protein (Click here to read more about alpha synuclein and its association with Parkinson’s).
And again, the investigators found that a partial reduction of Miro1 protein levels in cells with high levels of alpha synuclein rescued the cells. They also repeated this results in a fly model of alpha synuclein-associated Parkinson’s and found that it rescued them as well.
Importantly, the researchers demonstrated that the impact of alpha synuclein on Miro1 is independent of LRRK2, PINK or Parkin. And these results led the researchers to conclude that their data “positions mitochondria at the center of PD pathogenesis with Miro1 as a potentially straightforward therapeutic target”.
|
# # RECAP #2: Research indicates that Miro1 removal from mitochondria is delayed in cells collected from people with Parkinson’s. This finding suggests that a simple test involving Miro1 could be a biomarker for people with Parkinson’s. # # |
Has anyone developed any treatments targeting Miro1?
In 2019, Dr Wang and her team published this report:
 Title: Miro1 Marks Parkinson’s Disease Subset and Miro1 Reducer Rescues Neuron Loss in Parkinson’s Models.
Title: Miro1 Marks Parkinson’s Disease Subset and Miro1 Reducer Rescues Neuron Loss in Parkinson’s Models.
Authors: Hsieh CH, Li L, Vanhauwaert R, Nguyen KT, Davis MD, Bu G, Wszolek ZK, Wang X.
Journal: Cell Metab. 2019 Dec 3;30(6):1131-1140.e7.
PMID: 31564441 (This report is OPEN ACCESS if you would like to read it)
In this study, Dr Wang and her team wanted to determine in Miro1 was a useful biomarker for Parkinson’s, and to conduct a drug screen for molecules that can reduce levels of Miro1.
They began by collecting skin cells (fibroblasts) from a total of 71 people with Parkinson’s as well as 3 people people who have symptoms that put them at-risk of developing the condition. They also took a large collection of fibroblast cells from healthy control individuals.
The researchers put all of these cells in culture and treated the cells with CCCP.
After 6 hours of CCCP treatment, Miro1 was removed from the surface of mitochondria in all of the control samples. But after 6 hours of CCCP treatment, the researchers found that Miro1 was still attached to the mitochondria in 69 of the Parkinson’s and at-risk cells.
For those of you trying to do the maths, that’s 93% of the cases!
That’s amazing! So Miro1 is a Parkinson’s biomarker?
That would be a happy ending to this story wouldn’t it.
The inability to detach Miro1 was significantly associated with Parkinson’s, but it was not correlated with disease progression (based on years since diagnosis) or the clinical features of the biopsied patient (according to the UPDRS clinical rating scale). Nor was it associated with age or gender.
So it is a marker of Parkinson’s perhaps, but not any specific aspect of the condition?
Exactly.
What about other neurodegenerative conditions? Is Miro1 associated with them?
A really interesting question… with an even more interesting answer.
The researchers obtained cells from patients diagnosed with various movement disorders very similar to Parkinson’s, such as:
- Dementia with Lewy Bodies (DLB)
- Frontotemporal Degeneration (FTD)
- Sporadic Corticobasal Degeneration (CBD)
- Sporadic Progressive Supranuclear Palsy (PSP)
And guess what?
Drum roll please…
Miro1 was effectively degraded by CCCP treatment in all of these cells. The delay in Miro1 degradation appears to be specific to Parkinson’s.
So Miro1 sticking to mitochondria is really a biomarker of Parkinson’s?
Exactly.
The researchers next screened the ability of 6,835,320 commercialized small molecules (yes, that is a lot!) for their ability to remove Miro1 from the mitochondria of Parkinson’s cells. Critically, the investigators filtered the drugs for their ability to be taken orally and for their blood-brain barrier penetrance properties (the blood-brain barrier is a protective membrane surrounding the brain, stopping most drugs from entering).
And guess what?
They found 11 molecules that could reduce Miro1 in the context of Parkinson’s cells, and they selected one (#3) which they renamed ‘Miro1 reducer’ and then tested that molecule on both cells from people with Parkinson’s as well as fly models of Parkinson’s.
The researchers found that ‘Miro1 reducer’ promoted the clearance of damaged mitochondria and also protected Parkinson’s patient-derived neurons grown in cell culture against mitochondrial stress. In addition, ‘Miro1 reducer’ rescued fly models of LRRK2-, PINK-, and alpha synuclein-associated Parkinson’s.
More recently the researchers have been digging deeper into the biology underlying the Miro1 effect.
In September of this year, they published this report:
 Title: A mitochondrial membrane-bridging machinery mediates signal transduction of intramitochondrial oxidation.
Title: A mitochondrial membrane-bridging machinery mediates signal transduction of intramitochondrial oxidation.
Authors: Li L, Conradson DM, Bharat V, Kim MJ, Hsieh CH, Minhas PS, Papakyrikos AM, Durairaj AS, Ludlam A, Andreasson KI, Partridge L, Cianfrocco MA, Wang X.
Journal: Nat Metab. 2021 Sep;3(9):1242-1258.
PMID: 34504353
The researchers found that an interaction between Miro1 and another mitochondrial protein called MIC60 could be playing a key role. MIC60 is an inner mitochondrial membrane protein that when it becomes oxidised forms a bond with Miro1. Preventing the MIC60-Miro interaction either genetically or pharmacologically rescued multiple models of Parkinson’s.
Where can I get me some of that ‘Miro1 reducer’ stuff?
So this is where we come back to the biotech firm mentioned at the top of this post – the company that Dr Wang formed – called AcureX Therapeutics.
![]()
The goal of the company is to develop a ‘Miro1 reducer’ for clinical testing in people with Parkinson’s.
Dr Wang says “Our hope is that if this compound or a similar one proves nontoxic and efficacious and we can give it, like a statin drug, to people who’ve tested positive for the Miro1-removal defect but don’t yet have Parkinson’s symptoms, they’ll never get it.” (Source).
Dr Wang is suggesting here that the Miro1-removal defect could potentially be used to identify people at risk of developing Parkinson’s before they develop symptoms. She is also proposing that a ‘Miro1 reducer’ therapy could be given to such individuals and that this therapy might prevent them from developing Parkinson’s at all.
But there is still some work to be done before we get to that point.
And this is where we come back to the presentation of Dr Shrader at the recent Michael J Fox Foundation‘s Progress in the PD Pipeline webinar. As CEO and co-founder of AcureX Therapeutics, he was proposing that Miro1 could be used as a biomarker for the clinical testing of a clinical grade ‘Miro1 reducer’.
He was proposing that any individuals who were keen to take part in a clinical trial for a ‘Miro1 reducer’ agent, could firstly be tested to see if they have the Miro1-removal defect (if not, they are removed from the study). If they did, then skin cells from those individuals could be tested in culture to see if the ‘Miro1 reducer’ agent works on their cells (if not, they are removed from the study). If this test works, then the trial volunteer could be randomised and dosed with either the drug or the placebo and their clinical symptoms could be tracked over time.
During the course of the treatment arm of the study, peripheral cells could be used to track and quantify the Miro1 effect over time.
I like this type of clinical trial with a biomarker measure of drug target engagement that enables stratification of the participants before the study even begins.
Sounds like a good idea. What could possibly go wrong?
Well, as with all things in biology, there may be a Goldilocks effect in play that needs to be monitored.
Earlier this year, an independent research group published this report:
 Title: Loss of neuronal Miro1 disrupts mitophagy and induces hyperactivation of the integrated stress response.
Title: Loss of neuronal Miro1 disrupts mitophagy and induces hyperactivation of the integrated stress response.
Authors: López-Doménech G, Howden JH, Covill-Cooke C, Morfill C, Patel JV, Bürli R, Crowther D, Birsa N, Brandon NJ, Kittler JT.
Journal: EMBO J. 2021 Jul 15;40(14):e100715.
PMID: 34152608 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers found that if they genetically removed Miro1 in mice, it resulted in the appearance of “megamitochondria” – grossly enlarged and dysfunctional mitochondria, leading to increased cellular stress.
Thus, some careful consideration may be required for the dosing of a ‘Miro1 reducer’ agent in a clinical trial. It may need to be carefully titrated so as not to reduce Miro1 levels too far.
For anyone interested in reading more about Miro1 and its potential role in Parkinson’s, Dr Wang and colleagues have recently published this review:
 Title: Miro1 Impairment in a Parkinson’s At-Risk Cohort.
Title: Miro1 Impairment in a Parkinson’s At-Risk Cohort.
Authors: Nguyen D, Bharat V, Conradson DM, Nandakishore P, Wang X. Journal: Front Mol Neurosci. 2021 Aug 9;14:734273.
PMID: 34434090 (This report is OPEN ACCESS if you would like to read it)
So what does it all mean?
While I appreciate that the progress of Parkinson’s research is slower than the progress of the condition itself, I often marvel at the number of different approaches being developed at the moment as potential therapies for PD. From the common ones like alpha synuclein aggregation inhibition, LRRK2 inhibition and GCase activation, through to more novel and less well known approaches like Miro1 reduction – there are so many different ideas being tested. This is where Parkinson’s has the advantage over other neurodegenerative conditions (like Alzheimer’s or Huntington’s disease).
What we are lacking, however, are good biomarkers.
So when novel therapeutics approaches come along with a biomarker component included, I get really encouraged. And I am not the only one: The Silverstein Foundation for Parkinson’s with GBA awarded a research grant to Acurex in August of this year to further the development of the Miro1 research (Click here to read more about this).
 Here at the SoPD we will be watching with great interest the activities of AcureX Therapeutics, and looking out for similar novel therapeutic ideas with associated measures of target engagement.
Here at the SoPD we will be watching with great interest the activities of AcureX Therapeutics, and looking out for similar novel therapeutic ideas with associated measures of target engagement.
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
The banner for today’s post was sourced from Thoughtco
