
|
# # # # I am very regularly asked “what would you do if you were diagnosed with Parkinson’s tomorrow?” As a research scientist I don’t really feel comfortable answering it, but I can see how it is a fair question. I have previously attempted to address it (Click here to read that post), and I point folks who do ask in the direction of that post. But a recent experience has me wanting to re-address it. In today’s post, we will revisit this idea of what would I do if I were diagnosed with Parkinson’s tomorrow? # # # # |
 Source: Newatlas
Source: Newatlas
I lost someone extremely close to me early last year.
Even more than COVID19 or anything else that occurred, that singular event defined 2021 for me personally. There was life before, and now life adjusting to being without them.
And I’m not sharing this out of any desire for sympathy – honestly, I don’t want it. Everyone has suffered hardships over the last 2 years. Rather, I am telling you this for a very different reason.
It helps to set the context for the discussion today.
While their passing was a shocking sudden loss, it opened up the Pandora’s box of an unrecognised elderly care situation which became my responsibility. While the local community care workers have been wonderfully supportive, the situation has quickly developed into an all consuming part of my life.
It has been a roller-coaster ride, but the experience has provided valuable insights into aspects of life that I had previously been blind to. In particular, it has directly exposed me to the incredible everyday challenges facing the aged population in a frightening technological world (banks, in particular, seem to now run on IT systems developed by 20-somethings and designed solely for the purpose of screwing over their peers while utterly baffling many of the aged population).
In addition to life in general, the journey of the last 10 months has also had a major impact on how I view our approach to treating conditions generally associated with aging, like Alzheimer’s and Parkinson’s. And this shift in my thinking has occurred with a backdrop of the “statistical gymnastics and PR maneuvering” of the aducanumab/Aduhelm situation, which has by itself seemingly polarised efforts to pharmacologically alter the course of neurodegenerative conditions (Click here to read a SoPD post about that topic).
While I think that the future is very bright for drug treatments aimed at impacting the course of these conditions (this opinion is based on the continuous flow of new insights into their under lying biology), my recent experience has really hammered home to me the idea that more is required more immediately for individuals afflicted by these conditions. While the science and research described on this website is fascinating and exciting, I can appreciated that the tangible benefits of much of it still feel remote for most readers. And in some of those cases one has to ask if they are worth waiting for if the benefits are seemingly minor (as is the current situation with Aduhelm).
 The memory test data from ‘study 1’ of Aduhelm. Source: FDA
The memory test data from ‘study 1’ of Aduhelm. Source: FDA
In short: We have focused too much emphasis on the SoPD on small molecules that take too long to reach the patient community.
A prominent PD advocate recently told me that “a faster and much less expensive route to patients for DMTs” (disease modifying therapies) is required. And I wholeheartedly agree. But perhaps we should be looking beyond small molecule-based therapies and taking a more wholistic (I really hate that word) view.
So my thinking has shifted back to basics.
Not basic biology, but rather basic care.
What do you mean ‘basic care’?
As we age, lots of stuff happens to our bodies that we don’t immediately notice. There are many “stealthy and rotten subtractions“, to quote Stephen King (Source) occurring right under our noses unbeknownst to us.
Take skin as an example.
Yes, we see the wrinkles, but we don’t really notice that our skin actually thins as we age. Yes, it becomes less elastic and more fragile, but have you ever noticed that there is less fatty tissue just below the surface?
 Me in the morning vs evening. Source: Youtube
Me in the morning vs evening. Source: Youtube
Like a vintage car, as we age we require more care and maintenance. And we need to acknowledge this. We need to look after ourselves better in order to function optimally. Left alone, an old car will corrode and deteriorate.
 Just requires a little effort. Source: Eastendbodyshop
Just requires a little effort. Source: Eastendbodyshop
So if we need to take better care of ourselves, where do we begin?.
An easy place to start is nutrition, and investigating the idea of food as medicine.
What do you mean ‘food as medicine’?
In 1601, Captain Admiral James Lancaster conducted a remarkable (and completely unethical) experiment on the unwitting crew members of the four ships under his command.
 Capt. James Lancaster. Source: Medicineatmichigan
Capt. James Lancaster. Source: Medicineatmichigan
His fleet departed Torbay in southwest England on the 21st of April, and by the time they arrived in South Africa on 9th September, three of the ships were so sick with scurvy that the men of Lancaster’s own vessel – “Red Dragon” – had to help sail the other boats into harbour. And I mean really sick – approximately 40% of the sailors on the other three ships died.
And yet curiously no one on Lancaster’s own boat had succumbed.
How was this possible?
Answer: Every morning of the voyage, the crew of Red Dragon were given three spoonfuls of bottled lemon juice. The solution is full of lots of useful dietary components, but for scurvy in particular, lemon juice has high levels of vitamin C (ascorbic acid).
Upon return to England, the Admiralty received a full report of Lancaster’s experiment,…
…but it wasn’t until 1795 (nearly 200 years and countless, unnecessary deaths later) that the Admiralty finally decided to mandate lemon juice for all of its sailors.
There are innumerable stories like this in medical history. The modern pharmacological age of medicine basically began with the administering of particular foods to alleviate certain ailments. Efforts were then made to zero in on a particular factor that caused the effect, which could be packaged and delivered (for profit) to improve the quality of life for patients.
While we wait for perfect pills, it seems to me that a lot can be learnt from going back to basics and investigate the disease modifying potential of certain foods. We have previously discussed broccoli as one potential option (Click here to read that old SoPD post). It would be interesting to explore the idea of a broccoli (or cruciferous vegetables) clinical trial.
What are cruciferous vegetables?
Cruciferous vegetables are vegetables of the Brassicaceae family (also called Cruciferae). They are a family of flowering plants commonly known as the mustards, the crucifers, or simply the cabbage family. They include cauliflower, cabbage, garden cress, bok choy, broccoli, brussels sprouts and similar green leaf vegetables.

Cruciferous vegetables. Source: Thetherapyshare
So what have Cruciferous vegetables got to do with Parkinson’s?
Well, it’s not the vegetables as such that are important. Rather, it is a particular chemical that this family of plants share – called Glucoraphanin – that is key.
What is Glucoraphanin?
Glucoraphanin is a glucosinolate.
Glucosinolates are a naturally occurring class of organic compounds that contain both sulfur and nitrogen. They are derived from glucose and an amino acid. You know that pungent smell that fills the kitchen when you are cooking cabbage or brussels sprouts? This is partly due to the release of glucosinolates from the vegetables being cooked.
Cruciferous plants release glucosinolates when they are attacked or damaged (or steamed/boiled). These glucosinolates are rapidly released when the plant tissue senses danger: freezing or boiling cruciferous plants for 10 minutes reduces glucosinolate concentrations by about 50%. Glucosinolates are believed to be part of a plant’s defence system against pests and diseases.
And being a glucosinolate, Glucoraphanin is one component of this defence system.
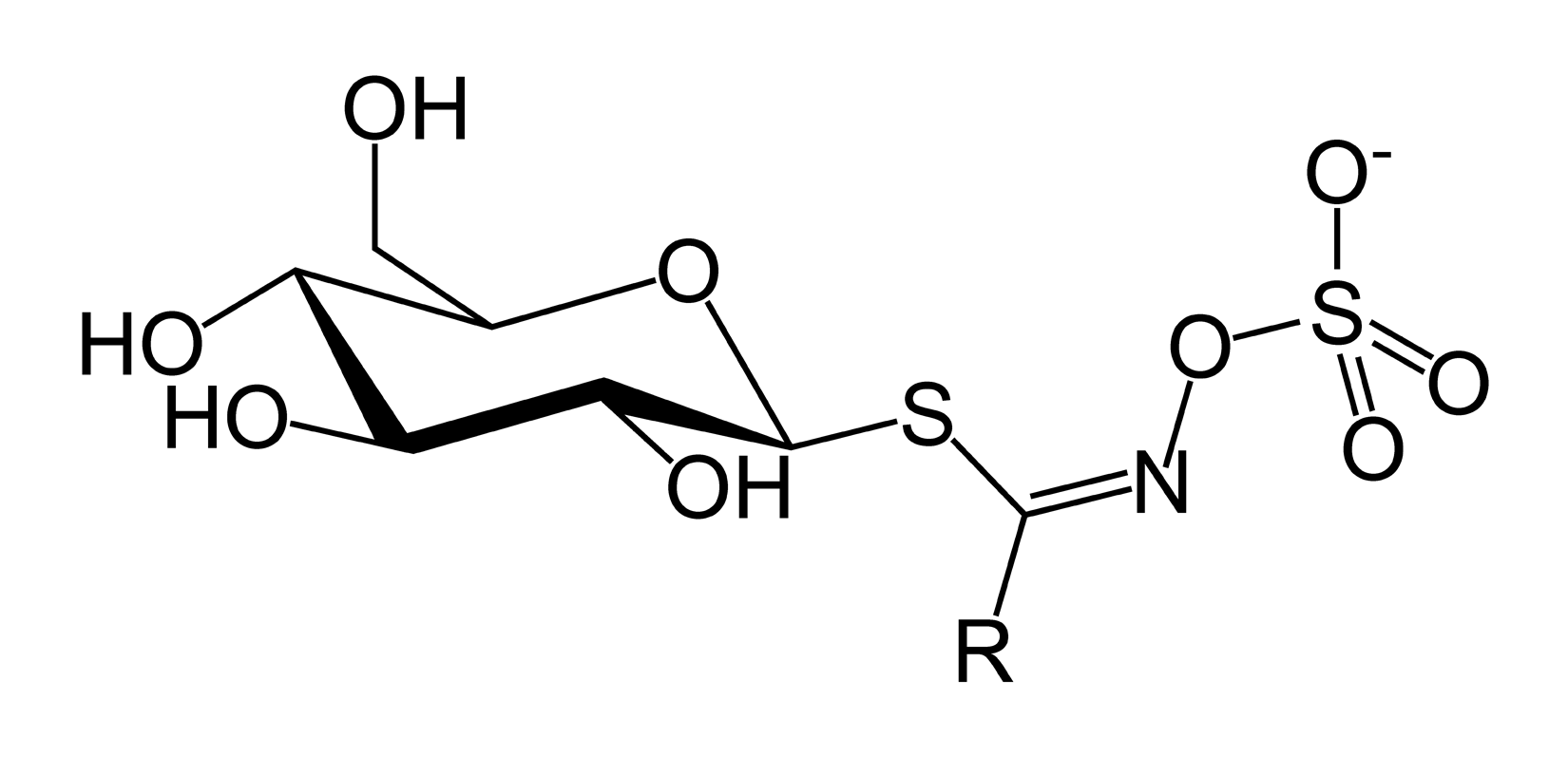
The structure of Glucoraphanin. Source: Wikipedia
When cruciferous vegetables are consumed, an enzyme called myrosinase transforms glucoraphanin into raphanin and sulforaphane. Raphanin is useful in that it inhibits activity of viruses, some fungi and various bacteria. A general anti-bacterial/viral agent.
And what about sulforaphane?
Sulforaphane is what I would like to focus on in this post, because it is something of a miracle worker.
Above all else, it is a potent activator of the NRF2 pathway.
What is NRF2?
Nuclear Factor Erythroid 2-Related Factor 2 (or NRF2) is a ‘transcription factor’, which is a protein that is involved in the process of converting DNA into RNA (an event called transcription) .
You may remember from your high school science class one of the central dogmas of biology: DNA gives rise to RNA, RNA gives rise to protein. Transcription is the process of making RNA.

The basic of biology. Source: Youtube
Now, a transcription factor can be an ‘activator’ of transcription – that is, it initiates or helps the process of generating RNA from DNA.

An example of a transcriptional activator. Source: Khan Academy
Or it can be a repressor of transcription – blocking the machinery (required for generating RNA) from doing its work.

An example of a transcriptional repressor. Source: Khan Academy
NRF2 is an activator of transcription. When it binds to DNA to aids in the production of RNA, which then results in specific proteins being produced.
And this is where NRF2 gets REALLY interesting.
You see, NRF2 binds to antioxidant response elements (ARE).
What are ARE?
Antioxidant response elements (ARE) are regions of DNA commonly found in the regulatory area of genes encoding powerful antioxidant and protective proteins (if you are wondering what antioxidants are – click here).
The regulatory region of a gene is the section of DNA where transcription is initiated. They are pieces of DNA that a transcription factor – like NRF2 – attach to and activates the production of RNA.
Given that these antioxidants and protective genes are generally considered a good thing for sick/dying cells (and that NRF2 is known to activate more than 200 of them), you can see why NRF2 is an interesting protein to investigate.
Source: NRF2 science
By binding to ARE, NRF2 is directly encouraging the production of naturally occurring antioxidant and protective proteins. And this is why a lot of people are excited about NRF2.
It is also why I am interested in sulforaphane: it is a naturally-occurring, potent activator of NRF2.
And broccoli have high levels of sulforaphane?
No, broccoli have high levels of glucoraphanin which is converted into sulforaphane (see above). Broccoli has approximately 44-170 mg of glucoraphanin for every 100g of dry weight.
Even more impressive are broccoli sprouts, which have 1100 mg of glucoraphanin for every 100g of dry weight.

Brocolli sprouts. Source: Organiclifestylemagazine
Perhaps a broccoli sprout clinical trial is the better way to go. But it has to be acknowledged that taking broccoli or broccoli sprouts into clinical studies is no easy task. They are not easy clinical studies to design and conduct. Careful consideration has to be given to how such studies are structured (beyond the simple fact that not everyone likes broccoli! Imagine measures of ‘quality of life’ for some who hates broccoli if they are asked to eat 2 pounds of the stuff per day!). Placebo groups in such studies are very difficult to manage.
A very good review on a related topic has recently been published and worth reading:
 Title: The Challenges of Designing and Implementing Clinical Trials With Broccoli Sprouts… and Turning Evidence Into Public Health Action.
Title: The Challenges of Designing and Implementing Clinical Trials With Broccoli Sprouts… and Turning Evidence Into Public Health Action.
Authors: Fahey JW, Kensler TW.
Journal: Front Nutr. 2021 Apr 29;8:648788.
PMID: 33996874 (This report is OPEN ACCESS if you would like to read it)
All of this said, I am unaware of any clinical studies that have investigated the potential of broccoli or related foods on Parkinson’s (and I’d be happy to be corrected on this).
A similar situation applies to things like cod liver oil.
 Cod liver oil. Source: MNT
Cod liver oil. Source: MNT
A strong case of support could be made for clinical testing of cod liver oil in Parkinson’s – it “contains large amounts of vitamins A, D, and omega-3 fatty acids, and the health benefits may go beyond rheumatism and rickets” (Source).
Why haven’t these things been investigated?
The simple answer is: ¯\_(ツ)_/¯
But we will be exploring this ‘food as medicine’ theme on the SoPD in 2022.
My point in today’s post is: As we age we all need to take better care of ourselves. Seek help from others – yes – but start with basics and identify where improvements can be made in your own life. Food is a good starting point. Most of us think that we are reasonably healthy in our nutritional intake, but much of the general population struggle to eat 5 fruit/veg (a minimum of 400g) per day (and potatoes do not count – Source).
And this is really a crying shame that there is not more research on this because the studies to date have demonstrated that fruit and vegetable intake is associated with reduced risk of all-cause mortality:
 Title: Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies.
Title: Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies.
Authors: Aune D, Giovannucci E, Boffetta P, Fadnes LT, Keum N, Norat T, Greenwood DC, Riboli E, Vatten LJ, Tonstad S.
Journal: Int J Epidemiol. 2017 Jun 1;46(3):1029-1056.
PMID: 28338764 (This report is OPEN ACCESS if you would like to read it)
And very similar results have been reported by other large studies:
 Title: Fruit, vegetable, and legume intake, and cardiovascular disease and deaths in 18 countries (PURE): a prospective cohort study.
Title: Fruit, vegetable, and legume intake, and cardiovascular disease and deaths in 18 countries (PURE): a prospective cohort study.
Authors: Miller V, Mente A, Dehghan M, Rangarajan S, Zhang X, Swaminathan S, Dagenais G, Gupta R, Mohan V, Lear S, Bangdiwala SI, Schutte AE, Wentzel-Viljoen E, Avezum A, Altuntas Y, Yusoff K, Ismail N, Peer N, Chifamba J, Diaz R, Rahman O, Mohammadifard N, Lana F, Zatonska K, Wielgosz A, Yusufali A, Iqbal R, Lopez-Jaramillo P, Khatib R, Rosengren A, Kutty VR, Li W, Liu J, Liu X, Yin L, Teo K, Anand S, Yusuf S; Prospective Urban Rural Epidemiology (PURE) study investigators.
Journal: Lancet. 2017 Nov 4;390(10107):2037-2049.
PMID: 28864331 (This report is OPEN ACCESS if you would like to read it)
The authors of this report acknowledge that 400g/day “may have important implications on household spending and food security in poorer countries“, but even modest efforts may have benefits.
But why is nutrition important for Parkinson’s?
This is Dr Laurie Mischley:

Source: Bastyr
She’s awesome. She is an Associate Clinical Investigator at Bastyr University, a guru when it comes to nutrition, and my first port of call when we field questions regarding Parkinson’s and nutrition.
You can see her in action in this video (recommended viewing for those with Parkinson’s and interested in the topic of diet/nutrition):
Dr Mischley also co-ordinates the “Complementary & Alternative Medicine Care in Parkinson’s Disease” (CAM Care in PD) study, which is attempting to ‘collect as much data as possible over a five-year period with the hope of finding dietary and lifestyle factors associated with a slower disease progression’ (Click here to learn more about it).
This CAM study has borne fruit that may be of real interest to the Parkinson’s community. It is a research report that reviews dietary and nutritional supplemental factors that can impact Parkinson’s progression.
This is the study here:
Title: Role of Diet and Nutritional Supplements in Parkinson’s Disease Progression
Authors: Laurie K. Mischley, Richard C. Lau, Rachel D. Bennett
Journal: Oxidative Medicine and Cellular Longevity, 2017, 6405278.
PMID: 29081890 (This article is OPEN ACCESS if you would like to read it)
In this study, 1307 people with Parkinsonisms signed up to the CAM Care in PD study and filled in the survey. Of these 1053 were identified as having a diagnosis of idiopathic Parkinson’s – that is, Parkinson’s that has arisen spontaneously and is not attributable to any known factor (genetics or otherwise). The data from these individuals was used in the analysis of this publication.
The average age of study participants was 63 years, and they had an average 5.2 years since diagnosis. Interestingly, more females (53%) enrolled in the study than males, and the vast majority of the subjects were of a Caucasian background (Click here to see all of the demographics of the sample population).
The survey used a self-assessment tool, called the ‘patient-reported outcomes in PD’ (PRO-PD), to assess the severity of the Parkinson’s in each participant. This survey consists of 33 common Parkinson’s related symptoms (such as tremor, sense of smell, etc), and required the participant to simply move a marker on a slide bar according to severity (the left side of the bar always representing no problems, and the right side of the bar always representing the highest level of severity.

How reliable are the results of a ‘self-assessed’ survey by people with Parkinson’s?
It’s a fair question.
One that Dr Mischley and her colleagues have already addressed in a comparison study. The results of the PRO-PD survey were compared with clinical measures made by clinicians and a report of the study was published:

Title:Use of a self-rating scale of the nature and severity of symptoms in Parkinson’s Disease (PRO-PD): Correlation with quality of life and existing scales of disease severity.
Authors: Mischley LK, Lau RC, Weiss NS.
Journal: NPJ Parkinsons Dis. 2017 Jun 16;3:20.
PMID: 28649620 (This article is OPEN ACCESS if you would like to read it)
In this comparative study, the investigators asked 58 people with Parkinson’s (who were involved in ongoing clinical trials), to fill in the PRO-PD survey. The researchers next compared the self-assessed results of the PRO-PD survey with the results determined in the clinical setting by clinicians. They found that the PRO-PD self assessed survey was highly correlated not only with patient-reported quality of life measures (such as the Parkinson’s Disease Questionaire-39), but also with clinician assessed measures (such as Hoehn & Yahr, and the Unified Parkinson’s disease Rating Scale (UPDRS). This result suggests that the PRO-PD survey can be reliably used in determining disease severity in online studies.
Ok, so what else did the investigators ask survey participants about in the diet study?
After the questions of disease severity, the survey moves on to a long list of life style questions, which deals with everything from dietary supplements to how far one lives from a highway. It is very thorough.
All of this information has been collected and analysed, and in this new research report Dr Mischley and her colleagues turned their focus on the dietary and nutritional data in the survey.
When looking at types of foods that were associated with a faster progression of Parkinson’s symptoms (that is, the disease getting worse), the investigators found that:
- fresh vegetables
- fresh fruit
- nuts and seeds
- fish
- olive oil
- wine
- coconut oil
- fresh herbs
- the use of spices
were all associated with significantly lower rates of disease progression (meaning a slower progression of the condition), while:
- Canned fruit
- Diet soda (carbonated drinks)
- Canned vegetables
- Fried food
- Beef
- Soda (carbonated drinks)
were all associated with significantly increased rates of disease progression (that is, the condition was getting worse as a result of consuming these foods).
In addition, ice cream, yogurt and cheese were also associated with increased rates of disease progression (although this was not significant). To see the full list of foods, please click here. We have previously discussed on this website the association between Parkinson’s and dairy products (milk in particular – click here to read that post) and will be exploring it again in an upcoming post.
But soda (or carbonated drinks) is a new one for me.

Soda drinks. Source: Secretlyhealthy
The study particularly points towards diet soda (as opposed to normal soda) as being a bad influence.
Why would this be?
Diet soda contains artificial sweetners, such aspartame. This sweetener (also known as NutraSweet) is converted in the gut into phenylalanine (pronounced ‘feen ill Alah neen’), which is known to compete with Levodopa for absorption into the brain and can interfere with dopamine processing . Short term treatment of aspartame in a clinical setting does not appear to have much impact on levodopa-treated Parkinson’s (Click here to read more about this), but perhaps the long term consumption of aspartame could be having a bad influence.
While high levels of aspartame do not appear to affect the production of dopamine per se (Click here and here to read more about this), it does seem to affect the way dopamine is used. When dopamine neurons are stimulated in the presence of aspartame, the release of dopamine is reduced (Click here and here to read more about this).
Alternatively, there may be some other ingredient in diet soda that could be having the negative influence. Obviously, more research is needed on this topic – particularly given the high volumes of soda being consumed by western societies (that said, my Friday night rum and coke may have to become a thing of the past – from now on it’ll just be a Friday night rum).
What’s the beef about beef? Is this the first time anyone has reported an association between red meat and Parkinson’s?

Beef. Source: Certifiedangusbeef
No.
It is not the first time red meat has been implicated as a negative influence on Parkinson’s.
For example, this report was published in 2007:

Title: Prospective study of dietary pattern and risk of Parkinson disease.
Authors: Gao X, Chen H, Fung TT, Logroscino G, Schwarzschild MA, Hu FB, Ascherio A.
Journal: Am J Clin Nutr. 2007 Nov;86(5):1486-94.
PMID: 17991663 (This article is OPEN ACCESS if you would like to read it)
In this study looked at the long term lifestyles of 49 692 men and 81 676 women. The data of all of these individuals was collected as part of the Nurses’ Health Study (NHS) and the Health Professionals Follow-Up Study (HPFS).
The NHS study was started in 1976 when 121,700 female registered nurses (aged 30 to 55 years) completed a mailed questionnaire. They provided an overview of their medical histories and health-related behaviours. The HPFS study was established in 1986, when 51,529 male health professionals (40 to 75 years) responded to a similar questionnaire. Both the NHS and the HPFS send out follow-up questionnaires every 2 years.
All of these individuals were free of Parkinson’s at the start of these studies, but 508 were diagnosed with Parkinson’s during the 16 years of follow-up. A high intake of fruit, vegetables, legumes, whole grains, nuts, fish, and poultry was associated with a lower risk of developing Parkinson’s, while a “Western diet” of red meats, processed meats, refined grains, French fries, desserts and sweets, and high-fat dairy products was associated with an increased risk of developing Parkinson’s.
Interestingly, of all the nutritional supplements investigated in the study only coenzyme Q10 and fish oil were associated with statistically significant reduced rates of Parkinson’s progression, and it should be noted that the association between coenzyme Q10 and Parkinson’s progression disappeared after the data was adjusting for income.
Coenzyme Q10 is an antioxidant (Click here to read more about antioxidants). It exhibited positive preclinical results in models of Parkinson’s, and this led to several large clinical trials. All of those trials have yet to show any dramatic impact on the progression of the condition (Click here to read more about one example of one of those studies).
Interesting, but are people with Parkinson’s malnourished?
Obviously it depends on a case by case basis, but one report published in 2018 indicated that “67.7% of our patients had an abnormal nutritional status” and they found that higher scores on measures like the UPDRS “were determined to be related to a poorer nutritional status” (Click here to read this report). Not a direct causal effect, but definitely an association that indicates that good nutrition is important.
And another reason that diet is important in aging populations is that it can have important implications for muscle and bone density, which can impact outcomes in terms of falls and mobility.- which are rather important matters for the Parkinson’s community.
So yeah, if I was diagnosed with Parkinson’s tomorrow, my diet would change some what based on some of the research discussed in this post.
So what does it all mean?
Everyone knows that eating well is important for our health and well being, but there is limited information about which foods are good for specific ailments, like Parkinson’s. For my ward, I take fruit and soups every time I visit and make sure that the fridge is stocked with fresh food. I do not expect to hold back the tide, but comfort, happiness and well being are the primary objectives.
I am shocked by the lack of research into nutrition for neurodegenerative conditions. And I am disturbed by the idea that perhaps there are some foods that are better for certain types of Parkinson’s (such as GBA-associated PD) compared to other forms of the condition (LRRK2-associated PD). And yet we simply don’t know.
As I said above, nutrition will be a theme here on the SoPD for 2022 so expect more content looking at this topic. I will be looking out for new research on this matter as the year progresses. Please share anything you find that might be of interest in the comments section below, or else contact me directly.
# # # #
“This is the true joy in life, being used for a purpose recognized by yourself as a mighty one; being a force of nature instead of a feverish selfish clod of ailments and grievances complaining that the world will not devote itself to making you happy. I am of the opinion that my life belongs to the whole community, and as long as I live it is my privilege to do for it whatever I can. I want to be thoroughly used up when I die, for the harder I work, the more I love. I rejoice in life for its own sake. Life is no ‘brief candle’ to me. It is sort of a splendid torch which I have a hold of for the moment, and I want to make it burn as brightly as possible before handing it over to future generations.” – George Bernard Shaw
 GBS. Source: Beforeimarry
GBS. Source: Beforeimarry
For TS
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
The banner for today’s post was sourced from steemit

Written not without cost and passion. A remarkable post!
LikeLike
Sporadic age-related PD is absent in rural Kenya. A powerful argument can be made that absence of sunlight on skin is the missing environmental factor in sPD. “Vitamin”D3 signalling impacts several hundred genes that promote anti-oxidant pathways (inc Nrf2), anti-inflammation, antagonism of asyn aggregation, and so forth. Most populations globally are badly deficient in D3, the ancestral physiological level being defined by natural-living Maassai and Hadza peoples. However there is no profit in D3.
LikeLiked by 1 person
Oh my gosh I cannot begin to tell you the excitement I felt reading this this morning. Since my diagnosis I’ve been following your great blog and constantly lamented “Why is diet rarely addressed? My family will testify to my constant rant out aloud while I ploughed through science articles. As interesting as they were my instincts kept telling me that the kilos of food that we consume must have a huge impact. Hooray, please please keep exploring this topic.
LikeLiked by 1 person
And here is Terry Wahls (MD), presenting her latest research on modifiable lifestyle factors (food being a major one) which assist in arresting and reversing neurodegeneration. Her focus is on multiple sclerosis (MS) but quite applicable to Parkinson’s (PD)
LikeLike
Isn’t the World Wide Web a wonderful resource.
Thank you very much for this contribution Kenneth. Off to buy more vegetables!
Cheers,
Barbara
LikeLiked by 1 person