
|
# # # # Today’s post was a joy to write. It is one of those stories that will ultimately become the stuff of legend. And other areas of medical research will come to envy the fact that they don’t have a similar compelling tale. It is such a fascinating story that one feels fortunate to be a researcher living through the period of time during which it is actually unfolding. The background of the narrative is really simple: A lady in an audience made a wonderous association, and then had the courage to publicly ask an odd question (“Why do people with Parkinson’s smell different?“). An intrepid researcher then had the curiosity to follow up on that question, and the resulting findings have opened up amazing new opportunities for us. Recently researchers in Manchester (and their collaborators) have published a series of updates on their research exploring the “smell of Parkinson’s” In today’s post, we will discuss what they have found and how their research could potentially affect our understanding of and approach to Parkinson’s. # # # # |
 Dr Les Milne. Source: BBC
Dr Les Milne. Source: BBC
Dr Les Milne was a consultant anaesthesiologist at Macclesfield in Cheshire for 25 years.
He was one of the first medical directors in the Mersey region, at one point having five departments under his management. Instrumental in changing the training of theatre operating assistants in the hospital, Les was known for giving up his own time to provide extra training to trainees to help them get their qualifications. His was an impressive career.
It is said that beside every great man, there is a great woman, and Les met his when he was 17.
Her name was Joy:
![]() Joy Milne. Source: Telegraph
Joy Milne. Source: Telegraph
When Les was 31 year old, he came home one evening, and Joy noticed something different about him.
Specifically, he smelled different.
“His lovely male musk smell had got this overpowering sort of nasty yeast smell,” she says (Source).
It was a “sort of woody, musky odour” Joy suggests, and she “started suggesting tactfully to him that he wasn’t showering enough or cleaning his teeth. He clearly didn’t smell it and was quite adamant that he was washing properly.” (Source).
Joy, who had trained as a nurse, let the matter go, but as we shall see this simple observation was to have important ramifications.
What happened?
In 1996, at 45 years of age, Les was diagnosed with early onset Parkinson’s.
Five years later, he retired and the couple decided to move back to Scotland. They settled in Perth and quietly dealt with the condition for the next decade.
Then on the 19th April 2012, Joy and Les decided to attend a Parkinson’s UK awareness lecture and it was here that Joy noticed something utterly remarkable.
What was it?
The event involved a young Parkinson’s UK Senior Research Fellow named Dr Tilo Kunath was presenting his research on stem cell biology.
 Dr Tilo Kunath – the man, the myth, the legend. Source: UofE
Dr Tilo Kunath – the man, the myth, the legend. Source: UofE
Dr Kunath is quickly becoming a world-renowned researcher in the area of Parkinson’s-related stem cell biology and he has made a previous appearance on the SoPD (Click here to read that post).
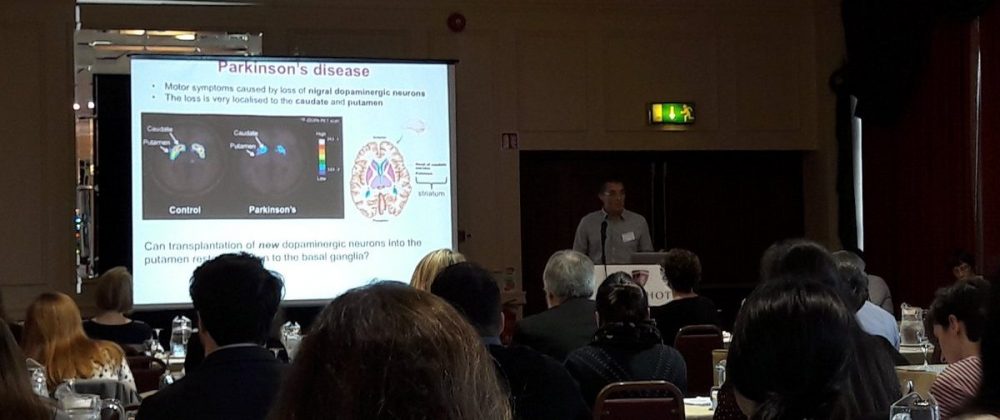 Dr Kunath presenting PD research. Source: Twitter
Dr Kunath presenting PD research. Source: Twitter
At the end of his presentation, Tilo was happy to take questions from the audience and Joy stood up and asked “why do people with Parkinson’s smell different?”
Tilo assumed that the question had been mis-worded and that it referred to the loss of one’s sense of smell, so he pointed out that “People with Parkinson’s often lose their sense of smell“.
But Joy clarified that she was actually asking about body odour, which took Tilo (and the rest of the global Parkinson’s research community!) completely by surprise.
Wait. What? People with Parkinson’s smell different?!?
Joy had arrived at the meeting that day and realised that a significant portion of the attendees at the event smelled exactly the same as Les.
Specifically: All of the folks who had been diagnosed with Parkinson’s had that same “woody, musky odour” that Joy could smell on her husband .
Given this suddenly revelation, Joy decided to take the opportunity of asking an “expert in Parkinson’s” research why this was the case.
One can imagine the scene: Joy sincerely asking a question of personal interest, and poor Tilo (or any other researcher who might have found him/herself in that position) being utterly lost for words or explanation.
To his credit, however, Dr Kunath decided to investigate the matter.
What did he do?
Firstly, he consulted some of his colleagues at the University of Edinburgh and asked if they had ever heard of anything like a “smell of Parkinson’s“?
They all said no, but some of them pointed out that you can sometimes smell diabetes.
 Source: Express
Source: Express
Bad breath (called halitosis) can help doctors to identify diabetes. Diabetes can also make ones urine smell like rotten apples.
And diabetes is not alone in having a distinctive odour. Typhoid is known to turn one’s body odour into the smell of baked bread (Source). And animals – whose sense of smell is superior to our own – can smell a wide variety of medical conditions (for example, dog can smell different types of cancers (Source)).
Armed with this knowledge, Tilo then decided to seek out Joy and he proposed that they do a test.
They recruited six people with Parkinson’s and six people without the condition, and they asked them to wear a t-shirt for 24 hours (sleeping in them as well). The scientists then collected the t-shirts, cut them into pieces and put two pieces from each shirt into separate bags – thus, each shirt was represented by two bags.
 Dr Kunath bagging t-shirts. Source: BBC
Dr Kunath bagging t-shirts. Source: BBC
The bags were coded, with Tilo noting down who had worn which shirt. They then asked Joy to blindly smell the piece of shirt in each bag and tell them who had Parkinson’s and who didn’t. The important detail here is that Joy had no idea who had worn which shirt.
The smell test session lasted 2 hours according to Dr Kunath, and Joy’s nose became sore and inflamed by the end of it.
But the outcome was nothing less than astounding.
What did they find?
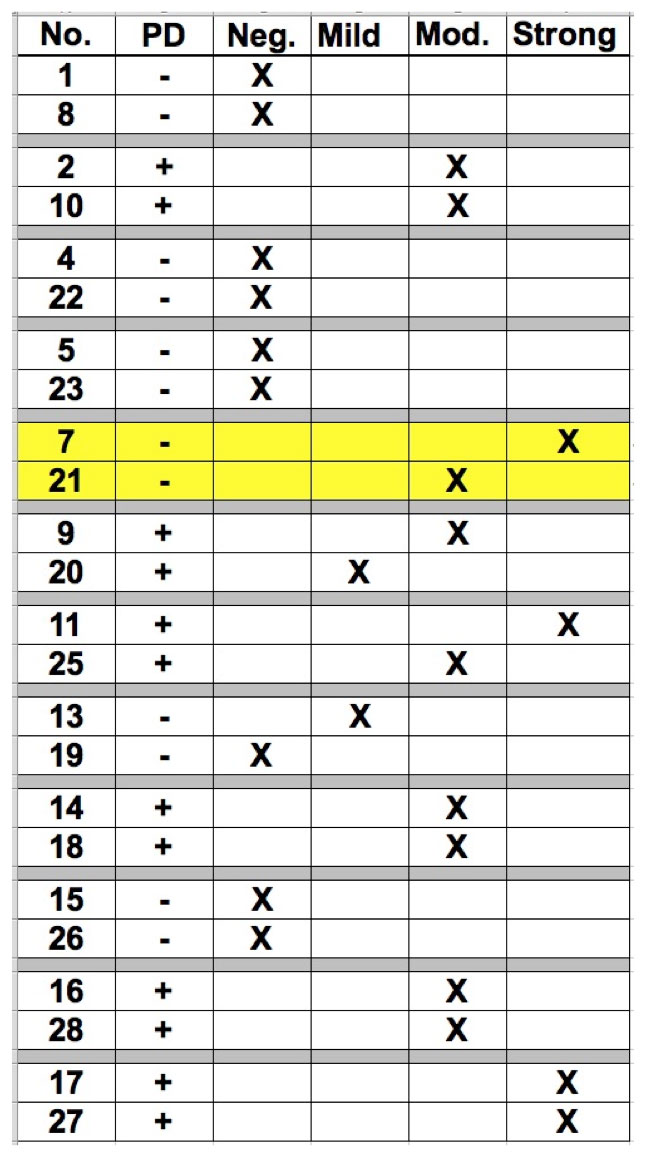
Joy correctly guessed 11 out of the 12 participants.
That is to say, she correctly identified all of the six people with Parkinson’s as having Parkinson’s, and she got 5/6 correct for the control group – a rather amazing feat I think you will agree!
Joy was also adamant that the one ‘control’ participant that she got wrong (the yellow highlighted two rows in the image below – Joy’s answers are represented by a X in each case) also had Parkinson’s. According to the individual in question and the team running the test, however, the subject did not have Parkinson’s.
 Source: Tilo Kunath
Source: Tilo Kunath
But then, eight months later, that same participant informed the scientists that he had just been diagnosed with Parkinson’s.
Pause here and let that sink in for a moment.
Joy had detected the smell of Parkinson’s 8 months before it was diagnosed.
And then think back to how Joy detected a change in body odour in Les when he was 31, only for him to be diagnosed with Parkinson’s at 45 years of age.
Contemplate that for a while.
Naturally, this small experiment attracted a lot of attention, and researchers began designing a study that would help to identify exactly what Joy was smelling.
|
# RECAP #1: Joy Milne asked why do people with Parkinson’s have a different body odour. Research scientist Dr Tilo Kunath answered: ¯\_(ツ)_/¯ but let’s do an experiment. And they found Joy’s ability to smell Parkinson’s to be extremely accurate. # |
A follow up study was proposed to identify which molecules Joy might be smelling. The study was conducted by Professor Perdita Barran and colleagues at the University of Manchester.
 Joy & Professor Barran. Source: Manchester
Joy & Professor Barran. Source: Manchester
And the results of that study were published in 2019:
 Title: Discovery of Volatile Biomarkers of Parkinson’s Disease from Sebum
Title: Discovery of Volatile Biomarkers of Parkinson’s Disease from Sebum
Authors: Trivedi DK, Sinclair E, Xu Y, Sarkar D, Walton-Doyle C, Liscio C, Banks P, Milne J, Silverdale M, Kunath T, Goodacre R, Barran P
Journal: ACS Cent. Sci., 2019, Apr 24;5(4):599-606.
PMID: 31041379 (This report is OPEN ACCESS if you would like to read it)
This study was divided into three stages. The first two stages (discovery and validation) involved samples from 61 people – this group involved a mix of control subjects, people with Parkinson’s on medication, and people with Parkinson’s not on medication (drug naïve). The first stage (involving 30 participants) focused on for volatilome discovery, and the second stage (involving 31 participants) was used to validate the results of the first stage.
Hang on a second. What does volatilome discovery mean?
The chemical compounds that the study was focused on are called “Volatile Organic Compounds” (or VOCs).
 Source: Rabbitair
Source: Rabbitair
These are organic (meaning derived from living matter) chemicals that have a high vapour pressure at ordinary room temperature. They are numerous (there are thousands of them), varied, and ubiquitous (they are all around you).
Most scents and odours you smell are VOCs.
Volatilome discovery involves determining all of the VOCs (and also some inorganic compounds) that originate from a sample being analysed.
The third cohort that the researcher used included three drug naïve people with Parkinson’s. They were used for smell analysis from Joy. Thus, in all 64 individuals were recruited to the study (21 controls and 43 people with Parkinson’s).
Each sampling from all of the individuals involves in the study involved swabbing the upper back with a medical gauze.
Why the upper back?
The early pilot test with T-shirts indicated the odour was present in areas of high sebum production – the upper back and forehead, but not the armpits.
Wait. What is Sebum?
Sebum is an oily/waxy matter that our skins secretes. It lubricates and waterproofs the skin and hair of mammals.

Sebum excretion in the skin. Source: Hair Articles
The researchers suspected that sebum may be the source of the “Parkinson’s odour”.
Why did they think that?
The idea relates to a common feature of Parkinson’s that doesn’t get much attention today.
When the original results of Joy Milne’s pilot experiment were announced, Prof Anthony Lang (at the University of Toronto) pointed out that “one feature of Parkinson’s that we don’t see much of in the era of levodopa treatment is seborrhea. This feature might be related to some metabolite secreted by the glands in the skin” (Source).
 Prof Anthony Lang. Source: Tanz
Prof Anthony Lang. Source: Tanz
What is seborrhea?
Seborrhea is a common inflammatory skin problem, characterised by the accumulation of scales and greasy skin. It causes a red, itchy rash and white scales.
 Seborrhea. Source: Beautypedia
Seborrhea. Source: Beautypedia
Seborrhea has been associated with Parkinson’s, occurring in as many as 50-60% cases (Click here to read more about this). It was also a feature of the condition that noted very early in the research of Parkinson’s:
 Title: The seborrhoeic facies as a manifestation of post-encephalitic Parkinsonism and allied disorders.
Title: The seborrhoeic facies as a manifestation of post-encephalitic Parkinsonism and allied disorders.
Author: Krestin D.
Journal: QJM. 1927; 21(81):177–186.
PMID: N/A
More recently, researchers have proposed that Seborrhea (or seborrheic dermatitis) may represent an early premotor feature of Parkinson’s (resulting from autonomic nervous system dysregulation), and it could be used as an early biomarker of the condition (Click here to read more about this).
Sebum secretion is increased in individuals affected by Parkinson’s, and as – Prof Lang noted above – treatment with L-dopa has been shown to reduce sebum secretion (Click here to read more about this).
Interesting. So what did the researchers find in their “volatilome” study?
The researchers identified 17 candidate compounds, 9 of which were present in both the discovery and validation cohorts, and 4 of which differential present in specific directions between the Parkinson’s and control samples. This provided the researchers with a very distinct combination of VOCs-associated with Parkinson’s, including significantly altered levels of perillic aldehyde (reduced levels) and eicosane (increased levels). This ‘signature’ provided a smell that Joy described as being highly similar to the smell of Parkinson’s that she was detecting.
 Source: Pubs
Source: Pubs
Interestingly, there were no significant differences found between people with Parkinson’s on medication and those who were drug naïve (indicating that treatment byproducts are not being picked up in the sebum).
The investigators acknowledged that the study was limited by small sample size, but the results were still very interesting and provided support for justifying further research.
|
# # RECAP #2: Careful initial investigations found a selection of molecules (called volatile organic compounds or VOCs) in skin swabs from people with Parkinson’s that were associated with Parkinson’s. The results of the study were encouraging enough to support further investigations into the smell of Parkinson’s. # # |
So have further (and larger) analyses been conducted?
Yes. And very recently some of that research has been published:
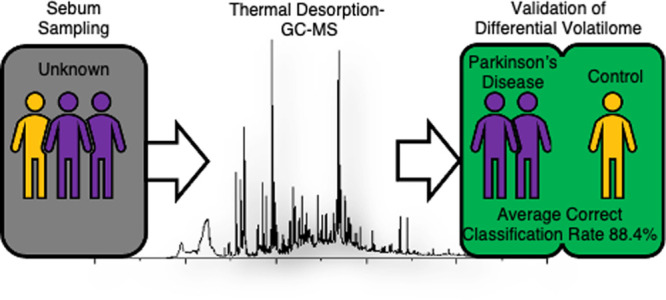
 Title: Validating Differential Volatilome Profiles in Parkinson’s Disease.
Title: Validating Differential Volatilome Profiles in Parkinson’s Disease.
Authors: Sinclair E, Walton-Doyle C, Sarkar D, Hollywood KA, Milne J, Lim SH, Kunath T, Rijs AM, de Bie RMA, Silverdale M, Trivedi DK, Barran P.
Journal: ACS Cent Sci. 2021 Feb 24;7(2):300-306.
PMID: 33655068 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers validated their previously published findings (discussed above) on swabs collected from 100 people with Parkinson’s (both drug naïve and those on PD medications), plus 29 control subjects. They were able to correctly classify 84.4% of the Parkinson’s cases using just the detected volatile compounds from skin swabs.
 Source: PMC
Source: PMC
It is a remarkable number when you consider that clinicians have a diagnostic error rate of approximately 15% (Click here to read an old SoPD post about this). That is to say, 15 of every 100 individuals clinically diagnosed with Parkinson’s are later found to be incorrectly diagnosed.
This was a validation study was conducted using a different instrument as well as a completely new set of patient sebum samples from the previous study.
But the researcher did not stop there.
Today, they have published new data:
Title: Metabolomics of sebum reveals lipid dysregulation in Parkinson’s disease.
Authors: Sinclair E, Trivedi DK, Sarkar D, Walton-Doyle C, Milne J, Kunath T, Rijs AM, de Bie RMA, Goodacre R, Silverdale M, Barran P.
Journal: Nat Commun. 2021 Mar 11;12(1):1592.
PMID: 33707447 (This report is OPEN ACCESS if you would like to read it)
In this study, the investigators analysed skin swab samples from 274 participants, of whom 80 had Parkinson’s but were not on any PD medication (eg L-dopa), 138 were medicated cases of Parkinson’s, and 56 were well matched, healthy control participants. Some of these skin swabs also came from individuals in the Netherlands.
Analysing all of these samples, the researchers replicated their previous finding of being able to differentiate between individuals with and without Parkinson’s (with an accuracy of 85%).
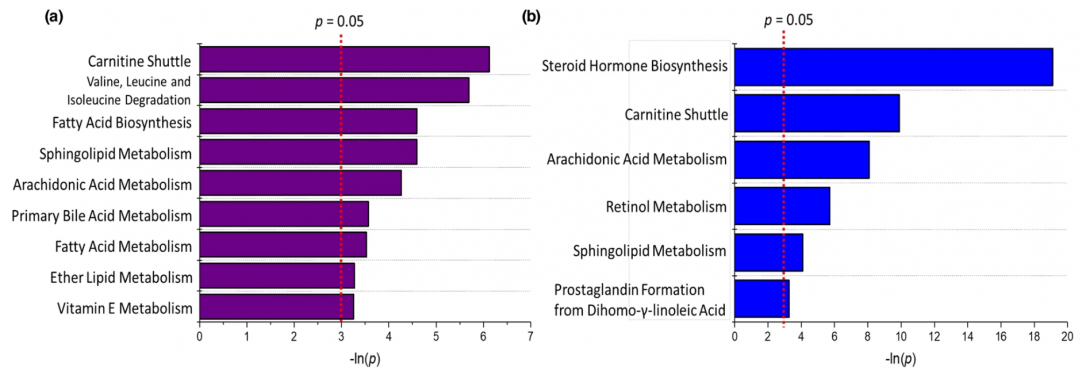
But they were also able to go one step further and they were able to start exploring metabolic pathways that could be affected in Parkinson’s, based on the molecules detected in the skin swab samples. In the image below, graph (a) represents drug naïve cases of Parkinson’s vs. controls and graph (b) displays pathways affected in medicated cases of Parkinson’s vs. controls.
 Source: Nature
Source: Nature
They found that the carnitine shuttle was one of the most significantly affected biological pathways linked to the Parkinson’s swabs in both groups.
What is the carnitine shuttle?
Most cells in our body contain mitochondria.
Mitochondria are the power house of each cell. They provide the cell with energy, which helps to keep the lights on. Without them, the lights go out and the cell dies.

Mitochondria and their location in the cell. Source: NCBI
To make energy, mitochondria require resources, which come in many forms. One of these forms is long-chain fatty acids. But the surface of the mitochondria is impermeable to long-chain fatty acids.
The carnitine shuttle is a mechanism by which long-chain fatty acids are transported into the inner region of a mitochondrion (singular) for the purpose energy production.
For those interested, this video goes deeper into the mechanisms of the carnitine shuttle:
Finding that the carnitine shuttle was one of the most significantly affected biological pathways linked to the Parkinson’s swabs, is an interesting observation as components of this mechanism have previously been proposed as a potential diagnostic markers for Parkinson’s (Click here to read more about this).
The researchers also found that perturbations within the sphingolipid pathway was highlighted in both drug naïve and medicated cases of Parkinson’s.
What is the sphingolipid pathway?
Sphingolipids are a type of molecule in the outer surface of cells. They play significant roles as structural components in the walls of cell as well as being signaling molecules in various regulatory pathways.
They are of interest in Parkinson’s research as they are implicated in the pathogenesis of GBA-associated Parkinson’s (Click here to read a previous SoPD post about this).
It is really interesting that these pathways are popping up in the skin swab analysis of cohorts of both drug naïve and medicated cases of Parkinson’s.
Interesting, but how could this change in smell be occurring?
The simple answer at the moment is we have no idea.
But recently, there have been a series of reports that suggest that particular forms of alpha synuclein – the protein associated with Parkinson’s – are present in the nerves lining the skin in people with Parkinson’s (Click here, here, here, & here to read more about that). It may be that disrupted activity in these nerves could be affecting the secretion of sebum.
Another possibility is that gradual reductions in levels of particular neurotransmitters in the brain (such as norepinephrine) could be affecting levels of other proteins that influence skin regulation. In the absence of norepinephrine (a neurotransmitter similar to dopamine), for example, levels of another protein called α–Melanocyte-stimulating hormone (or just α-MSH) increase significantly. Norepinephrine keeps α-MSH levels under control, but in Parkinson’s – where norepinephrine is reduced – α-MSH levels begin to increase, which in turn increase sebum secretion (Click here to read more about this).
This image below provided by Adrian Wilder-Smith & Dr Kunath demonstrates possible mechanisms underlying the increase in sebum secretion.
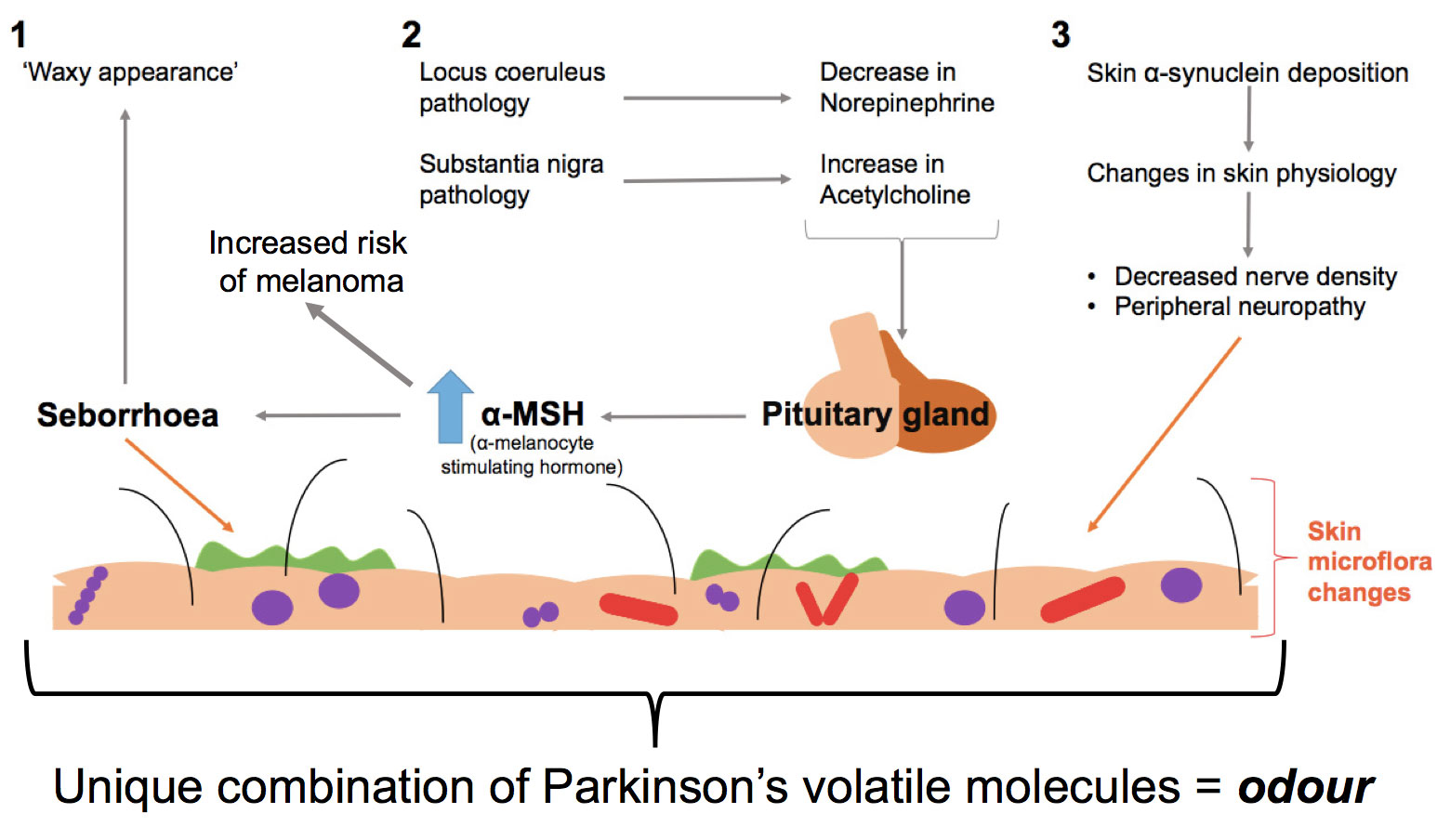 Source: Adrian Wilder-Smith & Tilo Kunath
Source: Adrian Wilder-Smith & Tilo Kunath
But how is this new research actually useful?
The findings open doors to a number of new possibilities.
The obvious application of this research is in providing a diagnostic aid for better determining individuals with Parkinson’s. As mentioned above, clinicians have a diagnostic error rate of approximately 15% (Click here to read an old SoPD post about this). So any tools that can help improve that level of accuracy would be most welcome.
And the research does not necessarily need to result in a new medical device. For example, there are efforts underway to teach dogs to smell Parkinson’s. Manchester University and the research charity Medical Detection Dogs are working on this (Click here to read a previous SoPD post about this).
 Source: Standard
Source: Standard
Once established, it could be very interesting to start including smell detection tests in research focused on the early “prodromal phase” of Parkinson’s.
What is the prodromal phase?
The ‘prodromal phase’ of the condition is the period of time before diagnosis. In Parkinson’s, it involves some of the very early signs of the condition (such as constipation, loss of a sense of smell, and REM sleep disorder), and the very first signs of motor/movement problems (a twitching finger, or a dragging leg).
 Source: Guidelinesinpractice
Source: Guidelinesinpractice
The earlier we can tackle Parkinson’s, the better for society in general.
That is why a considerable amount of research attention is now being focused on this phase of the condition (with studies like PREDICT-PD). And the more we can learn about the early stages of Parkinson’s, the more likely we are to identify new biological pathways that can be targeted in future therapies.
Could an odour test provide a better indication as to which individuals will go on to develop Parkinson’s? And perhaps when they are starting to convert?
But what is the point of early detection if we do not have any therapies to help people who may go on to develop Parkinson’s?
This is obviously a hard question to answer, but the idea of early detection and beginning clinical trials of experimental disease modifying therapies before individuals have even been diagnosed is very appealing.
Such an approach will hopefully lead to better quality of life for the individuals in question, and put less stress on health services and everyone involved in each case.
But what about individuals who already have Parkinson’s?
This new odour research could also lead to a new method of monitoring the condition over time. Larger, longitudinal studies will be required before we will have any clarity on this, but it is an interesting possibility.
So what does it all mean?
During life’s journey we learn a lot about ourselves and the world around us. Much of that learning comes from what has already been learned by others and is passed on to us in the form of teaching and nurture. The rest comes from personal discovery and experience.
One of the exciting aspects of a career in research is the “walking on the moon” aspect of it. That idea that each time you peer down the microscope you might be the first person ever to be seeing something new.
I have often wondered what was going through Joy Milne’s mind as she was walking into the Parkinson’s support group in 2012 and she noticed “the smell of Parkinson’s”. What an exhilarating moment it must have been! That instant of “ah ha!”.
And without that initial insight from a member of the community, researchers may never have considered that Parkinson’s has a smell. As I indicated in the intro to this post, I really love this story. It is one that I’d like to see shared far and wide in the hope of encouraging others to come forward with their own unique observations that may offer us novel insights into this condition.
And I really look forward to future developments of this research.
 All of the material on this website is licensed under a
All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
The banner for today’s post was sourced from NewScientist

Truly fascinating stuff, and I look forward to the next links in the chain that connect sebum perturbations with skin microbiome changes and thence to gut barrier and gut microbiome perturbations. This link has already been made in e.g. atopic dermatitis pathogenesis. See https://www.mdpi.com/2077-0383/8/7/987/htm
Garry
LikeLike
Two years or so before developing a tremor and being diagnosed with Parkinson’s I developed a strange smell. I scrubbed and scrubbed, but it made no difference, so I put it down to a change of aging. But it wasn’t the smell that one usually associates with age (I’m a GP), and I was only 62.
So I was not surprised when I read of this brave lady’s announcement. Yeasty is a good description, yes, and unpleasant too. Well done Mrs Milne.
LikeLike
It’s good to see this story developing. Joy is still busy working for the community including being part of Sparks of Experience https://www.pdavengers.com/blog/sparks-of-experience a project specifically designed to try to capture those unique observations and turn them into novel research. Please get in touch if you have ideas.
LikeLike
makes me wonder if this ties in with the melanoma & PD relationship. I had a melanoma on my upper back excised in 2011 & PD diagnosis 2014.
LikeLike
Simon
Another excellent article!
I have noticed a change in my urine smell. Could this be related?
How do Parkinons Plus syndromes fare in this context? Could someone with PSP for example be diagnosed more accurately and earlier ?
Keith
LikeLike
I have been told that the smell of my urine has changed over the past few months to a yeasty odour, which is unpleasant. But there is no yeasty odour from my skin.
Could the yeasty urine be related to PD.
Peter.
LikeLike