
|
# # # # I was reluctant to write this post given the media storm that tainted this drug during the early days of the COVID pandemic, but the science here is intriguing. Recently, researchers conducted a nationwide case-controlled study of 22,189 Finnish people diagnosed with Parkinson’s between 1996 to 2015. When they analysed their large dataset, they found an association between hydroxychloroquine and a lower risk of developing Parkinson’s. In today’s post, we will review this new research and discuss what could explain this curious finding. # # # # |
 Dr Didier Raoult. Source: Letelegramme
Dr Didier Raoult. Source: Letelegramme
On March 16, 2020, a video discussing a small study investigating the use of a drug called hydroxychloroquine in patients with SARS-CoV-2 was posted on YouTube (and a few days later a report on the study was made available).
It was an open-label, non-randomized study involving just 36 hospitalized patients with documented SARS-CoV-2 infections. It was a methodologically flawed study and making the results public without any kind of peer-review step was unethical, but this did not stop these results causing a media storm. And news of a potential first weapon in the fight against the new viral pandemic quickly spread, causing shortages in supplies of the drug for individuals with inflammatory conditions who actually needed it.
Eventually, a number of much larger and better designed clinical trials demonstrated that the drug did not represent a sensible treatment against COVID (Click here to read more about this).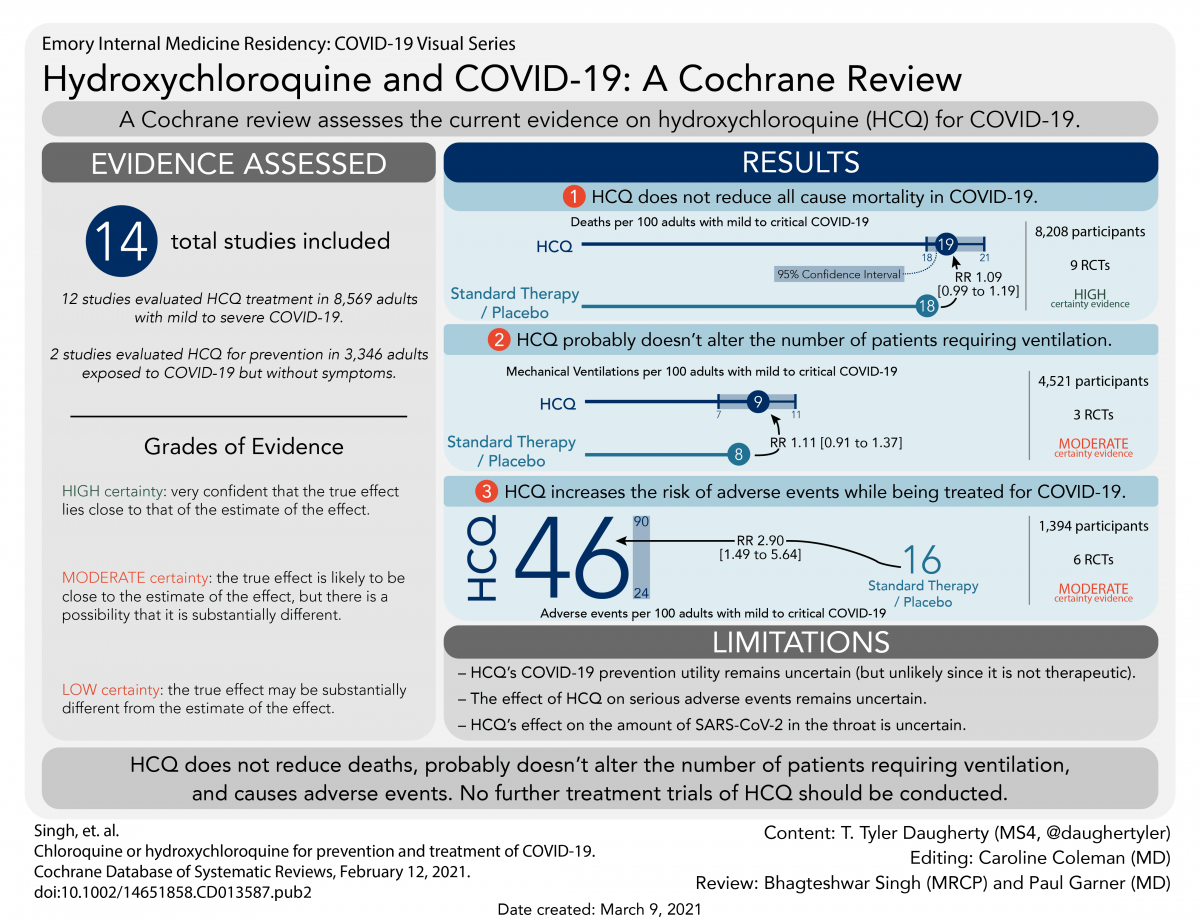
But sadly, a previously very useful treatment became somewhat tainted. And it has since been the subject of many jokes, cartoons and memes:
 Source: TheWeek
Source: TheWeek
Despite its 15 minutes of ignominy though, hydroxychloroquine is still a very useful drug and it may still hold one or two surprises.
Great. But what does this have to do with Parkinson’s?
Well, one of those surprises could relate to Parkinson’s. Very recently, this research report was published:
 Title: Disease-Modifying Antirheumatic Drugs and Risk of Parkinson Disease: Nested Case-Control Study of People With Rheumatoid Arthritis.
Title: Disease-Modifying Antirheumatic Drugs and Risk of Parkinson Disease: Nested Case-Control Study of People With Rheumatoid Arthritis.
Authors: Paakinaho A, Koponen M, Tiihonen M, Kauppi M, Hartikainen S, Tolppanen AM.
Journal: Neurology. 2022 Mar 22;98(12):e1273-e1281.
PMID: 35064025 (This report is OPEN ACCESS if you would like to read it)
In this study, some researchers in Finland conducted a nationwide case-controlled study.
What does ‘case-controlled’ mean?
Case-controlled studies are retrospective. They involve two clearly defined groups: one with the outcome/condition and one without the outcome/condition. They then look back into the (medical) past to assess whether there is a statistically significant difference in the rates of an event occurring between the groups. Case-controlled studies should involve two groups that are identical EXCEPT for their outcome.
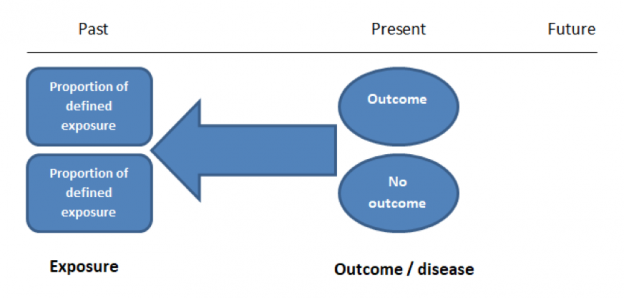 Case controlled study. Source: Students4bestevidence
Case controlled study. Source: Students4bestevidence
This is different to a ‘cohort study’ which can be retrospective or prospective, but usually involves following a large group of individuals and comparing outcomes based on exposures (think of the Honulu Heart study – Click here to read more about that). A cohort study should include two groups that are identical EXCEPT for their exposure status.

A cohort study. Source: Students4bestevidence
Importantly, case-controlled studies are better for very rare events, such as determining whether a condition like diabetes increases the risk of developing Parkinson’s (Click here to read a previous SoPD post on that topic).
So in this new study, the Finnish researchers took the medical data that has been collected in the Finnish Parkinson’s Disease (FINPARK) cohort, which includes 22,189 Finnish people who were diagnosed with Parkinson’s between 1996 to 2015.
From this dataset, they pulled out all of the cases of Parkinson’s that included a diagnosis of rheumatoid arthritis more than 3 years before the onset of PD.
This gave them a small dataset of 315 cases.
More than 60% of the cases in this smaller dataset were female, and the median duration of their rheumatoid arthritis was approximately 12.6 years.
The researchers then matched each of these cases with up to 7 control cases of people with rheumatoid arthritis. They were matched by age, sex, duration of rheumatoid arthritis, and region. This second set of cases (totaling 1,571 cases) were used for the comparison.
What were they comparing?
The researchers wanted to see if there were any rheumatoid arthritis medications that may reduce the risk of developing Parkinson’s.

Inflammation is believed to be a key player in the development of Parkinson’s, and identifying anti-inflammatory drugs that are associated with reduced risk of PD might provide us with novel insights into the biology underlying the condition.
Got it. So what did they find?
They found that of all the rheumatoid arthritis medications (referred to as ‘disease-modifying anti-rheumatic drugs’ or DMARDs) used, only chloroquine/hydroxychloroquine was associated with a potentially decreased risk of developing Parkinson’s. The adjusted odds ratio for this association was 0.74 (95% CI 0.56–0.97).
What is an odds ratio?
An odds ratios (which are measures of association, rather than risk or causation) of 1.0 indicates that the odds of a situation are the same between group. An odds ratio of 0.74 means that chloroquine/hydroxychloroquine was associated with a ~25% reduced risk of Parkinson’s.
Ok. So what exactly is hydroxychloroquine?
Hydroxychloroquine is a synthetic anti-malarial drug, although the parasite has become largely resistant to it. It is also used for the treatment of inflammatory conditions including rheumatoid arthritis, lupus, Sjögren’s syndrome, and dermatomyositis.
 Hydroxychloroquine. Source: Cidrap
Hydroxychloroquine. Source: Cidrap
The backstory of the drug is really interesting: Bark extracts from the Peruvian Cinchona tree have long been used to treat malaria, and it was introduced to Spain when Jesuit missionaries began returning from the New World.
 Bark from the Cinchona tree. Source: Phys
Bark from the Cinchona tree. Source: Phys
Quinine – the anti-malarial component in these bark extracts – was first isolated in 1820, and the history of this agent is truly fascinating. From saving Popes to becoming a key factor in the direction of World War II, quinine has quietly been playing an important role in many historical events (Click here to read more about this).
At the end of World War I, the German government sought to identify alternatives to quinine as an anti-malarial treatment. It was becoming less effective as the malaria parasite was gradually developing resistance to it, and high doses of the drug could result in death or permanent visual loss. The search for an alternative led to a synthetic analogue called chloroquine, which was discovered in 1934, by researchers at Bayer laboratories. Efforts to achieve superior pharmacological properties then resulted in the development of hydroxychloroquine.
Hydroxychloroquine was first approved for medical use in the United States way back in 1955, so we have a long history of clinical use. And in 2019 (the year before it became a household name in the COVID pandemic) more than 5 million prescriptions were written for it (Source).
|
# RECAP #1: Researchers in Finland conducted a large medical database comparison study to identify agents used in the treatment of rheumatoid arthritis that might reduce the risk of developing Parkinson’s. Their results indicate that only chloroquine/hydroxychloroquine was associated with a reduced risk of PD. # |
Is this the first time this association has been reported?
No.
The association between chloroquine/hydroxychloroquine and a lower risk of Parkinson’s has been previously reported in a case-control study.
This is that report:

Title: Immunosuppressants and risk of Parkinson disease
Authors: Racette BA, Gross A, Vouri SM, Camacho‐Soto A, Willis AW, Nielsen SS
Journal: Annals of Clinical and Translational Neurology, 2018 May 31;5(7):870-875.
PMID: 30009205 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers analysed the collected prescription data from the database of United States Medicare beneficiaries age 60–90 in 2009. They were looking for any immunosuppression medication and comparing their use with the incidence of Parkinson’s within the analysed group. And to make the data more interesting and informative, the investigators broke the immunosuppressant medications down into six categories, which were:
- Calcineurin inhibitors (cyclosporine, tacrolimus)
- Inosine monophosphate dehydrogenase (IMDH) inhibitors (azathioprine, leflunomide, mycophenolate)
- Dihydrofolate reductase inhibitors (methotrexate)
- Biologics (abatacept, adalimumab, anakinra, certolizumab, etanercept)
- Corticosteroids (prednisone, prednisolone, methylprednisolone, dexamethasone, cortisone, hydrocortisone)
- Miscellaneous (hydroxychloroquine, sulfasalazine, mesalamine, interferon beta‐1a, thalidomide, lenalidomide, glatiramer acetate, flingolimod, and dimethyl fumarate).
Of these groups, two were significantly associated with a lower risk of PD:
- Corticosteroids (Relative risk = 0.80; 95% Confidence Interval 0.77–0.83)
- IMDH inhibitors (Relative risk = 0.64; 95% Confidence Interval 0.51–0.79)
This suggests that people who had been prescribed IMDH inhibitors had 1/3 less incidence of Parkinson’s. On the SoPD, we have previously discussed Parkinson’s research on azathioprine and dexamethasone (Click here to read a SoPD post about that).
But, if you dig deep into the presented data of this 2018 report, you will find “a protective association for hydroxychloroquine when any exposure before PD diagnosis was considered (relative risk 0.77, 95% CI 0.65–0.90) and a weaker association when exposure occurring at least 1 year before the outcome was investigated (relative risk 0.83, 95% CI 0.68–1.00)” (quote from Source).
So how is hydroxychloroquine reducing the risk of Parkinson’s?
So this is where this curious association gets a bit confusing.
You see, chloroquine and hydroxychloroquine are both recognised for their ability to inhibit autophagy.
What is autophagy?
Autophagy (from the Ancient Greek αὐτόφαγος autóphagos, meaning “self-devouring”) is an absolutely essential function in a cell. Without autophagy, old proteins would pile up, making the cell sick and eventually causing it to die. Through the process of autophagy, the cell can break down the old protein, clearing the way for fresh new proteins to do their job.

The process of autophagy. Source: Wormbook
Waste material inside a cell is collected up in membranes that form sacs (called vesicles), ultimately forming what becomes an autophagosome. These large bags of waste then bind to other sacks (called lysosomes) which contain enzymes that will breakdown and degrade the waste material – the same way enzymes in your washing powder break down muck on your dirty clothes. The degraded waste material can then be recycled or disposed of by spitting it out of the cell.
Now, chloroquine and hydroxychloroquine block the binding of autophagosomes to lysosomes (by altering the acidic environment inside the lysosomes):
 Source: EMBO
Source: EMBO
This results in the accumulation of a large amounts of degraded proteins inside of cells, which can lead to stress on the cell and cell death (Click here to read more about this).
This is one of the mechanisms by which hydroxychloroquine works against malaria: The drug accumulates in the lysosomes of the malaria parasite, raising the acidity and interfering with the parasite’s ability to grow and replicate.
Now, long-time readers of the SoPD blog will be aware that lysosomal disfunction is widely considered a key player in the pathogenesis of Parkinson’s. Many of the genetic risk factors associated with PD are related to lysosomal function (Click here to read a previous SoPD post on this topic). That is to say, it is widely believed that disrupted lysosomal function is believed to make people vulnerable to developing Parkinson’s.
So the key question here is: how does a drug that knowingly inhibits lysosomal function, reduce the risk of developing Parkinson’s?!?!? Shouldn’t it be increasing the risk of Parkinson’s???
And it is a good question.
But hydroxychloroquine is a drug that has multiple mechanisms of action, and these could help explain the association.
For example, you will remember that in addition to treating malaria, hydroxychloroquine is also used in the treatment of rheumatoid arthritis, lupus, and other inflammatory conditions.
Ok, so how does hydroxychloroquine influence inflammatory conditions?
In addition to disrupting lysosomal function, chloroquine and hydroxychloroquine both inhibit Toll-like receptors.
Que?!?
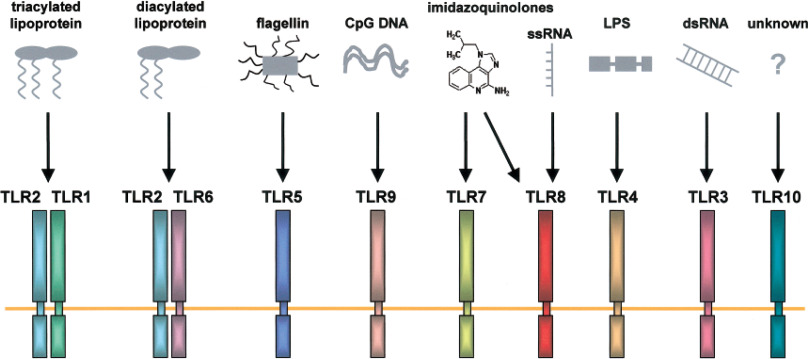
Toll-like receptors (or TLRs) are an important family of receptors that represent on of the first lines of defense against various invading microbes. They sit on the outer surface of cells, waiting to be triggered by different types of pathogens (disease causing organisms):
 Source: Sciencedirect
Source: Sciencedirect
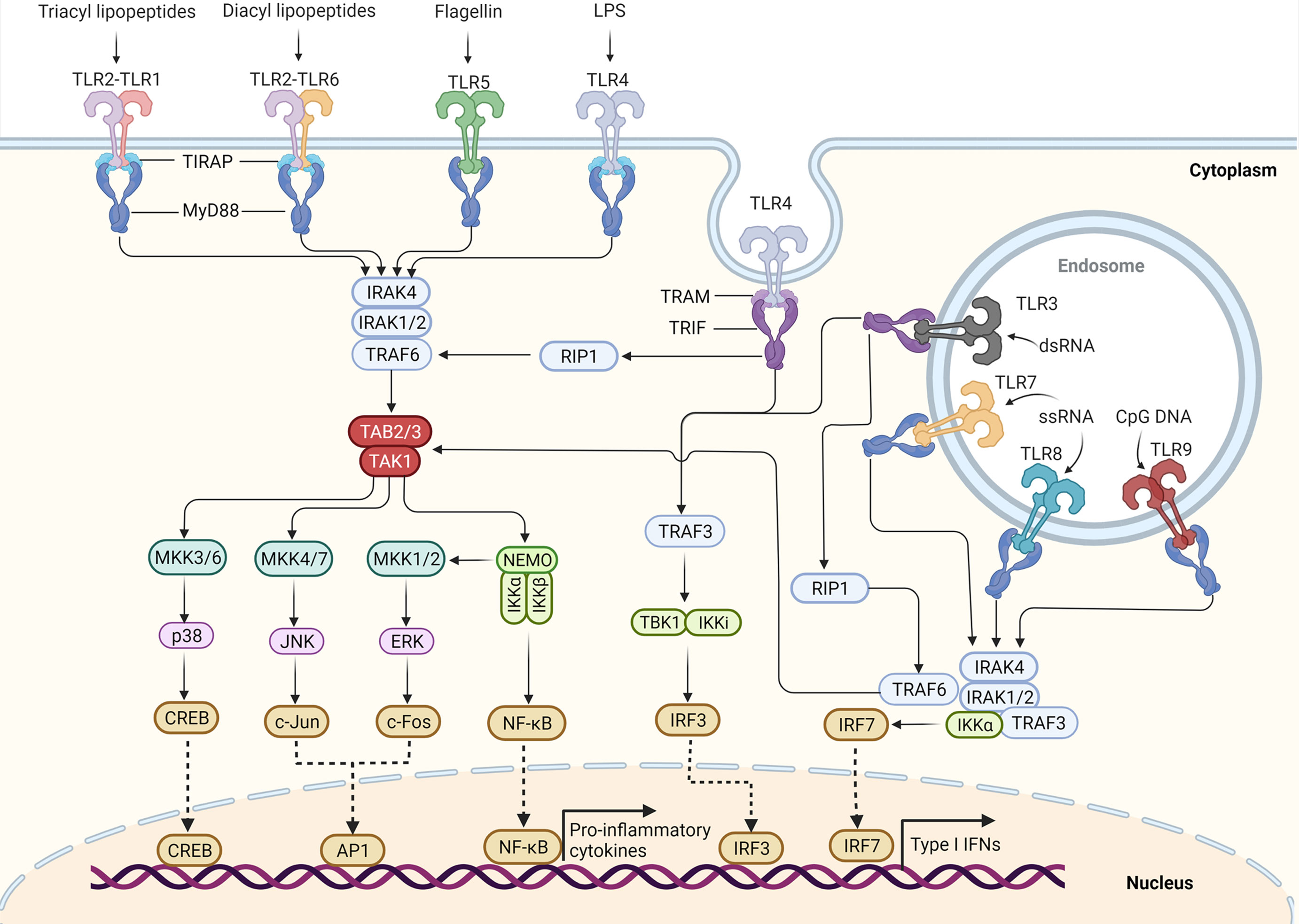
Once one of these receptors are activated, it unleashes a cascade of signalling pathways inside of the cell that all leads to the activation of pro-inflammatory genes (such as NFκB), and this leads to the release of inflammatory cytokines (tiny messenger proteins):
 Source: Frontiers
Source: Frontiers
Both chloroquine and hydroxychloroquine have been shown to inhibit of TLR3, TLR7 and TLR9 and this results in a reduction in these inflammatory cytokines from being released. And this process is particularly apparent on cells in the peripheral immune system (such as macrophages and dendritic cells, as well as B and T cells):
 Source: EMBO
Source: EMBO
This is why hydroxychloroquine is used in the treatment of inflammatory conditions, like Lupus and rheumatoid arthritis.
And this could help explain how this drug is reducing the risk of Parkinson’s – by dampening down the immune system (Click here for a good review on the research exploring the mechanisms of action for hydroxychloroquine).
|
# # RECAP #2: Hydroxychloroquine is a drug with several functions, including disruption of the lysosomal/waste disposal system. But its ability to reduce inflammation may explain why how it could be reducing the risk of developing Parkinson’s. # # |
So should I speak with my doctor about taking hydroxychloroquine?
No.
Hydroxychloroquine has never been clinically tested for any disease modifying potential in people with Parkinson’s, and while the data above is interesting, there is conflicting results which raise all sorts of questions.
What kind of conflicting results?
In 2019, a report exploring the risk of Parkinson’s in another inflammatory condition (Sjögren syndrome) found an increased risk of Parkinson’s in people treated with hydroxychloroquine:
 Title: Risk of Parkinson disease in Sjögren syndrome administered ineffective immunosuppressant therapies: A nationwide population-based study.
Title: Risk of Parkinson disease in Sjögren syndrome administered ineffective immunosuppressant therapies: A nationwide population-based study.
Authors: Ju UH, Liu FC, Lin CS, Huang WY, Lin TY, Shen CH, Chou YC, Lin CL, Lin KT, Kao CH, Chen CH, Yang TY.
Journal: Medicine (Baltimore). 2019 Apr;98(14):e14984.
PMID: 30946325 (This report is OPEN ACCESS if you would like to read it)
Sjögren’s (pronounced show-grins) syndrome is a systemic autoimmune condition in which the body’s immune system attacks the glands that secrete fluids, like tears and spit (saliva). As a result, the primary symptoms are dry eyes and a dry mouth.
In this study, the researchers used medical data from 12,640 patients with Sjögren’s collected from Taiwan’s National Health Insurance Research Database from 2000 to 2010. They compared this dataset with data from a control group of 50,560 people without Sjögren’s.
The investigators reported an increased incidence of Parkinson’s in the patients with Sjögren’s (compared to the control group). Curiously, the data indicated that the risk of Parkinson’s was higher in individuals with Sjögren’s who did not have any comorbidities (additional medical conditions) than in those with comorbidities.
And when the researchers looked at any influence the medication (used to treat Sjögren’s) might have had, they found that individuals taking hydroxychloroquine had a higher incidence. That is to say, people with Sjögren’s taking hydroxychloroquine had a higher risk of developing Parkinson’s.
In addition, those people with Sjögren’s taking non-hydroxychloroquine immunosuppressants had a reduced incidence of Parkinson’s.
This result suggests that the situation with hydroxychloroquine is not as clear as one might hope and further research is required before we can determine if this agent could have disease modifying potential (post-diagnosis) in Parkinson’s.
So what does it all mean?
There are some drugs that develop a bad reputation and struggle to shrug off the stigma associated with that reputation even when new research indicates some beneficial new property. An example of this is thalidomide of course, which had devastating consequences when it was initially used for morning sickness, but it has subsequently had a second life as an anti-cancer therapy and leprosy (Click here to read more about this).
While we are not advocating for hydroxychloroquine here at the SoPD, we do believe that there is something interesting to explore here in the context of Parkinson’s. Perhaps in the form of some preclinical studies utilising human cells and exploring the molecular biology associated with hydroxychloroquine (and non-hydroxychloroquine immunosuppressant) treatment. These investigations could explore and compare PD with a range of inflammatory conditions (such as Sjögren’s or rheumatoid arthritis).
I guess all I am really saying is let’s not write hydroxychloroquine off as some kind of joke, but rather do some careful analysis to see if/how it might be useful for Parkinson’s.
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
EDITOR’S NOTE: The information provided by the SoPD website is for information and educational purposes only. Under no circumstances should it ever be considered medical or actionable advice. It is provided by research scientists, not medical practitioners. Any actions taken – based on what has been read on the website – are the sole responsibility of the reader. Any actions being contemplated by readers should firstly be discussed with a qualified healthcare professional who is aware of your medical history. While some of the information discussed in this post may cause concern, please speak with your medical physician before attempting any change in an existing treatment regime.
The banner for today’s post was sourced from USAToday

Great info! It would also be worth investigating the potential for hydroxychloroquine to increase NURR1 levels.
LikeLike
I think you are correct to be very cautious when considering ‘association with…’ rather than ’caused by….). So much has changed with regard to using HCQ over the years. As a rheumatologist, I regularly prescribed it for SLE/RA/Sjogren’s with largely good effect. I think I got a ‘feel’ for who would do well or not. Inflammation itself is a broad range of reactions, so be cautious about making it sound like a ‘process’.
LikeLike
Dear Radoslav,
Thanks for your message. We wrote a post on VitB1 in April (https://scienceofparkinsons.com/2022/04/13/b1/). I hope this helps.
Kind regards,
Simon
LikeLike