
|
# # # # BEFORE WE START: There are some topics that I am reluctant to address on this website, because there are folks within the community who have extremely vested interests in them. Thiamine (or Vitamin B1) is one of those topics. Some members of the Parkinson’s community have indicated to me that high doses of this vitamin are helping them. If you are one of those people, I say ‘Wonderful! Do what works for you”. To stem the endless flow of emails asking for thoughts on high dose thiamine, however, I am writing this post to outline what research has been done on this topic in the Parkinson’s field. If you are looking for answers on thiamine, you may be disappointed. I am doing this to be able to point all future inquires towards it. That said, let’s begin: In today’s post, we will delve into what thiamine (or vitamin B1) is and what it does in the body, how it relates to Parkinson’s, and we will discuss what clinical research exists for supporting its use as a treatment for PD. # # # # |
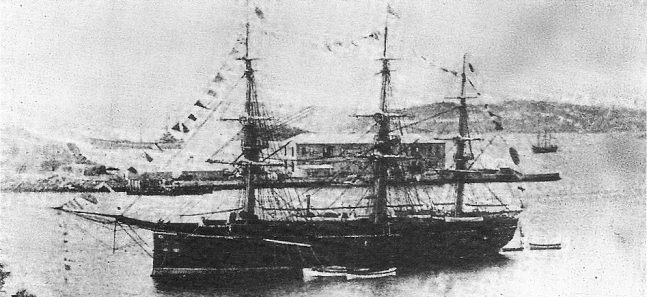 The Ryūjō. Source: Wikipedia
The Ryūjō. Source: Wikipedia
On December 19th 1882, the Japanese Naval training ship Ryujo (“Prancing Dragon”) set sail from Shinagawa, Japan, and over the next 10 months it called in at New Zealand (yay!), Chile, and Peru.
During this routine training voyage, however, 169 members of a crew of 376 crew became very sick.
That’s almost half (45%) of the crew.
In fact, the situation on board the boat got so bad that they had to stop in Hawaii on the homeward leg, because too many of the crew were sick to continue the voyage. Sadly by the time they returned to Japan in October 1883, there were 25 less members of the crew as a result of death due to sickness (and remember this was just a training voyage).
What was the sickness?
The men were suffering from a condition called beriberi.
What is beriberi?
Beriberi comes from a Sinhalese phrase which translates to “weak, weak” or “I cannot, I cannot“. There are two forms of the condition: ‘wet’ beriberi and ‘dry’ beriberi. Wet beriberi involves a fast heart rate, shortness of breath, and leg swelling. Dry beriberi is characterised by numbness of the hands and feet, confusion, trouble moving the legs, and pain. It is often said that ‘Wet’ involves the heart and ‘Dry’ involves the brain.
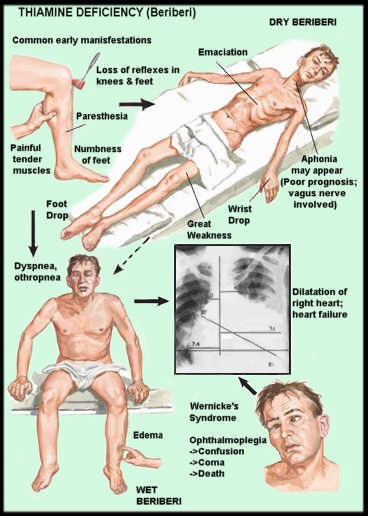
Source: Pinterest
Both forms of the condition, however, are caused by a deficiency in vitamin B1 – also known as thiamine.
What is Vitamin B1?
Vitamins are organic molecules that are essential micronutrients that organisms need in small quantities to function properly.
Vitamin B1/thiamine (aka thiamin) is one of the eight B vitamins. It is found in foods such as cereals, whole grains, meat, nuts, beans, and peas.

Source: myhealthincheck
All organisms need thiamine, but here’s the thing: It is made only in bacteria, fungi, and plants. And as a result animals (including us humans) must obtain it from their diet – hence the term ‘essential micronutrient‘.
The recommended daily intake for adults over the age of 18 years is 1.2 mg/day for men and 1.1 mg/day for women. Thiamine can only be stored in the body (typically in the liver) for short periods of time before it is excreted, so a regular dietary intake of thiamine is necessary to maintain proper blood levels.
Once thiamine is absorbed through the lining of the gut and into the blood, an enzyme called thiamine diphosphotransferase converts it into thiamine pyrophosphate (or TPP).
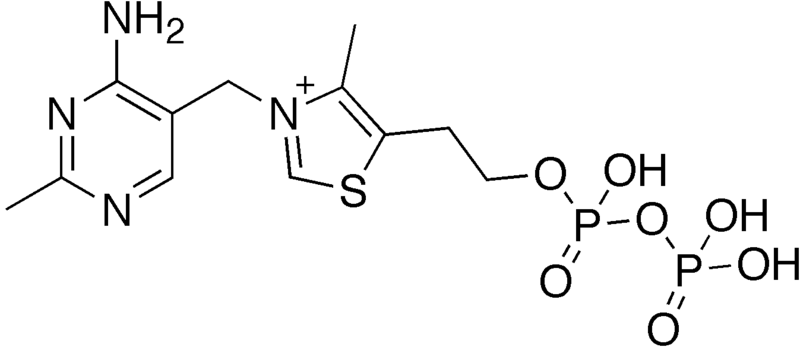 TPP. Source: Wikipedia
TPP. Source: Wikipedia
TPP is the active form of thiamine and it is involved in many important biological functions. Chief among these is energy metabolism, cell viability, and proper neuronal functioning. Crucially, TPP is a cofactor in the production of adenosine triphosphate (ATP) – this is the fuel that cells run on (Click here to read a previous SoPD post discussing ATP).
Got it. Vitamin B1 is important. So what happened to the Japanese sailors?
Well, after the stop over in Hawaii (on their homeward journey) something miraculous occurred: After taking on fresh meat and vegetables, all of the sailors who had been ill upon arrival in Hawaii made a full recovery.
And this is where we need to introduce Takaki Kanehiro:
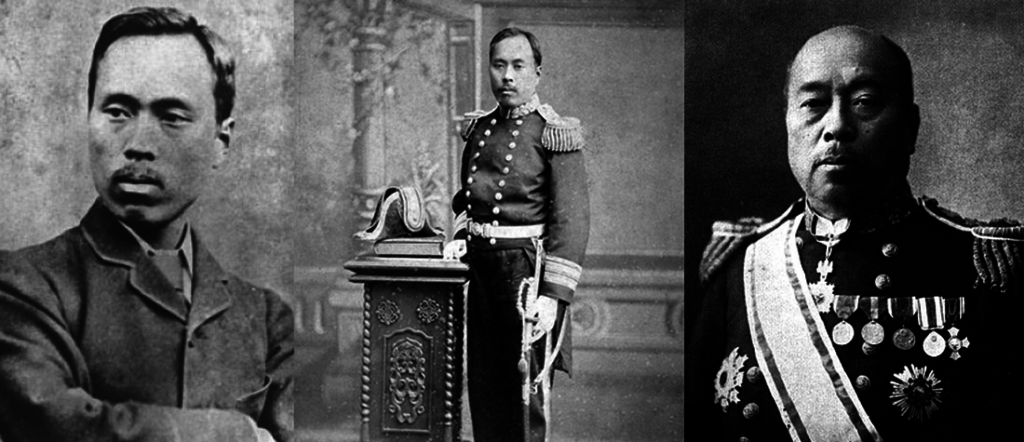
Takaki Kanehiro. Source: Warisboring
Noting the experience of the crew of the Ryujo, Takaki Kanehiro – a British-trained medical officer in the Japanese Navy – asked his superiors if they were prepared to do a little experiment.
Another training ship – the Tsukuba – was about to leave Shinagawa, bound for Hawaii, Russia and Korea before returning home. Takaki asked if they could make the exact same training voyage as the Ryujo instead, but this time there was one subtle difference: The crew were given a diet containing more variety (basically a much lower percentage of polished rice).
 The Tsukuba. Source: Wikipedia
The Tsukuba. Source: Wikipedia
By the end of their protein-rich voyage, there had been only 14 cases of beriberi and no deaths among the crew of 300+ on the Tsukuba – a significant improvement on the previous journey.
Takaki and the Navy were convinced by this result that diet was the key factor and they performed several more experiments which further verified this outcome. They did not realise it at the time – because vitamin B1 was not actually discovered until 1897 – but vitamin B1 was an important contributing factor to the success of their experiment.
Interesting history lesson, but what does vitamin B1/thiamine have to do with Parkinson’s?
Here at SoPD HQ, we get a fairly steady flow of email correspondence asking about about Dr Antonio Costantini and high dose thiamine.
 Dr Antonio Costantini. Source: Highdosethiamine
Dr Antonio Costantini. Source: Highdosethiamine
Dr Costantini was a neurologist in Viterbo, Italy with his own practice.
Since 2011, Dr Costantini and colleagues have been experimenting with the administration of high dose thiamine as a treatment for a range of medical conditions.
They started with fatigue related to inflammatory bowel disease, administering thiamine (dosage ranged from 600 mg/day (for a 60 kg person) to 1,500 mg/day (for a 90 kg person)) to 8 individuals with ulcerative colitis and 4 people affected by Crohn’s disease:
 Title: Thiamine and fatigue in inflammatory bowel diseases: an open-label pilot study.
Title: Thiamine and fatigue in inflammatory bowel diseases: an open-label pilot study.
Authors: Costantini A, Pala MI.
Journal: J Altern Complement Med. 2013 Aug;19(8):704-8.
PMID: 23379830
In this study, the investigators found that 10 of the 12 participants showed complete regression of their fatigue, while the remaining two individuals exhibited near complete regression of fatigue (compared to their fatigue scores before the thiamine therapy).
The researchers then published five additional papers in 2013 – all investigating thiamine therapy – in spinocerebellar ataxia type 2, for symptoms of fibromyalgia, Friedreich’s ataxia, multiple sclerosis, and Parkinson’s (which we will get to in a moment).
To date (and please correct me if I am wrong here), all of the studies that they have conducted have been “open label” – this means that everyone involved in the study knew who was getting treated and what they were being treated with. With no blinding or controls, such experiments can be at risk of having ‘placebo responses’ (a treatment effect that has no biological explanation).
I have never had any correspondence with Dr Costantini, and unfortunately he sadly passed away in 2020 from COVID while recovering from a post-surgery stroke (Source).
To his credit, Dr Costantini never patented the therapy or overtly promoted it – rather letting ‘word of mouth’ spread news of its utility. The clinic he worked out of does have a webpage that provides information about the treatment (Click here to see their website). There are numerous videos online – the one below has been provided by one of his collaborators:
I think it is important to repeat here that these studies are all open label in nature and in the video above Dr Colangeli does acknowledge that proper randomised, double blind, placebo-controlled clinical trials are required – and there is a Gofundme webpage trying to raise funds for this purpose.
|
# RECAP #1: Vitamin B1 (also known as thiamine) is an essential micronutrient. It is necessary for the production of energy inside of cells, but it must be attained via diet because our bodies do not naturally make it. A deficiency in thiamine results in a condition called Beriberi which used to be a problem for sailors on long voyages living on poor diets. # |
Is there any kind of thiamine deficiency associated with Parkinson’s?
Previous research has indicated some associations between cognitive issues and thiamine deficiency in ageing populations:
 Title: Role of dietary protein and thiamine intakes on cognitive function in healthy older people: a systematic review.
Title: Role of dietary protein and thiamine intakes on cognitive function in healthy older people: a systematic review.
Authors: Koh F, Charlton K, Walton K, McMahon AT.
Journal: Nutrients. 2015 Apr 2;7(4):2415-39.
PMID: 25849949 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers conducted a systematic review of the literature (2987 studies) and found that the “evidence supporting an association between higher protein and/or thiamine intakes and better cognitive function is weak”
Other studies have investigated thiamine levels in the blood and cerebrospinal fluid (the liquid surrounding our brains) from people living with neurodegenerative conditions, and these have found differing results.
For example:
 Title: Plasma thiamine deficiency associated with Alzheimer’s disease but not Parkinson’s disease.
Title: Plasma thiamine deficiency associated with Alzheimer’s disease but not Parkinson’s disease.
Authors: Gold M, Hauser RA, Chen MF.
Journal: Metab Brain Dis. 1998 Mar;13(1):43-53.
PMID: 9570639
In this study, the researchers found that individuals with Alzheimer’s had significantly lower blood thiamine levels than PD patients. In fact, there was a significantly higher number of Alzheimer’s patients with thiamine deficiencies compared to the Parkinson’s cohort.
Another study focused solely on PD has reported a subtle lowering of thiamine levels, but this was not associated with any specific characteristics:
 Title: Cerebrospinal fluid levels of thiamine in patients with Parkinson’s disease.
Title: Cerebrospinal fluid levels of thiamine in patients with Parkinson’s disease.
Authors: Jiménez-Jiménez FJ, Molina JA, Hernánz A, Fernández-Vivancos E, de Bustos F, Barcenilla B, Gómez-Escalonilla C, Zurdo M, Berbel A, Villanueva C.
Journal: Neurosci Lett. 1999 Aug 13;271(1):33-6.
PMID: 10471207
In this study, the researchers collected samples of cerebrospinal fluid from 24 individuals with Parkinson’s to compare with samples obtained from 40 matched controls. The mean cerebrospinal fluid levels of thiamine did not differ significantly from those of controls, but the investigators did see lower levels of free thiamine (not being untilised) in the Parkinson’s group. But the researchers noted that the thiamine levels observed in the study were not correlated with age, age at onset, duration of the disease, scores of the Unified Parkinson Disease Rating Scale (UPDRS), or the Hoehn and Yahr staging in the PD group.
So it doesn’t look like there is a strong association between low thiamine levels and PD.
There was however a paper published a couple of year ago that explored intake of vitamin B before onset of Parkinson’s:
 Title: Low plasma thiamine and phosphate in male patients with Parkinson’s disease is associated with mild cognitive impairment.
Title: Low plasma thiamine and phosphate in male patients with Parkinson’s disease is associated with mild cognitive impairment.
Authors: Håglin L, Domellöf M, Bäckman L, Forsgren L.
Journal: Clin Nutr ESPEN. 2020 Jun;37:93-99.
PMID: 32359763
This was a case controlled study from a research group in Umeå (Sweden). A case–control study is a type of observational study in which two existing groups differing in outcome are identified and compared. After analysing 75 individuals with PD and 24 control individuals, they reported that higher nutrition scores and higher thiamine levels in the blood at baseline decreased the risk of male participants to have a mild cognitive impairment (but curiously this effect was not observed in female participants). It was a small study, but perhaps it points towards the need to good nutrition and a balanced diet. The authors concluded that their results “indicate that nutritional factors may influence cognitive function in males in the early phase of PD“.
Does this mean that vitamin B1 isn’t involved with Parkinson’s?
No, it simply means that levels of thiamine appear to be relatively normal in individuals with Parkinson’s (on average! There may be individual differences) and that increasing levels (in males) might help reduce the risk of mild cognitive impairment.
What about motor impairment? Is there any evidence suggesting vitamin B1 can help with movement?
As we discussed above, vitamin B1 is involved in a wide range of important biochemical processes that are critical for normal cellular function. These include the release of dopamine in the brain.

Dopamine being released by one cell and binding to another. Source: Truelibido
Researchers have reported that delivery of TTP (the active factor of thiamine) to the brains of rodents resulted in increased levels of dopamine being released (Click here to read more about this).
It has to be said that there is a lack of research exploring thiamine/vitamin B1 in the context of Parkinson’s. In fact, if you go to the biomedical search engine Pubmed and conduct a search for the keywords “Parkinson’s” and “Thiamine”, you will only find 51 responses (at the date of this post being published), and many of them are not specifically focused on PD.
Have there been any clinical studies of thiamine in Parkinson’s?
Yes, and this is where we get back to Dr Costantini and colleagues.
As mentioned above, Dr Costantini and colleagues published the results of their first study in 2013:
 Title: High-dose thiamine as initial treatment for Parkinson’s disease.
Title: High-dose thiamine as initial treatment for Parkinson’s disease.
Authors: Costantini A, Pala MI, Compagnoni L, Colangeli M.
Journal: BMJ Case Rep. 2013 Aug 28;2013:bcr2013009289.
PMID: 23986125 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers recruited three individuals with newly diagnosed Parkinson’s (they were not on any anti-Parkinson’s treatments). They firstly checked their blood levels of thiamine and found that they were within the normal healthy range. Next they performed the Unified Parkinson’s Disease Rating Scale (UPDRS) to gain a baseline measure of the level of Parkinson’s in each of the participants, and then they started a regime of high dose thiamine (100 mg parenterally twice a week).
After 15 days (and four treatments), they conducted another assessment and found remarkable responses from the three participants, including a 31.3 to 77.3% improvement in the motor portion of the (UPDRS).
What did they suggest could be the cause of this change?
The researchers proposed that “the motor and non-motor symptoms of PD could derive from a chronic thiamine deficiency” in specific regions of the brain. And by increasing in thiamine levels in these regions of the brain (via high dose treatment) may help to improve the motor performance. This is an intriguing idea, but the blood thiamine levels were normal and the investigators provided no evidence to support this speculation (the levels of thiamine in the brain/cerebrospinal fluid were not examined).
To be fair this was just a small pilot study, so it is difficult to take too much away from it, but the results encouraged the investigators to dig deeper with a second much larger open label study which was published in 2015:
 Title: Long-Term Treatment with High-Dose Thiamine in Parkinson Disease: An Open-Label Pilot Study.
Title: Long-Term Treatment with High-Dose Thiamine in Parkinson Disease: An Open-Label Pilot Study.
Authors: Costantini A, Pala MI, Grossi E, Mondonico S, Cardelli LE, Jenner C, Proietti S, Colangeli M, Fancellu R.
Journal: J Altern Complement Med. 2015 Dec;21(12):740-7.
PMID: 26505466
In this study, Dr Costantini and colleagues recruited 50 individuals with PD. There were 33 men and 17 women, with an average age of 70 years and an average disease duration of 7 years. Again, all the participants were assessed at baseline with the UPDRS and assessments of fatigue, and then given a treatment regime of 100 mg of thiamine (administered intramuscularly twice a week). This treatment was given without any change to the participants personal therapy (for example, L-dopa or dopamine agonists). All the patients were re-evaluated after 1 month and then every 3 months after that.
The researchers found that high dose thiamine treatment resulted in significant improvement of both motor and non-motor symptoms in the participants. The average UPDRS scores (parts I-IV) improved from 38 to 18 (a high score indicates worsening severity) within 3 months. And the investigators indicated that “The clinical improvement was stable over time in all the patients“.
When the motor score of the UPDRS (part III) was analysed, the researchers found an improvement from 22 to 10 (again, a decrease suggests improvement). And this was a much longer study with the follow-up duration ranging from 95 to 831 days (the average was 291 days). The researchers concluded their study by stating that “Thiamine could have both restorative and neuroprotective action in Parkinson’s”.
And Dr Costantini and his team did not stop there – they published a third study in 2016:
 Title: An open-label pilot study with high-dose thiamine in Parkinson’s disease.
Title: An open-label pilot study with high-dose thiamine in Parkinson’s disease.
Authors: Costantini A, Fancellu R.
Journal: Neural Regen Res. 2016 Mar;11(3):406-7.
PMID: 27127471 (This report is OPEN ACCESS if you would like to read it)
This is a briefer report that outlines the analysis of a further 10 individuals with Parkinson’s being treated with high dose thiamine. The results are very similar to the previous two studies.
|
# # RECAP #2: Researchers have found no deficiency in vitamin B1 in people with Parkinson’s. Open label studies exploring high dose thiamine in individuals with PD have reported significant improvements in both motor and non-motor symptoms. Whether these effects are disease modifying still needs to be tested in a blinded, randomised, placebo controlled trial. # # |
The results sound really interesting! Should I try high dose thiamine?
Again (and I hate to berate the message), all of this clinical research has been open label. We really need to see a randomised, placebo-controlled, double-blind study before we jump to conclusions.
It still looks interesting though, right?
A reader of this website contacted me some time ago and pointed out something curious about vitamin B1/thiamine.
They had been interested in the high dose thiamine approach for their Parkinson’s and decided to do some homework on it. And what they found was that thiamine (and its derivatives) cannot cross the blood-brain barrier by simple diffusion (the blood-brain barrier being a membrane that surrounds and protects the brain).
What does that mean? Simple diffusion?
Well, some molecules can just pass through membranes and barriers without issue. But thiamine needs to be manually transported into the brain.
Transportation of thiamine from the blood to the brain is mediated by two transporters (thiamine transporters-1 and -2). This makes the process of getting thiamine into the brain rather slow. And raising levels of thiamine in the blood does not lead to an increase in thiamine transportation across the blood-brain barrier or to a corresponding increase in brain levels.
The reader also pointed towards pilot clinical studies of high-dose thiamine in Alzheimer’s.
The first trial of high dose thiamine (3 grams per day) in Alzheimer’s was a 12-month, double-blind, parallel-group study, which reported “No significant differences were found between the placebo and thiamine groups at any point during the study” (Click here to read more about this).
Subsequent studies were also not supportive.
But then the reader found something else: Benfotiamine
What is Benfotiamine?
Benfotiamine is a lipid-soluble synthetic precursor of thiamine, but crucially: it has better bioavailability – meaning that it is absorbed into the body better than thiamine.
What does lipid-soluble mean?
It refers to the ability of an agent to dissolve in fats, oils, and lipids. More importantly, it means that unlike thiamine (which is not lipid-soluble), benfotiamine has less issues crossing the blood-brain-barrier than thiamine.
Benfotiamine is better at accessing the brain (Click here to read more about this).
And once it gets in the brain, benfotiamine is converted into thiamine.
So the reader was wondering if benfotiamine might be a better approach than thiamine.
Interesting. Has any preclinical research been done on benfotiamine?
Not in Parkinson’s models (please correct me if I am wrong here), but beneficial properties of benfotiamine have been demonstrated in models of Alzheimer’s. For example:
 Title: Benfotiamine treatment activates the Nrf2/ARE pathway and is neuroprotective in a transgenic mouse model of tauopathy.
Title: Benfotiamine treatment activates the Nrf2/ARE pathway and is neuroprotective in a transgenic mouse model of tauopathy.
Authors: Tapias V, Jainuddin S, Ahuja M, Stack C, Elipenahli C, Vignisse J, Gerges M, Starkova N, Xu H, Starkov AA, Bettendorff L, Hushpulian DM, Smirnova NA, Gazaryan IG, Kaidery NA, Wakade S, Calingasan NY, Thomas B, Gibson GE, Dumont M, Beal MF.
Journal: Hum Mol Genet. 2018 Aug 15;27(16):2874-2892.
PMID: 29860433 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers tested benfotiamine treatment in an Alzheimer’s mouse model. These mice produce very high levels of the human TAU gene carrying the P301S genetic mutation. The investigators found that benfotiamine-treated P301S mice lived significantly longer than P301S mice fed with a control diet (An average of 390 vs 322 days, or a 21% increase in longevity).
 Source: PMC
Source: PMC
Benfotiamine treatment also reduce behavioral issues in these mice, and decreased neurodegeneration. It also reduced advanced glycation end (AGE) products (Click here to read a previous SoPD post about AGE and RAGE inhibition).
The researchers also found that benfotiamine treatment reduced inflammation and oxidative stress, via activation of the NRF2 pathway (Click here to read a previous SoPD post on the NRF2 pathway).
Other independent research groups have reported similar results with benfotiamine (for example, click here and here to read more about this).
And recently researchers published the results of a clinical trial evaluating benfotiamine in individuals with Alzheimer’s:
 Title: Benfotiamine and Cognitive Decline in Alzheimer’s Disease: Results of a Randomized Placebo-Controlled Phase IIa Clinical Trial.
Title: Benfotiamine and Cognitive Decline in Alzheimer’s Disease: Results of a Randomized Placebo-Controlled Phase IIa Clinical Trial.
Authors: Gibson GE, Luchsinger JA, Cirio R, Chen H, Franchino-Elder J, Hirsch JA, Bettendorff L, Chen Z, Flowers SA, Gerber LM, Grandville T, Schupf N, Xu H, Stern Y, Habeck C, Jordan B, Fonzetti P.
Journal: J Alzheimers Dis. 2020;78(3):989-1010.
PMID: 33074237 (This report is OPEN ACCESS if you would like to read it)
In this study, the investigators recruited 70 people with mild cognitive impairment or mild dementia due to Alzheimer’s, and they randomly assigned them to daily treatment with benfotiamine (N=34) or placebo (N=36) for 12 months. The treatment involved one 300 mg capsule of benfotiamine in the morning and another one in the evening everyday.
One year of oral benfotiamine treatment was found to be safe and well tolerated.
More importantly, the progression in cognitive issues was 43% slower in the benfotiamine group than in the placebo group (as measured by the Alzheimer’s Disease Assessment Scale–Cognitive Subscale – ADAS-Cog). This result suggested that there was less cognitive decline in the benfotiamine-treated group. And this effect was also seen in the clinical dementia rating (CDR) score which found that the benfotiamine-treated group was 77% better off compared to the placebo group (curiously, this effect was stronger in the APOE ε4 non-carriers – click here to read a previous SoPD post about APOE).
And remember that this study was randomized, placebo-controlled, double-blinded trial of benfotiamine. This was not open label. If high-dose thiamine is a treatment for Parkinson’s in the future, this is the type of study we need to see. It could actually be interesting to see thiamine compared with benfotiamine in such a study.
The researchers who conducted the benfotiamine in Alzheimer’s study are now planning a larger trial of benfotiamine in Alzheimer’s to see if they can replicate and extend on the results over a longer period of time.
And a group of scientists in China recently published safety and tolerability data for benfotiamine in healthy volunteers, providing a better characterisation of the agent (Click here to read more about this).
So what does it all mean?
As I suggested at the top, I have been reluctant to write this post because there are some vested interests involved with thiamine. I have been contacted folks who have told me that high-dose thiamine has really helped them. But I have equally been asked by a lot of folks to write a post on the topic.
I think the take home message from the SoPD point of view is that there simply isn’t enough research on thiamine (high-dose or otherwise) in the context of Parkinson’s to make any kind of statement. I have tried to be fair in this post, but most of the preclinical work was conducted last century. And while Dr Costantini and his colleagues have provided stimulating pilot data, more carefully controlled studies are required. The gold standard is a randomised, double-blind, placebo-controlled clinical trial, and that is what is missing from this story.
And until that is conducted, we here at the SoPD will politely defer from making any judgements or statements on thiamine.
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
EDITOR’S NOTE: The information provided by the SoPD website is for information and educational purposes only. Under no circumstances should it ever be considered medical or actionable advice. It is provided by research scientists, not medical practitioners. Any actions taken – based on what has been read on the website – are the sole responsibility of the reader. Any actions being contemplated by readers should firstly be discussed with a qualified healthcare professional who is aware of your medical history. While some of the information discussed in this post may cause concern, please speak with your medical physician before attempting any change in an existing treatment regime.
The banner for today’s post was sourced from Wikipedia

.png){kind=link}
Hey Simon.
Randall from Toronto here.
Still taking the Subtilis. Bactillus for cognate issues w PD. Anecdotally I think it’s helping me (doing better on Jeopardy than ever before…lol-perhaps we can make that part of the cognitive testing in PD..the Jeopardy Threshold ..lol. Met w a person we have in common few months ago…Brian Stecher…Nothing but praise for u. I told him how much enjoy your analysis. I always know real intelligence by the way a person can take difficult nuanced issues and boil them down to their basic elements and communicate them simply so that even I and the common person….can understand the concept. So based on your analysis above I’m not gonna try the thiamine but the benfotiamine. Any studies on dosage? Thanks so much once again for your reviews which are a pleasure to read. Randall Rothbart
LikeLike
Hi Randall,
Thanks for your message and kind words. In terms of trying benfotiamine, PLEASE consult with your neurologist/clinician before proceeding. There may be something in your medical history that may complicate things. The Chinese safety, tolerability and pharmacokinetics study mentioned in the post used high doses, but for only a short period of time. The Phase IIa Alzheimer’s study used 300mg twice per day. You may want to contact the researchers who conducted that study and ask them about dose. But as I said, please do this only after consulting with your physician.
Kind regards,
Simon
LikeLike
Hi Simon,
I have PD and no experience with vitamin B1 supplements. It seems that the finding “that thiamine (and its derivatives) cannot cross the blood-brain barrier by simple diffusion” is a strong argument against the efficacy of vitamin B1 in PD. However, I assume that this finding was made in experiments with healthy brain tissue samples. This could make a difference because if I am not mistaken I have also read that the blood-brain barrier is often somewhat disrupted and more permeable in people with PD than in people without PD. If this increased permeability also applies to thiamine, this could mean that in some PD patients who consume large amounts of thiamine, at least a small amount of it could get into the brain through those leaks without using any transporter. Or is this idea too naive?
zz
LikeLike
Hi zz,
Thanks for the interesting comment. It is not naive, but I think we sometimes get the wrong idea when people say that the BBB can become more permeable under certain conditions. It is still mostly in tact and leaky spots get patched up rather dynamically. It is not a static thing is my point, I guess. Rather than using the word permeable, we should probably say weaker. But the BBB still does a remarkable job of keeping things out. Yes, perhaps some thiamine may be getting through a weaker BBB, but it really needs to be investigated. When the next clinical study of thiamine is conducted in PD, it would be interesting to assess how much is accessing the brain (with CSF measures or some kind of tracer). That is the only real way to test this.
Thanks again for the great question!
Kind regards,
Simon
LikeLike
Sorry– one thing forgot to tell you.
Love the title to the paper.
Be one
B1
Very clever
Randall Rothbart
LikeLike
Ben,
I found this an interesting read and wondered if you might find it helpful. They mention fatigue and IBS among other things. I already take a low dose vit B supplement but might try a higher dose.
Ma ________________________________
LikeLike
Hi Jellywoman,
Glad you liked the post.
Kind regards,
Simon
LikeLike
Interestingly B1 helps carbohydrate metabolism. Ketones also beneficial to pd brain. Then there’s the promise of GLP agonists. Common thread?
LikeLike
It would be great to hear back more from the guy who suggested that Benfotiamine might be a better alternative to Thiamine because of being more able to cross the blood-brain barrier … did he actually try using Benfotiamine and what outcomes he did get from it.
LikeLike
Hi Andrew,
Thanks for your comment. The reader contacted me regarding this a couple of years ago, and I haven’t heard from them for a while. At the time, they said that they wanted to remain anonymous. I am not sure if they tested benfo. but yes, it would be interesting to learn more if they did. I will have a search for them and see if they have anything to share.
Kind regards,
Simon
LikeLike
Click to access AJBSR.MS.ID.000621.pdf
LikeLike
Hi Simon,
According to this publication of the Laboratory of Neurophysiology, GIGA-Neurosciences University of Liègi it would seem that benfothiamine is water soluble form.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8196556/#__ffn_sectitle
LikeLike
Thank you for another interesting post. I do, however, think that the statistical treatment of the B1 case is firmer than you suggest. This follows if you take into account the conquences of not making a decision. Furthermore, the placebo effect is real.
I am reminded of this story, possibly apocryphal, from the early days of Himalayan mountaineering. A climber has reached the summit too late in the day to make a descent. He realizes that if he is benighted at this altitude he is almost certain to freeze to death. He can see an icy slope going in the right direction. But, he can only see the top of the slope, lower down there may be be rocks. Should he jump?
LikeLike
Hello Simon,
I was diagnosed with PD (Parkinsonism) in 2018. I prefer a natural approach when it comes to healing however its not available with PD in the U.S.. so i took the prescribed C/L. Until i found mucuna. Recently i had a scare where nothing seemed to help and i was battling constipation. I read an article on B1 TTFD and an article on Berberine. I started taking berberine and 10mg of B1 TTFD. Im regular again and the mucuna seem to be helping. I consult my neurologist and provide a list of the supplements i take. But it’s not familiar so i dont think it matters. It is really a sad situation. Very informative article for those of us who take our health into our own hands Thank You
BK
LikeLike
Thank you so much for taking the time to write this article about B1. I appreciate your even handed analysis.
I am a high school biology teacher, and I teach about the need for randomized controlled trials in medicine and about the placebo effect. I appreciate that randomized controlled trials are the gold standard in medicine, for good reason.
My follow up question is this: If people are getting significantly better and staying better for years, who cares if it the mechanism is “merely” a placebo effect? Maybe someone would argue that an effect which is merely a placebo would wane over time… is this the issue? If so, it should be fairly easy to follow up with the original patients and see if their condition remains improved now years later.
My second follow up question is why are the powers that be sufficiently un-impressed with Dr. Constantini’s data that no one is willing to fund a randomized controlled trial. I found the videos of his patients to be quite compelling. Assuming that these videos have not been cherry picked or faked or manipulated in some way, thiamine/benfotiamine seems like a great lead that deserves a randomized controlled study.
LikeLike
Hi Jessie
Just come across this article and the responses. I totally agree with you and can answer your question- money! Pharmaceutical companies will not make any money out of Vitamin B1 trials. What is not made clear to the patients being prescribed these drugs is that 1) not everyone will benefit 2) number needed to treat. NICE guidelines are dictated by clinical trials from pharmaceutical companies who will only under take those trials if money WILL be made. There is no incentive for them to find a cure due to loss of income. you may be interested in this https://www.facebook.com/groups/512119977204633
LikeLike