
The title of this post is a play on a Thomas Jefferson quote (“the olive tree is surely the richest gift of heaven“). Jefferson, the third President of the United States (1801 to 1809), was apparently quite the lover of food. During the Revolutionary War, while he was a U.S. envoy to France, Jefferson travelled the country. In Aix-en-Provence, he developed an admiration for olive trees, calling them “the most interesting plant in existence”.
Being huge food lovers ourselves, we here at the SoPD wholeheartedly agree with Jefferson. But we also think that olives are interesting for another reason:
They contain a chemical called Oleuropein.
In today’s post we’ll explore what is known about this chemical and discuss what it could mean for Parkinson’s disease.

Olives. Source: Gardeningknowhow
The olive, also known by the botanical name ‘Olea europaea,’ is an evergreen tree that is native to the Mediterranean, Asia and Africa, but now found around the world. It has a rich history of economic and symbolic importance within western civilisation. And the fruit of the tree also tastes good, either by themselves or in a salad or pasta dish.
Traditional diets of people living around the Mediterranean sea are very rich in extra-virgin olive oil. Olives are an excellent source of ‘good’ fatty acids (monounsaturated and di-unsaturated), antioxidants and vitamins. Indeed, research has shown that the traditional Mediterranean diet reduces the risk of heart disease (Click here to read more on this).

Olive oil. Source: Bonzonosvilla
There are also chemicals within the olive fruit that may have very positive benefits for Parkinson’s disease.
But before you rush out and gorge yourself on olives, we have one small piece of advice:
The chemical is called Oleuropein, and it is usually removed from olives due to its bitterness.
What is Oleuropein?
Oleuropein is a ‘phenylethanoid’ – a type of phenolic compound that is found in the leaf and the fruit of the olive. Phenolic compounds are produced by plants as a protective measure against different kinds of stress.

Oleuropein. Source: Wikipedia
The main phenolic compounds found in olives are hydroxytyrosol and oleuropein – both of which give extra-virgin olive oil its bitter taste and both have demonstrated neuroprotective effects.
More research has been done on oleuropein so we will focus on it here (for more on hydroxytyrosol – please click here).
Oleuropein has been found to have many interesting properties, such as:
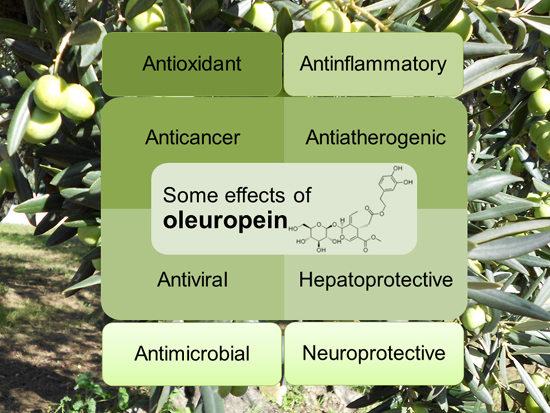
The many properties of oleuropein. Source: Mdpi
What neuroprotective research has been done on Oleuropein?
Thus far, most of the research addressing this question has been conducted on models of Alzheimer’s disease. The first study

Title: Oleuropein aglycone protects transgenic C. elegans strains expressing Aβ42 by reducing plaque load and motor deficit.
Authors: Diomede L, Rigacci S, Romeo M, Stefani M, Salmona M.
Journal: PLoS One. 2013;8(3):e58893.
PMID: 23520540 (This article is OPEN ACCESS if you would like to read it)
The Italian researchers who conducted this study treated a microscopic worm model of Alzheimer’s disease with oleuropein aglycone. We should not that oleuropein aglycone is a hydrolysis product of oleuropein (a hydrolysis product is a chemical compound that is broken apart by the addition of water). The microscopic worm used in the study are called Caenorhabditis elegans:

Caenorhabditis elegans – cute huh? Source: Nematode
Caenorhabditis elegans (or simply C. Elegans) are tiny creatures that are widely used in biology because they can be easily genetically manipulated and their nervous system is very simple and well mapped out (they have just 302 neurons and 56 glial cells!). The particular strain of C. elegans used in this first study produced enormous amounts of a protein called Aβ42.
Amyloid beta (or Aβ) is the bad boy/trouble maker of Alzheimer’s disease; considered to be critically involved in the condition. A fragment of this protein (called Aβ42) begins clustering in the brains of people with Alzheimer’s disease. This clustering of Aβ42 goes on to form the plaques that are so characteristic of the Alzheimer’s affected brain.
The Italian researchers conducting this study had previously shown that oleuropein can inhibit the ability of Aβ42 to aggregate in cells growing in culture dishes (Click here to read more about that study), and they wanted to see if oleuropein had the same properties in actual live animals. So they chose the C. Elegans that had been genetically engineered to produce a lot of Aβ42 to test this idea.
In the C. Elegans that produce a lot of Aβ42 gradually become paralysed and their lives are shortened. By treating these worms with oleuropein, however, the Italian researchers found that there was less aggregation of Aβ42 (though the levels of the protein stayed the same), resulting in less plaque formation, and improved mobility (>50% reduction in paralysis) and survival compared to untreated Aβ42 producing C. Elegans.
Encouraged by this result, the researchers next moved on to studies in mice:

Title: The polyphenol oleuropein aglycone protects TgCRND8 mice against Aß plaque pathology.
Authors: Grossi C, Rigacci S, Ambrosini S, Ed Dami T, Luccarini I, Traini C, Failli P, Berti A, Casamenti F, Stefani M.
Journal: PLoS One. 2013 Aug 8;8(8):e71702.
PMID: 23951225 (This article is OPEN ACCESS if you would like to read it)
For this study, the Italian researchers used the genetically engineered TgCRND8 mice. These mice have a mutant form of amyloid precursor protein (which, similar to Aβ42, is associated with Alzheimer’s disease). In the brains of these mice, amyloid clustering begins at 3 months of age, and dense plaques are evident from 5 months of age. The mice also exhibit a clear learning impairment from 3 months of age.
By treating these mice with oleuropein aglycone, the researchers observed a remarkable reduction in plaques in the brain, and those that were present appeared less compact and “fluffy” (their very technical description, not ours). In addition, there was a reduction in the activation of astrocytes and microglia (the helper cells in the brain), indicating a healthier environment.
These same researchers have observed the same results in a rat model of Alzheimer’s disease in a report published the next year (Click here to read more about this).
Interestingly, the oleuropein treated TgCRND8 mice also displayed a major increase in autophagy activity. As we discussed in our previous post (Click here to read that post), autophagy is the rubbish disposal/recycling system of each cell, and increasing the activity of this system can help to keep cells health (particularly if there is a lot of a genetically engineered protein present!).
The Italian researchers repeated this study, and published the results this year, with an interesting twist:

Title: Oleuropein aglycone and polyphenols from olive mill waste water ameliorate cognitive deficits and neuropathology.
Authors: Pantano D, Luccarini I, Nardiello P, Servili M, Stefani M, Casamenti F.
Journal: Br J Clin Pharmacol. 2017 Jan;83(1):54-62.
PMID: 27131215
In this study, the researchers tested the same genetically engineered mice, but with two different treatments:
- Two much lower doses of oleuropein (4 and 100 times lower)
- A mixture of polyphenols from olive mill concentrated waste water
The lowest dose of oleuropein (100 times less oleuropein than the previous study) did not provide any significant improvements for the mice, but the intermediate dose (only 4 times less oleuropein than the previous study) did provide significant benefits. These result indicate that there is a dose-dependent range to the beneficial properties of oleuropein.
The researchers also observed very similar beneficial effects from the mice drinking a mixture of polyphenols from olive mill concentrated waste water. Given these results, the investigators are now seeking to design appropriate conditions to perform a clinical trial to assess better the possible use of oleuropein (or a mix of olive polyphenols) against Alzheimer’s disease.
Ok, but what research has been done with oleuropein and Parkinson’s disease?
Unfortunately, not much.
A research group in Iran has looked at the effect of oleuropein in aged rodents and found an interesting result:

Title: Antioxidant role of oleuropein on midbrain and dopaminergic neurons of substantia nigra in aged rats.
Authors: Sarbishegi M, Mehraein F, Soleimani M.
Journal: Iran Biomed J. 2014;18(1):16-22.
PMID: 24375158 (This article is OPEN ACCESS if you would like to read it)
In this study, the investigators took twenty aged rats (18-month-old) and randomly assigned them to two groups: a treatment group (which received a daily dose of 50 mg/kg of oleuropein for 6 months) and a control group (which received just water). Following these treatments, the investigators found an increase in the activity of anti-oxidant agents (such as superoxide dismutase, catalase and glutathione) in the treatment group compared to control group. The treated rats also had significantly more dopamine neurons in the region of the brain affected by Parkinson’s disease (the substantia nigra). The investigators concluded that oleuropein consumption in a daily diet may be useful in reducing oxidative stress damage by increasing the antioxidant activity in the brain.
This first study was followed more recently by a report from a group in Quebec (Canada) who investigated oleuropein use in a cell culture model of Parkinson’s disease:

Title: Oleuropein Prevents Neuronal Death, Mitigates Mitochondrial Superoxide Production and Modulates Autophagy in a Dopaminergic Cellular Model.
Authors: Achour I, Arel-Dubeau AM, Renaud J, Legrand M, Attard E, Germain M, Martinoli MG.
Journal: Int J Mol Sci. 2016 Aug 9;17(8).
PMID: 27517912 (This article is OPEN ACCESS if you would like to read it)
The researcher conducting this study wanted to determine if oleuropein could prevent neuronal degeneration in a cellular model of Parkinson’s disease. They exposed cells to the neurotoxin 6-hydroxydopamine (6-OHDA) and then investigated mitochondrial oxidative stress and autophagy.
What is mitochondrial oxidative stress?
Mitochondria are the power house of each cell. They keep the lights on. Without them, the lights go out and the cell dies.

Mitochondria and their location in the cell. Source: NCBI
Oxidative stress results from too much oxidation. Oxidation is the loss of electrons from a molecule, which in turn destabilises the molecule. Think of iron rusting. Rust is the oxidation of iron – in the presence of oxygen and water, iron molecules will lose electrons over time. Given enough time, this results in the complete break down of objects made of iron.

Rust, the oxidation of metal. Source: TravelwithKevinandRuth
The exact same thing happens in biology. Molecules in your body go through a similar process of oxidation – losing electrons and becoming unstable. This chemical reaction leads to the production of what we call free radicals, which can then go on to damage cells. A free radical is an unstable molecule – unstable because they are missing electrons.

How free radicals and antioxidants work. Source: h2miraclewater
In an unstable format, free radicals bounce all over the place, reacting quickly with other molecules, trying to capture the much needed electron to re-gain stability. Free radicals will literally attack the nearest stable molecule, to steal an electron. This leads to the “attacked” molecule becoming a free radical itself, and thus a chain reaction is started. Inside a living cell this can cause terrible damage, ultimately killing the cell.
Now if this oxidative process starts in the mitochondria, it can be very bad for a cell.
And what is autophagy?
Yes, the researchers also looked at autophagy levels in their cells. Autophagy is an absolutely essential function in a cell. Without autophagy, old proteins and mitochondria will pile up making the cell sick and eventually it dies. Through the process of autophagy, the cell can break down the old protein, clearing the way for fresh new proteins to do their job.
Think of autophagy as the waste disposal/recycling process of the cell.

The process of autophagy. Source: Wormbook
Waste material inside a cell is collected in membranes that form sacs (called vesicles). These vesicles then bind to another sac (called a lysosome) which contains enzymes that will breakdown and degrade the waste material. The degraded waste material can then be recycled or disposed of by spitting it out of the cell.
Ok, so what did the researchers find?
Well, by pretreating the their cells with oleuropein 3 hours before exposing them to the neurotoxin, the investigators found a significant neuroprotective effect. There was a significant reduction in mitochondrial production of free radicals, and the investigators found an important role for oleuropein in the regulation of autophagy.
And the good news is that other research groups have observed similar beneficial effects of oleuropein in cell culture models of Parkinson’s disease (Click here to read more about that).
The bad news is: that is all the published research on oleuropein and Parkinson’s disease we could find (and we would be happy to be corrected on this if people are aware of other reports!).
So what does Oleuropein do in the brain?
This is a good question, but with so little research done in this area, it is hard to answer.
We know that oleuropein is well absorbed by the human body and that it is relatively stable (Click here to read more on this). In addition, it can cross the blood-brain-barrier – in rodents at least (Click here to read more on that).
Obviously (based on the research we described above), we know that oleuropein has anti-oxidant promoting activities. In addition, it appears to be doing something with regards to autophagy. And it may be regulating autophagy by acting as an inhibitor of mammalian target of rapamycin (mTOR) activation.
What is mTOR?
mTOR is a protein that binds with other proteins to form the nexus of a signalling pathway which integrates both intracellular and extracellular signals (such asnutrients, growth factors, and cellular energy status) and then serves as one of the central instructors of how the cell should respond.
For example, insulin can signal to mTOR the status of glucose levels in the body. mTOR also deals with infectious or cellular stress-causing agents, thus it could be involved in a cells response to conditions like Parkinson’s disease.

Factors that activate mTOR. Source: Selfhacked
One important property of mTOR is its ability to block autophagy (the recycling process of the cell that we discussed above). Recently, the Italian researchers whose work we reviewed above, found that oleuropein can activate autophagy by blocking the mTOR pathway:

Title: Oleuropein aglycone induces autophagy via the AMPK/mTOR signalling pathway: a mechanistic insight.
Authors: Rigacci S, Miceli C, Nediani C, Berti A, Cascella R, Pantano D, Nardiello P, Luccarini I, Casamenti F, Stefani M.
Journal: Oncotarget. 2015 Nov 3;6(34):35344-57.
PMID: 26474288 (This article is OPEN ACCESS if you would like to read it)
The researchers conducting this study found that treatment with oleuropein caused an increase in autophagy in both cell culture and in a mouse model of Alzheimer’s disease, and they demonstrated that it achieved this by blocking the mTOR pathway.
Has anyone ever looked at oleuropein in the clinic?
No, not to our knowledge (and we are happy to be corrected on this).
There have been six clinical trials of olive leaf extract (the majority of which is oleuropien), but none of them have been focused on any neurological conditions.
So oleuropein is safe then?
It is a widely available supplement that a lot of people use to help lower bad cholesterol and blood pressure, so yes it can be considered safe. But any decision to experiment with oleuropein should only be made in consultation with your regular medically trained physician.
Why? Because there are always caveats.
Importantly, individuals with low blood pressure and diabetes may suffer even lower blood pressure and blood glucose levels as a result of consumption of oleuropein. Oleuropein may also interact with other pharmaceutical drugs that are designed to lower blood pressure or regulate diabetes. Such interactions could be dangerous.
And this is a particularly important factor for Parkinson’s disease as up to 30% of people with Parkinson’s may be glucose intolerant (Click here to see our post on Parkinson’s & diabetes).
Those who experience symptoms such as headache, nausea, flu-like symptoms, fainting, dizziness, and other life threatening symptoms should medical attention immediately.
What does it all mean?
We are grateful to regular reader (Don) who brought oleuropein to our attention. It is a very interesting chemical and we are definitely intrigued by it. We would certainly like to see more research on oleuropein in models of Parkinson’s disease.
Attentive readers will have noticed that most of the research discussed above have been conducted in the last 5-10 years. This suggests that oleuropein research is still in its infancy, particularly with regards to research on neurological conditions. And we hope that by reporting on it here, we will be bringing it to the attention of researchers.
Oleuropein is extracted from all parts of the olive tree (the leaves, bark, root, and fruit). It forms part of the defence system of the olive tree against stress or infection. Perhaps we could apply some of its interesting properties to Parkinson’s disease.
EDITORIAL NOTE: Under absolutely no circumstances should anyone reading the material on this website consider it medical advice. The information provided here is for educational purposes only. Before considering or attempting any change in your treatment regime, PLEASE consult with your doctor or neurologist. While some of the drugs and supplements discussed on this website are clinically available, they may have serious side effects. We urge caution and professional consultation before altering any treatment regime. SoPD can not be held responsible for any actions taken based on the information provided here.
The banner for this post was sourced from jrbenjamin

 Immune cells (blue) checking out a suspect cell. Source: Lindau-nobel
Immune cells (blue) checking out a suspect cell. Source: Lindau-nobel Many approaches to immunotherapy against cancer. Source: Bloomberg
Many approaches to immunotherapy against cancer. Source: Bloomberg Source: RND
Source: RND






























{kind=link}