
|
This week Denali Therapeutics released the results of a phase I clinical trial of their primary product, called DNL-201. DNL-201 is a LRRK2 inhibitor that the company is attempting to take to the clinic for Parkinson’s disease. In today’s post we will look at what LRRK2 is, how an inhibitor might help in Parkinson’s, and what the results of the trial actually mean. |

Denali. Source: Wikipedia
Denali (Koyukon for “the high one”; also known as Mount McKinley) in Alaska is the highest mountain peak in North America, with a summit elevation of 20,310 feet (6,190 m) above sea level. The first verified ascent to Denali’s summit occurred on June 7, 1913, by four climbers Hudson Stuck, Harry Karstens, Walter Harper, and Robert Tatum.
Tatum (left), Karstens (middle), and Harper (right). Source: Gutenberg
Robert Tatum later commented, “The view from the top of Mount McKinley is like looking out the windows of Heaven!”
More recently another adventurous group associated with ‘Denali’ have been trying to scale lofty heights, but of a completely different sort from the mountaineering kind.

Founded in 2013 by a group of former Genentech executives, San Francisco-based Denali Therapeutics is a biotech company which is focused on developing novel therapies for people suffering from neurodegenerative diseases. Although they have product development programs for other condition (such as Amyotrophic Lateral Sclerosis and Alzheimer’s disease), Parkinson’s is their primary interest.
And their target for therapeutic effect?
The Parkinson’s-associated protein called Leucine-rich repeat kinase 2 (or LRRK2).
What is LRRK2?
Also known as ‘Dardarin‘ (from the Basque word “dardara” which means “trembling”), LRRK2 is an enzyme that has many functions within a cell – from supporting efforts to move things around inside the cell to helping to keep the power on (involved with mitochondrial function).
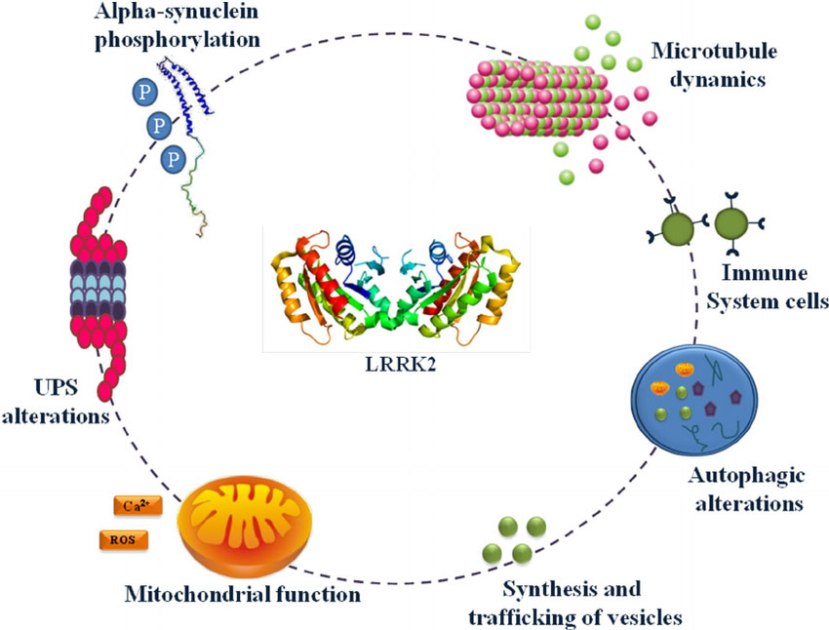
The many jobs of LRRK2. Source: Researchgate
The gene that provides the instruction for making the LRRK2 enzyme resides on the 12th chromosome, in an area of DNA referred to as ‘PARK8’ (one of the Parkinson’s disease-associated genetic regions). The LRRK2 gene is located within the PARK8 region, and it is made up of many different sections, each of which is involved with the different functions of the eventual protein.
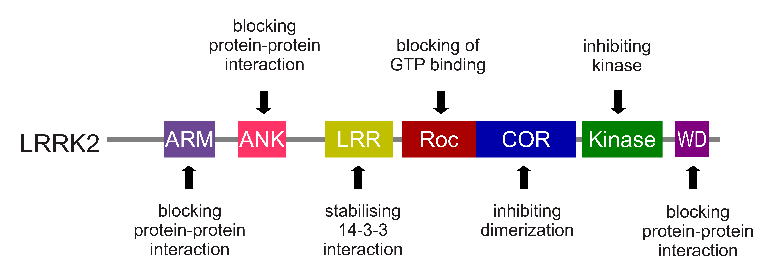
The regions and associated functions of the LRRK2 gene. Source: Intechopen
Genetic mutations within the LRRK2 gene are recognised as being some of the most common with regards to increasing ones risk of developing Parkinson’s disease (they are present in approximately 1-2% of all cases of Parkinson’s).
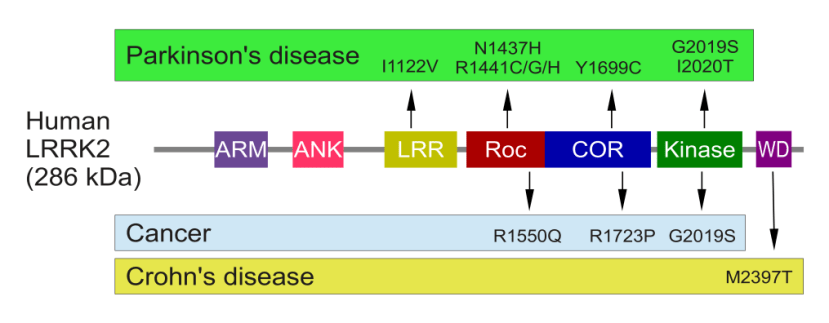
The structure of Lrrk2 and where various mutations lie. Source: Intech
As the image above suggests, mutations in the PARK8 gene are also associated with Crohn’s disease (Click here and here for more on this) – though that mutation is in a different location to those associated with Parkinson’s. And one particularly common Parkinson’s-associated LRRK2 mutation – called G2019S – is also associated with increased risk of certain types of cancer, especially for hormone-related cancer and breast cancer in women – Click here to read more about this. If you have a G2019S mutation, it is good to be aware of this association and have regular check ups.
The G2019S mutation (the name designates its location on the gene) is the most common LRRK2 mutation. In some populations of people it can be found in 40% of people with Parkinson’s (Click here to read more about this). But what is interesting about this mutation is that it gives rise to a LRRK2 enzyme that is hyperactive.
The structure of LRRK2 protein. Source: Wikipedia
As a protein, LRRK2 interacts with many different types of other proteins, and you can imagine that in a finely balanced environment like the cells that a mutant ‘hyperactive’ form of LRRK2 is going to cause problems. The consequences of this constantly active form of LRRK2 protein is believed to be the cause of cell death in LRRK2-associated Parkinson’s.
So how are Denali trying to stop this hyperactive form of LRRK2?
They are developing drugs called LRRK2 inhibitors. These are compounds that bind to the protein and prevent it was doing its job.
Their first drug, DNL-201, is a selective, orally-available, brain-penetrant, reversible small molecule LRRK2 inhibitor.
And this is the drug that they reported phase I results on this week.
What did the clinical trial involve?
A phase I clinical trial is a test of safety in humans.
In April 2017, Denali filed an investigational new drug application (or IND) with the FDA for the testing of DNL-201 in humans. They then initiated a Phase I clinical trial of the drug in healthy volunteers in the United States in June 2017. The purpose of that trial was simply to determine if the drug was safe in man.
But this trial came with an important detail.
DNL-201 was subject to a ‘partial clinical hold‘ issued by the US Food and Drug Administration (FDA). A partial clinical hold is a delay or suspension of part of the clinical work requested under the IND. In the case of DNL-201, the FDA wanted to limit the amount (or exposure) of drug that the company was initially giving to participants in the study. Often phase I clinical trials will involve the testing of gradually increasing levels of a drug to determine the levels at which the drug begins to become unsafe.
The limiting of the amount of drug in the case of DNL-201 is called an exposure cap.

Source: FDA
The FDA allowed Denali to proceed with their Phase I clinical trial in healthy volunteers at doses that they believed would sufficiently inhibit LRRK2 by 50% on average over the course of the dosing period. Denali believed that this dose was a single dose of 60mg of DNL-201.
And it should be noted that this ‘partial clinical hold’ is not a bad thing.
It is simply a precautionary step taken by the regulators.
Why are the regulators taking precautionary steps?
- Because they are regulators and if anything goes wrong they don’t want to be blamed!
- Because people are being very cautious with the development of LRRK2 inhibitors.
Why?
As I mentioned above, LRRK2 is a busy little protein that has a lot of functions inside of a cell. It has been associated with protein synthesis, mitochondrial function, apoptosis (or programmed cell death), cytoskeletal activity, and various aspects of autophagy (the waste recycling system of the cell). And thus there is justifiable concern that inhibiting this protein could have significant ‘off-target’ effects.
And during the development of DNL-201, there were some indications of this:
Title: Effect of selective LRRK2 kinase inhibition on nonhuman primate lung
Authors: Fuji RN, Flagella M, Baca M, Baptista MA, Brodbeck J, Chan BK, Fiske BK, Honigberg L, Jubb AM, Katavolos P, Lee DW, Lewin-Koh SC, Lin T, Liu X, Liu S, Lyssikatos JP, O’Mahony J, Reichelt M, Roose-Girma M, Sheng Z, Sherer T, Smith A, Solon M, Sweeney ZK, Tarrant J, Urkowitz A, Warming S, Yaylaoglu M, Zhang S, Zhu H, Estrada AA, Watts RJ.
Journal: Sci Transl Med. 2015 Feb 4;7(273):273ra15.
PMID: 25653221
In this study, the researchers wanted to determine what potential issues could be encountered by the inhibition of LRRK2. They started out by looking at where LRRK2 could be found in both humans and mice, and they found a lot of similarities. They next made a thorough analysis of mice that had no LRRK2, assessing their overall health. This analysis revealed that these LRRK mutant mice had changes in lungs and kidneys.
The investigators then sought to test a pair of LRRK2 inhibitors (called GNE-7915 and GNE-0877) that had been developed to see if they would cause similar issues in the lungs and kidneys of mice. These toxicity assessments in rodents indicated no lung or kidney changes were caused by either of the two LRRK2 inhibitors.
When the researchers next tested those same drugs in primates, they found normal kidney function, but some toxicity issues in the lungs. And these lung changes resembled the changes that the investigators had seen in the lungs of the LRRK2 mutant mice, which suggested to them that the effect was specific to LRRK2 activity.
In addition, the researchers observed reduced levels of activity and decreased reactivity to stimulus in rats that were treated with very high doses of the the inhibitors. And while these particular behavioural observations were transient (only observed between 3 to 9 hours after treatment), the FDA decided that it would cautious with the more into humans.
Hence the ‘partial clinical hold’ order.
Do we know if DNL-201 works in models of Parkinson’s?
Yes. There have been two peer-reviewed publications involving the GNE-7915 inhibitor (which I am assuming is DNL-201; there have been no follow up reports of GNE-0877).
First, in February of 2017:

Title: Effects of LRRK2 Inhibitors on Nigrostriatal Dopaminergic Neurotransmission.
Authors: Qin Q, Zhi LT, Li XT, Yue ZY, Li GZ, Zhang H.
Journal: CNS Neurosci Ther. 2017 Feb;23(2):162-173.
PMID: 27943591 (This article is OPEN ACCESS if you would like to read it)
In this study, the researchers wanted to evaluate the effects of three types of LRRK2 inhibitors (LRRK2-IN-1, GSK2578215A, andGNE-7915) on dopamine release in the brains of mice. They found that LRRK2-IN-1 decreased levels of dopamine release, while GSK2578215A and GNE-7915 did not. They next assessed the effects of the inhibitors in two mouse models of LRRK2-associated Parkinson’s (genetically engineered mice; one group contained the human LRRK2 gene with the G2019S mutation, and the other group had the human LRRK2 gene with the R1441G variant). In both mouse models, GNE-7915 was found to enhances dopamine release and improve cell function, while GSK2578215A had no effect. Thus the investigators concluded the GNE-7915 should be “validated for further therapeutic development for PD”.
And this was done in a study that was published in November 2017:
Title: LRRK2 G2019S-induced mitochondrial DNA damage is LRRK2 kinase dependent and inhibition restores mtDNA integrity in Parkinson’s disease.
Authors: Howlett EH, Jensen N, Belmonte F, Zafar F, Hu X, Kluss J, Schüle B, Kaufman BA, Greenamyre JT, Sanders LH.
Journal: Hum Mol Genet. 2017 Nov 15;26(22):4340-4351.
PMID: 28973664
In this study, the researchers wanted to assess the impact of the LRRK2 G2019S mutation has on mitochondrial DNA. You may recall from previous posts that mitochondria are small bean-shaped structures that act as the power stations of each cell. They help to keep the lights on. Without them, the party is over and the cell dies.

Mitochondria and their location in the cell. Source: NCBI
A curious feature of these little structures is that they have their own DNA – separate from the DNA in the nucleus of the cell within which they live. Damage to mitochondrial DNA can cause the mitochondria to die, and as they die so too does the cell.
The researchers found that by producing high levels of LRRK2 G2019S mutant protein, they caused increased levels of damage to mitochondrial DNA. Interestingly, they only saw this effect in dopamine neurons, and not neurons from other regions of the brain such as the cortex. By introducing high levels of normal LRRK2 protein, the investigators could not rescue the mitochondrial DNA damage.
Amazingly, treatment of the dopamine cells producing high levels of LRRK2 G2019S mutant protein with the LRRK2 inhibitor GNE-7915, either prevented or restored mitochondrial DNA damage back to normal levels. These investigators concluded by suggesting that “blocking or reversing mitochondrial DNA damage via LRRK2 inhibition or other therapeutic approaches may be useful to slow PD-associated pathology”.
And it should also be noted that none of the researchers involved in these two studies were associated with Denali Therapeutics (to my knowledge).
OK, so what were the results of the Denali Phase I study?
In June 2017, Denali Therapeutics initiated a three part Phase I clinical trial of the safety of the LRRK2 inhibitor DNL-201 in normal healthy humans.
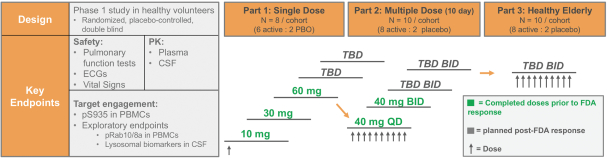
The structure of the phase I trial of DNL-201. Source: SEC
Part 1 involved a single dose per participant of the drug up to the agreed limit of 60mg (6 subjects were involved in this part). Next, Part 2 involved 8 participants receiving 2 doses of 40mg of DNL-201 10 days apart. Upon the successful completion of these parts of the study, Denali submitted a complete response to the FDA’s partial clinical hold in November 2017, requesting the FDA to lift the exposure cap and permit the company to test higher doses to achieve higher levels of LRRK2 inhibition.
This week the company reported that “DNL-201, achieved, on average, greater than 90% inhibition of LRRK2 kinase activity observed at peak” (the point at which the drug has the highest level in the blood) “and greater than 50% inhibition at trough drug levels at the highest multiple dose tested in a healthy volunteer Phase 1 study”.
LRRK2 inhibition was measured by two independent blood-based biomarker assays of LRRK2 activity (the phosphorylation of LRRK2 at Serine 935 and phosphorylation of the LRRK2 substrate Rab10). The company also reported robust penetration of the brain by the drug, as determined by levels of DNL-201 in the cerebrospinal fluid – the liquid that our brains sits in.
In addition to these results, Denali announced that “based on a full review of the clinical data from this ongoing study, and additional preclinical data, the FDA has removed the previously imposed partial clinical hold”. Thus the company is now able to move ahead with the rest of the planned Phase I clinical trial, which will include:
- testing higher single doses of DNL-201 in healthy individuals
- testing further combinations of doses of DNL-201 in healthy individuals
- testing DNL-201 in healthy elderly individuals
On top of the ongoing testing of DNL-201, Denali announced that they had submitted a Clinical Trial Authorisation (or CTA) for DNL-151 (another LRRK2 inhibitor) to the Netherlands Health Authority in October 2017 and it was accepted in November. They are now going to initiate a Phase I clinical trial of DNL-151 in parallel to the DNL-201 trial.
After completion of the Phase I clinical trials of both DNL201 and DNL151, Denali next plans to start testing one of the drugs (DNL201 or DNL151) in a Phase Ib study that will involve people with LRRK2-associated Parkinson’s.
Ok, so what does it all mean?
Genetic mutations in the LRRK2 gene are a major risk factor for Parkinson’s. In many cases of these genetic variants, the resulting LRRK2 protein is hyperactive. The cell can not handle this constantly active form of LRRK2 and it is believed that this results in the cell dying. By reducing the level of LRRK2 activity in these cells, researchers hope that they can slow down the progression of Parkinson’s.
Thus targeting the hyperactive version of LRRK2 with carefully designed inhibitors represents a promising therapeutic approach. The worry about this inhibitor idea, however, is that LRRK2 is involved with many functions and by blocking some of them, are there going to be debilitating side effects from the use of such a drug. Another question that has not been addressed in the brief results is what (if any) effect DNL-201 has had on LRRK2’s sibling LRRK1 (which we discussed in a previous post – Click here to read that post). It would be interesting (and ultimately necessary) to determine if DNL-201 is also affecting LRRK1.
In today’s post, we have looked at some recent clinical trial results which bode rather well for this class of drugs. The results do not mention anything about side effects or adverse events, so we can assume ‘So far, so good’. The company behind the trial are now going to continue on and we should see the full study results in the new year.
I will be keeping an eye out for these results and report them here.
EDITORIAL NOTE: Denali Therapeutics Inc is now a publicly traded company. That said, the material presented on this page should under no circumstances be considered financial advice. Any actions taken by the reader based on reading this material is the sole responsibility of the reader. Denali Therapeutics Inc has not requested this material to be produced, nor has the author had any contact with the company or associated parties. This post has been produced for educational purposes only.
The banner for today’s post was sourced from Denali

I am searching for clinical trials for Stage 1 PD. Was diagnosed 11/2017.
LikeLike
Hi Glenn,
Thanks for you comment – sorry to hear of your diagnosis, but well done for being proactive about it. I have a lot of respect for that kind of attitude.
The first step in deciding to take part in the clinical trial is to find out as much as you can about yourself (for example, do you have a genetic risk factor for PD). This kind of information is useful in determining which trials would be most appropriate for you. And there are currently clinical trials that are focused solely on individuals with a particular genetic variation (such as the GBA/Ambroxol trials – https://scienceofparkinsons.com/2017/04/16/an-ambroxol-update-active-in-the-brain/). The genetic analysis step should not be taken lightly though, as such information may be very difficult to absorb if there are any nasty surprises in the data. Genetic counselling is encouraged if you go down that path.
The next step depends entirely on geography. Where you are in the world may impact which trials you can partake in (some will have limited resources for compensating travel costs, and multiple visits will be required in most cases). The Michael J Fox Foundation has a very useful resource for determining which trials are near you (https://foxtrialfinder.michaeljfox.org/), as does Parkinson’s UK (https://www.parkinsons.org.uk/research/take-part-research). Beyond that, it is best to speak with your neurologist/clinician about what is locally available as they will be contacted by researchers seeking participants.
I hope this information helps.
Kind regards,
Simon
LikeLike