
|
In today’s post we will review recent research regarding one particular family of bacteria, Helicobacter pylori, and what they might be doing in relations to Parkinson’s disease. |

Source: ScienceFriday
In his magnificent book, I contain multitudes, science writer/journalist Ed Yong writes that we – every single one of us – release approximately 37 million bacteria per hour. By talking, breathing, touching, or simply being present in the world, we are losing and also picking up the little passengers everywhere we go.
Reminds me of that Pascal Mercier book “Night Train to Lisbon” – We leave something of ourselves behind when we leave a place,… I’m not sure if this is what he was referring to though.
Yong also points out that: 80% of the bacteria on your right thumb are different to the bacteria on your left thumb.
It’s a fascinating book (and no, I am not receiving any royalties for saying that).

Microbes. Source: NYmag
We have discussed microbes several times on this blog, particularly in the context of the gut and its connection to Parkinson’s disease (Click here, here and here to read some of those posts). Today we are going to re-visit one particular type of microbe that we have also discussed in a previous post: Helicobacter pylori.

Helicobacter pylori. Source: Helico
Looks delightful. But what exactly is Helicobacter pylori?
Helicobacter pylori is a spiral shaped bacterium that lives in the stomach and duodenum (that is the section of intestine just below stomach). They are present in the gut of about 50% of us (more in the developing world, less in the western nations), but 85% of people will never display the symptoms of an infection.
The infection usually occurs in the first years of life and tends to persist indefinitely unless it is treated. Helicobacter pylori was initially found to cause gastritis and peptic ulcer, and has been associated with gastric cancer.

Source: Wikipedia
To avoid the acidic environment of the stomach, Helicobacter pylori will burrow into the mucus lining of the stomach, trying to reach the epithelial cells underneath, which is less acidic.
Mmmm, lovely. Are Helicobacter pylori associated with Parkinson’s disease?
There have been numerous studies that have assessed the Helicobacter pylori populations in the guts of people with Parkinson’s disease (for a good OPEN ACCESS review on this, please click here). The prevalence of Helicobacter pylori infections within the Parkinson’s disease community does appear to be quite high (see table below).
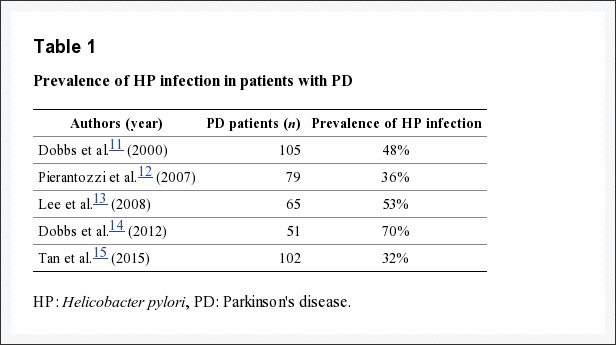
Source: NCBI
There has previously been little research indicating that Helicobacter pylori are directly involved with the development of Parkinson’s disease (Click here for one study suggesting a direct association), but there has been a lot of data indicating that they may be influencing the disease in other ways.
So what new research has been published about Parkinson’s disease and Helicobacter pylori?
Since we last discussed this topic (Click here for that post), three further research reports have been published:
Title: Association of Helicobacter pylori with Parkinson’s Disease
Authors: Mridula KR, Borgohain R, Chandrasekhar Reddy V, Bandaru VCh, Suryaprabha T
Journal: J Clin Neurol. 2017 Apr;13(2):181-186.
PMID: 28406585 (This article is OPEN ACCESS if you would like to read it)
In this study, researchers in India recruited 36 individuals with Parkinson’s disease and found a perfect split in the ratio of Helicobacter pylori infections – 18 of the participants were infected and 18 were not. The mean duration of the disease did not differ between the two groups (13.8 vs. 12.5 years, respectively), but interestingly the average daily dose of Levodopa was significantly higher among Helicobacter pylori infected group (824 mg in the infected group vs. 707 mg in the uninfected group).
The investigators next treated the infected group with Helicobacter pylori eradication drugs and at a 3-week follow-up, they found that the Helicobacter pylori eradication had caused a significant improvement the average Unified Parkinson’s Disease Rating Scale (UPDRS) scores. The researchers concluded that Helicobacter pylori infection was associated with a poor response to levodopa and increased medication usage. In addition, the eradication therapy had demonstrated better overall outcomes.
One caveat with this study (which the investigators admit to in their report) is that the study had an unblinded open-label design, meaning that they could not rule out a placebo effect. Obviously a follow up double blinded study is required, but this study adds to an accumulating body of research (some of which I have previously reviewed) that indicates Helicobacter pylori are affecting Levodopa treatment.
And this study was supported by the findings of another recent clinical study:
Title: Eradication of Helicobacter pylori infection might improve clinical status of patients withParkinson’s disease, especially on bradykinesia.
Authors: Liu H, Su W, Li S, Du W, Ma X, Jin Y, Li K, Chen H.
Journal: Clin Neurol Neurosurg. 2017 Jul 5;160:101-104.
PMID: 28704778
The investigators recruited 94 people with idiopathic Parkinson’s disease and they were given a breath test (Helicobacter pylori testing can be done with a breath test, blood test or stool test – click here for more on this). 48 of the participants successfully completed the study.
The participants were put into three groups: Group 1 subjects were Helicobacter pylori negative. Group 2 had Helicobacter pylori positive people who didn’t want to receive the bacteria eradication treatment. And Group 3 subjects were Helicobacter pylori positive and they chose to receive eradication treatment. The Helicobacter pylori infected patients were all given the choice to receive Helicobacter pylori eradication treatment or not. There was no difference between the three groups in sex, age, disease duration, levodopa daily dose and stage of the disease.
One year later, the investigators assessed the motor skills of the three groups. Interestingly, group 3 demonstrated significantly lower motor examination scores (as determined by UPDRS; P=0.007). The differences were mainly in finger tapping (P=0.045), rapid movements of hands (P=0.031) and leg agility (P=0.011). The researchers concluded that the eradication of Helicobacter pylori might improve the clinical status of idiopathic parkinson’s disease.
Again, like the previous study, this study has the issue of the participants being unblinded and selecting to have a treatment or not. The beneficial effect of the eradication treatment could all be due to the placebo effect. The report of the study also does not indicate whether the investigators were themselves blind during the assessment (at 1 year post eradication). It would be very interesting to know this.
Interesting. But do these study tell us if Helicobacter pylori could be actually playing a role in the development of Parkinson’s disease?
No, these small studies are too small and not designed to ask such a question. But a recent large analysis of all the clinical studies investigating Helicobacter pylori and Parkinson’s disease provides some tantalising evidence:
Title: Association of Helicobacter pylori infection with Parkinson’s diseases: A meta-analysis.
Authors: Shen X, Yang H, Wu Y, Zhang D, Jiang H.
Journal: Helicobacter. 2017 Jun 9. doi: 10.1111/hel.12398.
PMID: 28598012
In their analysis of the clinical studies, the investigators found 8 studies which collectively involved 33,125 participants. And interestingly, when the researchers analysed the raw data they found that people with Helicobacter pylori infections were 1.6 times more likely to have Parkinson’s disease than those with no infection (95% confidence interval ranging from 1.37-1.85). The researchers concluded that ‘this meta-analysis indicated that H. pylori infection might be associated with the risk of Parkinson’s disease’.
While this result is intriguing, it is difficult to determine if Helicobacter pylori infections per se are associated with increased risk of Parkinson’s disease, or whether a long term infection of any sort is increasing the risk.
Ok, so what can I do with all this information?
While I do not like to provide advice on this forum, I will say this: if I had been diagnosed with Parkinson’s disease and was a regular reader of this amazingly, spectacular blog, I would probably think about being proactive and discussing with my doctor the possibility of having the Helicobacter pylori breath (or blood) test. A puff of breath or couple of drops of blood would not be too taxing, and it could be useful to know.
What does it all mean?
Previously it was believed that the number of microbes inside us out numbered our own cells by 10:1. This number is now considered an “alternative fact”. New research has suggested that the ratio is closer to even (in fact, ‘the numbers are similar enough that each defecation event may flip the ratio to favour human cells over bacteria’ – Source).
Regardless of their actual number, many of these microbes play a critical role in our general state of wellbeing, while others may be causing trouble. Helicobacter pylori seems to fall into the latter. Gastritis/peptic ulcer, gastric cancer, and increasing the dose of Levodopa required for treating Parkinson’s? Maybe it is time to get rid of these freeloaders!
The banner for todays post was sourced from ehealthtopics

Ok, yes another amazing spectacular blog but I’m a little confused. Is it known how you become infected with HPylori and if you have been treated in the past can you become reinfected (ie should a breath test be pursued if this has occurred)? Is it possible that the micro environment caused by Parkinson’s allows the HPylori to flourish rather than the Hpylori causing/promoting Parkinson’s disease?
Simon great stuff, as ever
LikeLike
Hi Hilary,
Thanks for the comment. They are good questions. I might actually edit the post a little to add some facets of them in.
Helicobacter pylori infection occurs via many of the usual routes for microbes. Drinking, cooking, or bathing in contaminated water may cause infection. Also close interaction between partners, siblings, and parent to child (it can be wise to have a partner tested as well – although this does not really affect reinfection apparently – https://www.hindawi.com/journals/grp/2015/706507/). Having said all this, the prevalence decreases as the quality of life increases – hence the higher rates in the developing world.
The most commonly used initial treatment for eradication is a triple regimen combining a proton pump inhibitor with two antibiotics (usually clarithromycin and amoxicillin/or metronidazole).
Re-infection occurs in less than 15% of cases in the west (https://www.ncbi.nlm.nih.gov/pubmed/16629941), higher in developing parts of the world. But this is being affected by the development of clarithromycin resistant strains of Helicobacter pylori (http://gut.bmj.com/content/59/8/1143).
Regarding the ‘chicken or egg’ question, I’m not sure if this has ever been examined. It’s a good point though and with all the PD research focusing on the gut right now I wouldn’t be surprised if people are looking at this.
I hope this helps.
Kind regards,
Simon
LikeLike