
|
Last week one of the most comprehensive analyses assessing the risk of developing Parkinson’s following mild traumatic brain injury (or TBI) was published. Using data collected from US military veterans, the study concluded that mild TBI was associated with a 56% increased risk of developing Parkinson’s. In today’s post, we will review the study, discuss what TBI means, and consider what implications this study could have for the Parkinson’s community. |

Source: Jamesriverarmory
At a recent research conference, a young PhD student was looking at me from across the room.
Finally, she walked across to me and asked:
“Excuse me. Are you the goat guy?”
I smiled.
It had been a while since anyone had asked me this.
“Yes,” I replied, “I am the goat guy”
Let me explain:
One evening over drinks, a group of us in a previous research institute had been sharing stories and I can’t remember how we got on to the topic, but I told them the ‘goat story’.
As a kid growing up in the back waters of third world New Zealand, I raised a pet lamb every year. We would teach it to do a trick or two, and then present them at my local school agricultural day. Anyways, one bad lambing season I was given a baby goat which I named ‘Billy the kid’ (yes, I was always an original thinker).

Not Billy, just a perfect look-alike. Source: Youtube
Billy was a good pet. I have many happy memories of long afternoons hanging out with him. But as he got older, he developed a desire to head butt things, and I would placate him by providing my fist for him to vigorously go at. Then one day (perhaps you can already see where this is going), I wondered what his reaction would be if I put out my head instead of my fist (I can honestly provide no real insight into how this idea formed in my head, it just did).
And so I got down on all fours and presented my cranium for Billy to consider.
I will not attempt to describe the flash of excitement and delight that passed across Billy’s eyes when he was presented with such a challenge. And the last thing I actually remember was a silhouette of Billy rearing up on his hind legs with the late afternoon sun behind him (and perhaps there was a last second moment of me questioning whether this was such a good idea).
I do not remember him coming down or the actual blow of our heads colliding.

Not 9 year old me. Source: Parade
When I woke, Billy had snuggled in beside me. He was chewing on a bit of grass and enjoying the last gasps of twilight. And perhaps there was a jaunty air of the victor about him. He certainly didn’t look remotely affected by our knock, while I had an absolutely killer head ache. I lay there for a moment gathering my wits, wondering how long I had been out. And I questioned whether I should tell anyone about what had happened (dear lord, how would I even begin to explain?!?).
Obviously I chose not to.
Until, that is, after a few drinks with colleagues who loved the story and decided to share it with others in the research community.

Source: Thetab
Now, some of you will obviously be asking yourselves ‘why on Earth is he sharing this?‘
The truth is, this was probably the least embarrassing story involving one of the bangs my head has taken over the years. But as a neuroscientist, I am acutely aware of the longer-term consequences of such a knock. And I have often wondered if there would be issues later on as a result of some of my early misadventures.
And recently the ‘goat guy’ story and other memories (or lack there of) came back to haunt me as I read a new research report that provided further support for an association between mild traumatic brain injury and Parkinson’s:

Title: Mild TBI and risk of Parkinson disease: A Chronic Effects of Neurotrauma Consortium Study.
Authors: Gardner RC, Byers AL, Barnes DE, Li Y, Boscardin J, Yaffe K.
Journal: Neurology. 2018 May 15;90(20):e1771-e1779.
PMID: 29669907
In this study, the researchers were interested in assessing the risk of Parkinson’s following traumatic brain injury (or TBI). They collected information for all of the patients with a TBI diagnosis in Veterans Health Administration database between October 2002 and September 2014. Next, they matched each of these cases with a random sample of patients without TBI.
In total, the records of 325,870 patients were used in the analysis. Half with these individuals were diagnosed with a TBI (average age 47.9 ± 17.4 years; average follow-up 4.6 years). When they looked at the number of individuals who were diagnosed with Parkinson’s during that period (2002-2014), they found 1,462 cases within their sample of 325,870.
Compared to individuals that had no TBI history, those with a TBI diagnosis had a higher incidence of Parkinson’s. And this incidence appears to increase with the severity of the TBI:
- The incidence of Parkinson’s in people with no TBI was 0.31% (of the total population)
- The incidence of Parkinson’s in people with any TBI was 0.58%
- The incidence of Parkinson’s in people with mild TBI was 0.47%
- The incidence of Parkinson’s in people with moderate-severe TBI was 0.75%
These results suggested that an episode of mild TBI increased one’s risk of developing Parkinson’s by 56% (and moderate-severe TBI increased it to 83%).
The results of the study highlight the importance of TBI prevention and long-term follow-up of TBI-diagnosed individuals. It also points towards the need to determine the “mechanisms and modifiable risk factors for post-TBI PD”.
Hang on a second, what exactly is meant by TBI?
Traumatic brain injury (or TBI; also known as intracranial injury) occurs when an external force injures the brain. It is classified based on severity (mild, moderate, and severe), mechanism (closed or penetrating), or other features (such as whether it occurs in a specific location on the brain or over a widespread area).
With regards to severity, mild is generally defined as “loss of consciousness for less than 30 minutes”, moderate is considered “loss of consciousness for 30 minutes to 24 hours”, and severe is “loss of consciousness for more than 24 hours” (Source).
TBI is a major cause of death/disability worldwide, especially in the young.

Source: Visually
The causes of TBI are many and varied, from falls or vehicle collisions to the result of violence or work related accidents. Most brain trauma occurs as a result of a sudden acceleration or deceleration within the cranium, causing the brain to impact the interior wall of the skull. They can also include a complex combination of both movement and sudden impact.
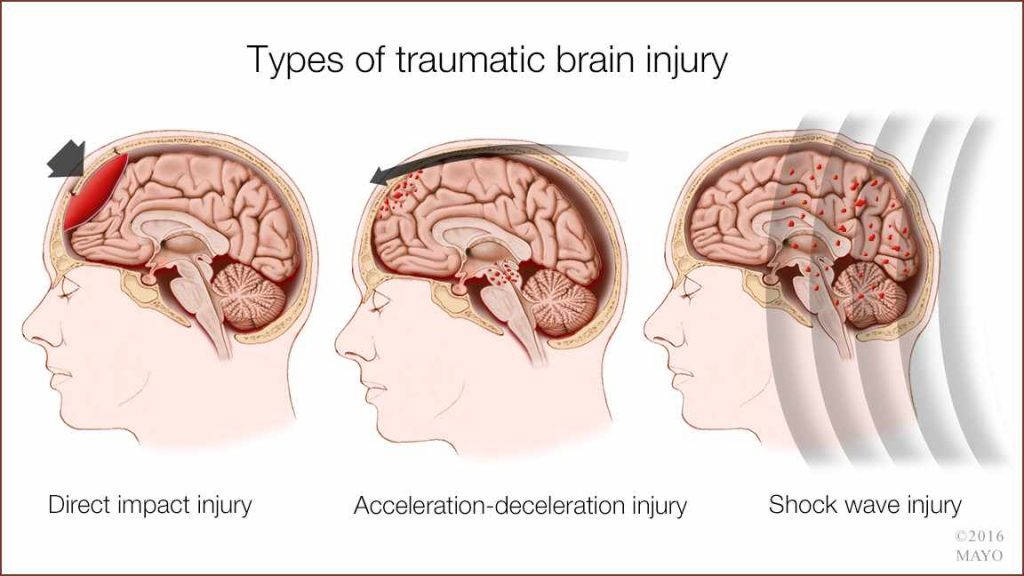
Examples of TBI. Source: Mayo
In addition to the damage that occurs at the moment of injury, additional events in the minutes to days following the injury can also occur, resulting in secondary injury. These processes include alterations in pressure within the skull and cerebral blood flow.
This video provides a full explanation of TBI (but be warned some readers may find some of the images a little disturbing):
Was this new report the first time an association has been made between TBI and Parkinson’s?
No.
As I suggested above, there have actually been several previous reports suggesting an association:

Title: Association between Traumatic Brain Injury and Late Life Neurodegenerative Conditions and Neuropathological Findings
Authors: Crane PK, Gibbons LE, Dams-O’Connor K, Trittschuh E, Leverenz JB, Keene CD, Sonnen J, Montine TJ, Bennett DA, Leurgans S, Schneider JA, Larson EB.
Journal:JAMA Neurol. 2016 Sep 1;73(9):1062-9.
PMID: 27400367 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers pooled together clinical and neuropathology data from three prospective cohort studies with the goal of determining if TBI with loss of consciousness was associated with increased risk of Alzheimer’s or Parkinson’s. Their results (based on 7,130 people with head injury data) indicated that TBI with loss of consciousness was “associated with risk of Lewy body accumulation, progression of parkinsonism, and Parkinson’s, but not dementia, Alzheimer’s disease, neuritic plaques, or neurofibrillary tangles”.
And this study is supported by another study suggesting that repeated TBI with loss of consciousness is associated with increased risk of Parkinson’s (Click here to read that study).
Some of the studies that have demonstrated an association, however, could be indicating that TBI is the result of the early stages of Parkinson’s rather than being a causal agent of the condition:
Title: Traumatic brain injury in the prodromal period of Parkinson’s disease: A large epidemiological study using medicare data.
Authors: Camacho-Soto A, Warden MN, Searles Nielsen S, Salter A, Brody DL, Prather H, Racette BA.
Journal: Ann Neurol. 2017 Nov;82(5):744-754.
PMID: 29024046
In this study, the researchers identified 89,790 incident PD cases and 118,095 comparable controls in 2009 using the large Medicare claims database. When they looked at the 5 years preceding the diagnosis of Parkinson’s, they found that TBI became more common the closer to diagnosis (the hazard ratios ranged from 1.64 at 5 years preceding diagnosis to 3.93 in the year before diagnosis). The researchers concluded that this phenomenon “may be a result of undetected nonmotor and motor symptoms, but confirmation will be required”.
And this finding is in agreement with a previous study from Denmark that found a similar trend (Click here to read more about that study). Thus, it could be that the ‘association’ between TBI and Parkinson’s could be a consequence of the evolving movement disorder rather than a causal element.
Have all of the studies found an association?
No.
While the majority of the studies suggest an association, there have been a couple of very big studies out of Scandinavia that found no association:
Title: A nationwide population study of severe head injury and Parkinson’s disease
Authors: Spangenberg S, Hannerz H, Tüchsen F, Mikkelsen KL.
Journal: Parkinsonism Relat Disord. 2009 Jan;15(1):12-4.
PMID: 18367422
In this study, the researchers looked at the medical records of everyone in Denmark (over the age of 20 years) who suffered head trauma between 1981-1993. They followed up these individuals till 2004, but they found no evidence of severe head injury among adults being a risk factor for Parkinson’s.
And that study has recently been followed by this study from Finland:

Title: Risk of hospitalization with neurodegenerative disease after moderate-to-severe traumatic brain injury in the working-age population: A retrospective cohort study using the Finnish national health registries.
Authors: Raj R, Kaprio J, Korja M, Mikkonen ED, Jousilahti P, Siironen J.
Journal: PLoS Med. 2017 Jul 5;14(7):e1002316.
PMID: 28678790 (This report is OPEN ACCESS if you would like to read it)
In this study – using the Finnish Care Register for Health Care to identify everyone in Finland between the ages of 18 and 65 years hospitalized for TBI during 1987–2014 – the researchers found that a history of moderate-to-severe TBI was associated with an increased risk for future dementia, but not for Parkinson or amyotrophic lateral sclerosis (ALS, also known as motor neuron disease).
Thus, there is some evidence against this idea of an association between TBI and Parkinson’s.
But that said, a recent meta analysis of 22 studies (19 case-control studies, 2 nested case-control studies, and 1 cohort study) found that a history of head trauma that results in concussion is associated with a higher risk of developing (Click here to read more about that study).
But if there is an association, how could this brain trauma be resulting in increased risk of Parkinson’s?
It is a real good question.
The short answer is: we really don’t know.
But there are some suggestions as to what could be occurring. For example, a study in 2011 which utilised the positron emission tomography (PET) brain scanning technique suggested that the helper cells of the brain – the microglia – remain activated in various brain areas for a long period of time after a TBI event (up to 17 years – Click here to read more about this study).
TBI may also disrupt the blood-brain barrier – the membrane that surrounds and protects the brain. Such a disruption of the barrier could expose the brain to neurotoxins or pro-inflammatory agents (Click here to read more about this study).
In addition, it has been suggested that TBI disrupts mitochondrial functioning and induces glutamate excitotoxicity, both of which are associated with neurodegeneration (Click here and here to read more about this).
And there could also be genetic reasons for an association between Parkinson’s and TBI:
Title: LRRK2 Contributes to Secondary Brain Injury Through a p38/Drosha Signaling Pathway After Traumatic Brain Injury in Rats.
Authors: Rui Q, Ni H, Gao F, Dang B, Li D, Gao R, Chen G.
Journal: Front Cell Neurosci. 2018 Mar 1;12:51.
PMID: 29545743 (This report is OPEN ACCESS if you would like to read it)
Genetic variations in the region of DNA called “Leucine-rich repeat kinase 2” (or LRRK2) can result in a hyperactive form of the LRRK2 protein, and having this version of the protein has been associated with an increased risk of Parkinson’s (Click here to read a previous SoPD post about LRRK2).
In this study, the researchers reported that administration of a LRRK2 inhibitor (called PF-06447475) which significantly reduced neuronal cell death, brain water content, and blood–brain barrier permeability 12 h after a model of TBI was induced. This treatment also reduced the neurological deficits 72 h after the TBI episode was induced.
Thus, it may be that individuals with a genetic mutation in their LRRK2 gene could be at further risk of developing Parkinson’s following a TBI episode. This suggestion needs to be more thoroughly investigated though.
So what does it all mean?
A recent analysis of medical records from members of the US military veterans association has the strongest indication of an association better traumatic brain injury and the risk of developing Parkinson’s.
It is important to remember, however, when reading all of this research is that not everyone in the Parkinson’s community has had a TBI (mild or otherwise) episode. In fact, TBI is a very rare event (a study of European incidence of TBI found 262 per 100,000 people per year get admitted to hospital each year for TBI – source). Collectively, less than 5% of the general population has probably had a significant episode of mild TBI in their lifetime. And if only 0.58% of all of those TBI cases in the US veterans study (discussed above) went on to develop Parkinson’s, it is still only a very small fraction of the overall community. Thus, having a bang on the head is not a reason to panic and assume that one is going to develop Parkinson’s. Nor is it necessarily the explanatory reason why people with Parkinson’s have the condition.
The possibility of an association, however, is still very interesting. Such knowledge is important for post TBI care, and a better understanding of the mechanisms underlying the connection may well tell us a bit about how Parkinson’s develops in certain individuals.
And for those who are interested:
Ever the coward, I never ever had the courage to offer my noggin to Billy again. And he always seemed keen for a second shot at it. He still enjoyed charging at my fist, and crazy as he was he even started challenging some of the large sheep in nearby fields.
At the end of a long summer together though, Billy went back to his herd to become a stud breeder. Six months later, I visited him and while I recognised him, it was apparent that he did not have a clue who I was me.
Perhaps it was the long term consequences of our heads colliding or maybe he just had far more important things on his mind, but Billy only gave me a passing glance before continuing on his merry way.

Feeling rejected. Source: Telco7
The ‘goat guy’ indeed. I’ll probably be explaining all of this to a shrink one day.
Lots of interesting material for them to work with, I guess.
The banner for today’s post was sourced from Craighospital

i love the anecdote about the goat
LikeLike
The ridiculous part is that it’s all true!
LikeLike
Ask Muhammad Ali.
LikeLike
Hi Gavril,
We are not sure about Ali’s situation. While he had the clinical features of PD, no autopsy was ever carried out on his body, so we will never know for sure if he had the pathological hallmarks of PD in the brain. Was trauma in his case was causative or simply additive? There has, however, been a lot of recent research focused on chronic traumatic encephalopathy (CTE) in American football players, and there was a research report last year (2017) that was quite enlightening. The researchers looked at the brains of 202 ex-footballers who had passed away and their brains had been donated to research. Histological analysis of the brains suggested that CTE was neuropathologically evident in 177 of the cases (https://jamanetwork.com/journals/jama/fullarticle/2645104) and many of these cases (62) passed away with what was described as “neurodegenerative conditions (ie, dementia-related and parkinsonian-related causes of death)”. Obviously more research is required on this topic.
Kind regards,
Simon
LikeLike