
|
On Saturday 7th January, 2018, one of the world’s largest pharmaceutical companies – Pfizer – announced that it was abandoning research efforts focused on finding new drugs for Alzheimer’s and Parkinson’s. Naturally, the Parkinson’s and Alzheimer’s communities reacted with disappointment to the news, viewing it as a demoralising tragedy. And there was genuine concern that other pharmaceutical companies would follow suit in the wake of this decision. Those fears, however, are unfounded. In today’s post we will look at some of the reasons underlying Pfizer’s decision, why our approach to failure is wrong, why Pfizer will definitely be back, and what the Parkinson’s community can do about it all. |

Photo by David Kovalenko on Unsplash
1. Our approach to failure
I am currently reading “Black box thinking: The Surprising Truth About Success“. It is a really interesting book by journalist Matthew Syed that investigates how we approach to failure.
Matthew Syed. Source: Amazon
In the first chapter of his book, Syed makes comparisons between the way the aviation industry and the medical profession approach failure, pointing out the processes that follow situations when a disasters occur. In the aviation industry, when any event occurs there is a major investigative process that starts with the recovery of the black boxes. The aviation industry uses this system of investigation to learn from every single incident. It makes the information available to all and this helps with re-thinking everything from cockpit ergonomics and design to air traffic controller procedures. Even the airline companies are keen to be seen to be involved in this process of investigation. Failure, while unfortunate, is not shameful or stigmatising, but rather embraced and enlightening.
In addition, Syed points out that when an airline pilot sits down in his/her cockpit, their neck is also on the line if something goes wrong. Thus, it is in their best interest that the flight should be successful. And this is another reason why the aviation industry takes the reporting of failure so seriously. Everyone benefits from learning from previous situations. And all of this comes together with the observation that 2017 was the safest year on record for flying (based on deaths/flights – Source).
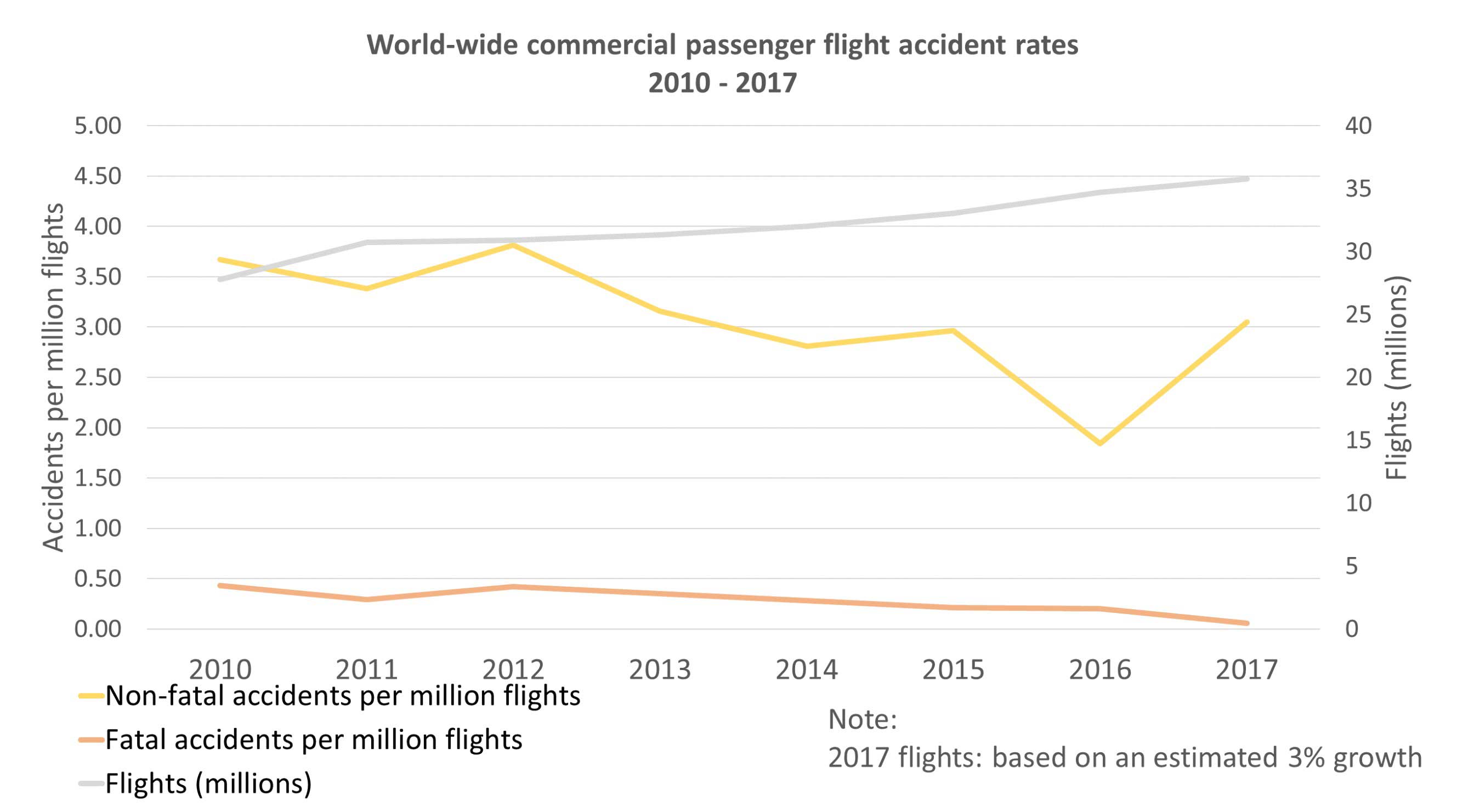
Note the downward trend on the orange line (deaths) despite the upward trend on number of flights (grey). Source
Now compare that with the medical profession, which Syed does in the first few pages of his book with a horrific real life case study. When medical incidents occur (and unfortunately they do), there has previously been little in the way of investigation or feedback to improve practice – as Syed outlines in his book. In addition, it is very difficult for members of the public to access any of the information. And this is particularly evident in the setting of clinical trials, where even when drugs are successful in the clinical trial process there is very little actual reporting of results beyond the major media headlines.
Of the 224,000 clinical studies registered on the National Institutes of Health (NIH) ClinicalTrials.gov website, only 23,000 of them actually display results information (Source).
That is less than 10%!
And the failure to report clinical trial results has previously put the general public at risk. For example, in 2012 the pharmaceutical company GlaxoSmithKline paid $3 billion after it failed to disclose trial data demonstrating that its antidepressant Paxil was not only no more effective than placebo during their trials, but that it was also linked to increased suicide attempts among teenagers (Source).
Admittedly there are now efforts and policies being put in place to correct this (such as a major change in the rules regarding the reporting of clinical trial results – Click here to read more about this), but the medical profession is still woefully behind the aviation industry in embracing and investigating failure.
‘But medicine is more complicated’ some will say.
Boeing 747-400. Source: FAIB
The Boeing 747-400 has over 6 million parts. That sounds pretty complicated to me. It also contains 171 miles (274 km) of wiring and 5 miles (8 km) of tubing (Source). And while there are contingencies built in (thanks to a process of failure investigation), it is helpful when each of the 6 million parts does exactly what is it supposed to do. Years of feedback on every single system has resulted in better success with regards to passenger safety. And it has also resulted in improvements to the system of reporting, for example as Syed points out that the black box recoding systems are no longer black, they are now pink to help visually locate them better (and they collect a lot more information than they used to as well).
This proactive approach to failure overshadows the strange path that the pharmaceutical company Pfizer took on the 7th January 2018. Their announcement that they were terminating all research focused on finding new drugs for Parkinson’s and Alzheimer’s disease was accompanied by the removal of all of information on their website dealing with the topics of neuroscience – go to their ‘Therapeutic areas‘ page, neuroscience is gone (as if it never actually existed). The one page that still exists for Parkinson’s disease (Click here to see it… before it too disappears), is actually an article borrowed from the Gethealthystayhealthy website. Admittedly you can still search their website for Parkinson’s, and this provides a list of the contact details regarding previous clinical trials (Click here to see those search results), but there is precious little in feedback regarding what happened in any of those trials.
It should be said that Pfizer is not the first pharmaceutical company to removed content from their website following such a decision, but this sort of industry practice only highlights the lack of constructive learning-based feedback that the aviation industry encourages.
To their credit, Pfizer’s has provided an explanation about why they made their decision.

Dr Mikael Dolsten. Source: Twitter
Dr Mikael Dolsten, M.D., Ph.D., President of Pfizer Worldwide Research and Development, outlined in the company’s explanation on the Pfizer website (Click here to read it), that:
“This decision was driven by science; not cost. As the fourth largest investor in pharmaceutical research and development worldwide, we expect limited impact, if any, to our overall investment in R&D as a result of this decision. Our reallocation of funding will allow us to place greater focus on areas where we believe we have the strongest possibility of bringing important therapies and vaccines to patients in the near term.”
This explanation is both reasonable and nonsensical at the same time.
It is reasonable because, yes it is in the best interests of the shareholders for Pfizer to focus on what it believes it does best. However, if the decision is not going to have an material impact on the “overall investment in R&D” then why make it at all? If neurological conditions make up such an inconsequential component of R&D, why not simply continue research on them?
But more importantly:

Source: Fortunepr
Why make this decision/announcement in such a public fashion?
Why would any company alienate itself by making such a demoralising decision for a large community that it claims to care for? The share price did not jump in the following days, so there was no financial gain for investors. Why wouldn’t Pfizer just quietly and slowly wind things down and avoid the negative press? As far as public relations disasters go, the Pfizer announcement was exemplary and one can foresee future MBA students using it as a case study in how things should not be done.
If we are going to celebrate the rewards and successes of this industry (for example, Dr Mikael Dolsten was the 2016 winner of the Foundation for the National Institutes of Health award honouring 20 years of support for advancing biomedical research – Source), then we should also embrace the failures and learn as much as we can from them as a community. All the information (minus the sensitive intellectual property) should not be deleted from a company’s website, but rather be made available for scrutiny. Only this way, can we all move forward.
And as the airline industry has demonstrated, this more proactive approach is in everyone’s best interest.
2. An inconvenient truth: Brain actually is hard 

The reality of neurodegenerative clinical trials? Source: Schumpetercentre
The history of drug development for brain-related conditions has thus far been a story of chance and cosmetics.
Many of the drugs that we use for neurological conditions started out their lives as potential treatments for other conditions. For example, the first antipsychotic, called Thorazine, was originally tested as a sedative in the 1950s. It failed as a sedative, but when given to people with schizophrenia it miraculously stopped their hallucinations and the research community was able to notch it up as a break through treatment for psychosis. Similarly, the first antidepressant, called Imipramine, started out being paraded around as an all new type of antipsychotic. It also failed, but clinicians kept on using it when they noticed that it seemed to improve the mood of individuals taking it. While the skilful observations of the clinicians testing the drugs allowed for them to be re-oriented to alternative uses, it was extremely lucky for the companies developing those drugs that they were not costly disasters.
In addition, most of the brain-related, blockbuster drugs of the past have been based on the idea of simply treating symptoms rather than the underlying condition. For example, do you want to make depressed people feel better about themselves? Just juice them up on neurotransmitters like serotonin (most antidepressants). People with Parkinson’s have reduced levels of dopamine? Just boost their dopamine levels (Levodopa). Most antipsychotics work on the simple idea of blocking the dopamine D2 receptor. These rather blunt instrument approaches to ‘solving’ complications associated with the brain, however, do not really address the mechanistic problem associated with the brain. Rather, they just cover them up by reducing the symptoms.
Actually ‘solving’ the complications associated with the brain, like neurodegeneration, has proven to be a very hard task.
Over the last 20 years, the pharmaceutical company Pfizer has funded 99 clinical trials for 24 drugs that were being tested in the treatment of the neurodegenerative condition, Alzheimer’s. Each one of those drugs was touted at some point as a potential game changing ‘blockbuster’ product, that would not only stop this terrible form of dementia but also generate the company billions in much desired profits.
Only one of those 24 drugs was ever approved for clinical use by the US Food and Drug Administration (FDA).
That drug: Donepezil (marketed under the trade name Aricept).

Aricept. Source: Yourlawyer
Donepezil (a acetylcholinesterase inhibitor developed by Eisai, which Pfizer bought the rights to commercialise until July 2022 – source) has shown the ability to improve cognitive functions and behaviour in people with Alzheimer’s, but does not slow or cure the disease (and this drug has also caused some controversy – Click here to read more on that). But Donepezil is one of few outliers in the very large field of Alzheimer’s drugs. Between 2002 to 2012, a total of 244 compounds were tested in clinical trials for Alzheimer’s.
Just 1 of those 244 drugs received FDA approval (that one drug: Memantine).
This translates to a 0.4% success rate for Alzheimer’s drugs during that period (Source), compared with 19% for cancer drugs. To date there have been only five drugs approved by the FDA for use in treating Alzheimer’s (Source), and only four of them remain on the market.
The high rate of failure for experimental Alzheimer’s drugs is extremely discouraging, but it also comes with an enormous monetary cost: these massive clinical trial programmes required for attaining regulatory approval are extremely expensive.
For example, in 2009 Pfizer, Elan, and Johnson & Johnson – three large pharmaceutical companies – teamed up to fund a much-hyped Alzheimer’s drug through the clinical trial process. When the drug – Bapineuzumab (or simply ‘Bapi’) failed crucial phase III trials, the companies collectively wrote off more than $500 million in associated costs (Click here to read more about this).
And remember, Pfizer has done this for 23 different drugs that have all failed.
Like I said: Expensive

A lost cause? Source: Pixabay
The sheer cost of these clinical trial programmes is one of the reasons that some large pharmaceutical companies have no Alzheimer’s projects.
No Parkinson’s projects.
No Huntington’s or motor neuron disease projects.
In fact, nothing to do with brain at all.
For example, the Pharmaceutical company Bayer (the world’s 10th-largest independent biotech company with a market capitalisation of $100 billion) has no drugs for brain-related conditions in clinical trials:
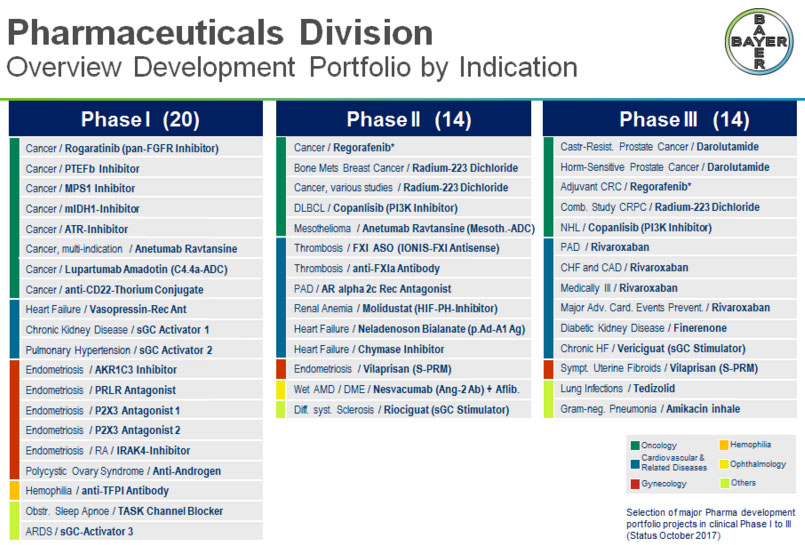
Bayer’s clinical trial pipeline in October 2017. Source: Bayer
The pharmaceutical company Gilead also has no neuroscience-related clinical trials in its pipeline (Source). Even the massive GlaxoSmithKleine has only one “neuroscience’ clinical trial, but that is for a degenerative condition of the eye (IONIS-GSK4-L – Source). The last Alzheimer’s drug that GlaxoSmithKleine was actually developing (called RVT-101/Intepirdine) was sold in December 2014 for $5 million to a company called Axovant Sciences… which was the same biotech company that announced late last year that Intepirdine had failed in a phase III clinical trial for Alzheimer’s (Click here to read more about this). Did GSK dodge a bullet? For an excellent OPEN ACCESS review of the current state of the Alzheimer’s clinical trial pipeline: Click here.
The announcement by Pfizer on the 7th January that it was abandoning research efforts focused on finding new drugs for Alzheimer’s and Parkinson’s was an admission of an inconvenient truth: Brain is hard.
A weak excuse?
“But why, some say, the moon? Why choose this as our goal? And they may well ask why climb the highest mountain? Why, 35 years ago, fly the Atlantic? Why does Rice play Texas?
We choose to go to the moon. We choose to go to the moon in this decade and do the other things, not because they are easy, but because they are hard, because that goal will serve to organise and measure the best of our energies and skills, because that challenge is one that we are willing to accept, one we are unwilling to postpone, and one which we intend to win, and the others, too”
John F Kennedy, September 12, 1962

JFK. Source: Parade
Say what you like about JFK, but his ‘Moon speech’ at Rice Stadium in 1962 was on the mark. We don’t succeed because we only do easy things. If we only did the easy stuff, we would still be sitting in caves.
It is not a case of doing what we can. The way forward has always been shown to us by people doing what we can’t. Think Elon Musk: everyone said electric cars will never work, and now all of the major car makers are racing to catch up. The space veterans told him that SpaceX would never fly, and now the company is planning to head for Mars.
And this philosophy is particularly apparent in the creatives on the internet who have been changing the way the next generation create and consume content:
Finally snuck a Casey Neistat video into a post!
The research community also embraces this philosophy. Every day new discoveries are being made because we step up to the challenge of trying to do what was previous considered impossible.
Even individuals within the Parkinson’s affected community step up to the plate and attempts to “do what you can’t”:
If Pfizer (or any other pharmaceutic company) choose to only do what is easy, then that is their call. But you have to admit that their choice certainly flies in the face of Charles Pfizer’s original vision to “innovate every day to make the world a healthier place“.
Charles Pfizer (1824 – 1906). Source: Wikipedia
Yes, brain is hard, but that only serve as a rallying cry for those who want to make a difference in the world.
It is not a call to retreat.
3. Pfizer had very limited resources focused on Parkinson’s
If we are completely honest the response to Pfizer’s announcement has been over done, for one very simply reason: Pfizer has never really been very big on Parkinson’s.
In December 2016, Pfizer had 96,500 members of staff across 46 countries. In their announcement on 7th January, Pfizer said that it was dropping about 300 employees in Connecticut and Massachusetts (100 each in Andover, Groton and Cambridge). While the loss of employment for these individuals is unfortunate (rest assured that research scientists are not paid as much as the high flying sales execs), the number of jobs represents only a tiny fraction of the research effort at Pfizer.
The research effort at Pfizer has never really been very focused on neuroscience (and most of their main brain-related drugs were gained by acquisition and not R&D). As of October 2017, Pfizer listed seven experimental neuroscience drugs in Phase 1 or 2 testing (only Tanezumab was in phase III; Source). Now, compare that to the 24 experimental drugs Pfizer had targeting cancer. Four of the brain-related clinical programs were aimed at Alzheimer’s and just one targeted Parkinson’s. The Parkinson’s clinical trial programme was for a drug called PF-06649751 – a dopamine D1 receptor agonist. And this was not going to be a disease modifying drug, nor a novel treatmet (there are already many dopamine D1 receptor agonists available – Click here for a list). Thus, the lost of this particular drug is not the end of the world.
On the NIH ClinicalTrial.gov website (a database of all registered clinical trials), Pfizer had 19 clinical trial registered for Parkinson’s dating back over the last two decades. This might sound like a lot, but 8 of those trials were for just one drug (PF-06669571 which was another dopamine 1 receptor agonist) and 3 other trials were for Sumanirole (a dopamine D2 receptor agonist that the company dropped in 2004, citing “recent studies that failed to sufficiently distinguish Sumanirole from currently available therapies” (Source). Sumanirole was originally developed by Pharmacia & Upjohn, which Pfizer acquired in 2002).
Long story short: Pfizer has never really been very big on Parkinson’s.
And this is evident when you look at some other pharmaceutical companies that are focused on Parkinson’s, such as Merck (which has had 20 clinical trials registered for Parkinson’s), Novartis (23 trials for Parkinson’s), and AbbVie (25 trials for Parkinson’s).
The Parkinson’s (and Alzheimer’s) community has worried, however, that Pfizer’s decision would lead to other large pharmaceutical companies following Pfizer’s lead (not the red faced PR disaster, but by walking away from neurodegenerative research).
But I think (personal opinion here) that this worry is unfounded.
4. Pfizer isn’t stepping away completely, nor for very long
In their announcement, Pfizer did stress that late-stage development programmes for Tanezumab (a monoclonal antibody against nerve growth factor for the treatment for pain which was originally developed by Rinat Laboratories and acquired by Pfizer in 2006) and Lyrica (also known as pregabalin – a chronic pain drug, developed by Parke-Davis and acquired by Pfizer in 2000… anyone else noticing that Pfizer acquires a lot of their drugs?), as well as rare disease programmes in the neuromuscular or neurology area, would continue to be supported.
This is reassuring because:
A.) It means that Pfizer is not stepping away from neuroscience-based clinical trials completely. They are simply stepping away from the conditions that they consider too hard.
B.) The recent decision by the US Government to cut back on the Orphan Drug Designation program in their new tax plan (Click here to read more on this) has not caused a company like Pfizer to walk away from their own rare disease projects.

The United States Capitol. Source: SpotHeroBlog
The company also announced that in lieu of doing actual research in the field of neuroscience, Pfizer would set up a dedicated neuroscience venture fund to support efforts to help advance progress.
“We recognise that neuroscience is an area of tremendous unmet need for patients and we plan to create a dedicated neuroscience venture fund to support continued efforts to advance the field. More details on the fund will be forthcoming this year.”
They were, however, short on details of this new fund (simply saying that there would be more details later in the year).
But Pfizer, like all of the big pharma companies simply can’t afford to walk away from neurodegenerative conditions.
And here’s the business reason why:
The United States spent roughly $259 billion on health care expenses related to Alzheimer’s disease alone in 2017, with Medicare and Medicaid covering about 67 percent of that money (Source). And these expenses are only going to increase as the population ages and the affected community grows.

The projected cost of dementia (note the tiny red bars). Source: UCSF
And this growth rate is a key driver for most pharmaceutical companies in their efforts to provide therapeutic products for conditions like Alzheimer’s.
Total spending on medicines is forecast to reach $1.5 trillion by 2021, up 33% from 2016 levels. But this growth rate is actually down from the recent high growth rates in 2014 and 2015, according to a recent analysis by IQVIA (Source). Medicine spending will grow at a 4% to 7% compound annual growth rate during the next five years (2016–2021), down from the nearly 9% growth level seen in 2014 and 2015.
Neurodegeneration (particularly dementia and Parkinson’s), however, represents a major growth opportunity for the pharmaceutical companies, as growth in other areas of healthcare slows. To ignore this is only going to be detrimental to a company’s long term prospects.
Thus, Pfizer can step away from neurodegeneration and have a breather for a while if they think that a wise move, but they will most definitely be back. They literally don’t have a choice on this matter.

Source: Geektyrant
And there is another aspect of this that needs to be appreciated by the affected community.
Throughout this post, I have pointed out that most of Pfizer’s brain-related drugs were gained via acquisition rather than in-house R&D. And Pfizer is not alone in this regard, most of the big pharmas rely on this strategy for new products.
Currently the largest selling pharmaceutical product in the world is a drug called Adalimumab (also called Humira) with annual sales of over US$ 14 billion (Source).
Adalimumab/Humira. Source: Medscape
Adalimumab is a TNF-inhibiting, anti-inflammatory drug that is used to treat a wide range of inflammatory conditions, including rheumatoid arthritis, psoriatic arthritis, and Crohn’s disease. The drug is sold by the pharmaceutical company AbbVie. But Adalimumab was not developed by AbbVie. It was originally discovered during a collaboration between two much smaller biotech companies called BASF Bioresearch Corporation and Cambridge Antibody Technology. The rights to Adalimumab were purchased by the original parent company of AbbVie, called Abbott Laboratories – which was split into two companies in January 2013.
And this is a common theme if you make you way down the list of top selling pharmaceutical products (Click here to see the list). A small biotech finds an interesting compound and tests it to the clinical phase I or II stage and then a larger pharmaceutical company comes in and takes over. If the drug is particularly interesting, the pharmaceutical company will typically buy the smaller biotech outright in order to own the intellectual property, and then take the drug through the larger phase III clinical trials in order to get the product to market. And this is the life cycle that a lot of biotech investors rely on.
And this life cycle is playing out as I write this with news that Parkinson’s focused company Acorda Therapeutics is in take-over talks with neuroscience-focused pharmaceutical company Biogen and UCB (despite the termination of their lead drug Tozadenant for Parkinson’s, Acorda’s inhalable Levodopa product, Inbrija, makes this company very attractive for a neuro-focused pharma seeking innovative new products).
All of this is to say: it is generally not the large pharmaceutical companies that discover the really innovative new products.
They will provide us with new and interesting variations of old products (for example, the diabetic drug Exenatide being turned into Bydureon), but they don’t usually do the major discovery work. Given this situation, companies like Pfizer should be doubly down on neuroscience rather than retreating. There are a host of novel therapeutic approaches being developed by smaller biotech firms that Pfizer should be considering, and planning to provide future variations on rather than shutting down their own neurodegenerative research facilities.
A bit of foresight is required.
5. Addressing the problems

New opportunities. Photo by Tanja Heffner on Unsplash
In every problem there is opportunity.
Thus, the question we should be asking ourselves is what can we do to improve this particular situation? It is wrong to rely on the Pharmaceutical companies like Pfizer to invent new therapies. As indicated above, history has demonstrated that the smaller, innovative biotech firms provide the new drugs. We must thus try to increase the chances of success for these pharmaceutical companies at the expensive phase II or III stage of neurodegenerative drug development.
And how exactly do we do that?
My 2 cents (again, personal opinion here) is that we have two problems reducing our chance of success:
- Our approach to understanding the underlying mechanisms of these neurodegenerative conditions is apparently flawed
- Our systems of measuring, assessing and tracking these conditions is woefully inadequate
On the former, as I mentioned early in this post, much of our past success in brain-related research has been due to chance. Thus, we need to increase our amount of luck. How do we do that? We need to do more (“The more throws of the dice, the more chances to win” the casino man said to me). But key to this approach is not having everyone in the research world chasing after the same targets.
And this is particularly apparent in the Alzheimer’s field where currently 60% of Phase III experimental drugs and 100% of Phase II/III therapies in clinical trials are targeting one of just three targets: beta-amyloid, tau or cholinergic pathway proteins. In fact, therapies targeting beta-amyloid alone still make up about one-fifth to one-third of the products in early clinical and preclinical development (Source – this is a really interesting article on this topic). This is crazy. Particularly because thus far all of the beta amyloid therapies tested in clinical trials have failed (click here to read more on this), resulting in a major re-think of our understanding of Alzheimer’s.

Source: Blackandretired
All our eggs should not be in just one or a few baskets. We would increase our chances of luck, simply by increasing our number of baskets. And by doing this, we would hopefully also increase the chances of success for the pharmaceutical companies.
But this can not occur in isolation.
Many of the Alzheimer’s/Parkinson’s drug trials that have failed have called for better methods of assessment. And this issue of ‘measuring, assessing and tracking’ is particularly critical at present for the Parkinson’s community. We have multitudes of potential drug treatments lined up and waiting on the side line for clinical testing, plus a wave of potential new targets each year. But the real issue is that we need better methods of individual assessment and monitoring. We can not clinically test all of these novel therapies relying solely on monthly clinical assessments (such as UPDRS) and 12 month brain imagings (DAT-scans). Some of these drugs may have very specific effects which will not picked up by either of these approaches.
In addition, these methods of assessment are not without their own issues. Intra/inter-rater reliability of UPDRS clinical assessments is too debatable to be the primary end point (Click here to read more on this), especially in large phase III trials where multiple research centres involve dozens of clinicians conducting the assessments. And the brain imaging is simply too expensive and specifically localised for large scale tests. Requesting participants to go OFF treatment for 12 hours before brain imaging and travelling to the imaging facility during that time is a lot to ask of individuals.
New objective methods of assessment would be very welcomed by all of the neurodegenerative community.

Could wearable technology help with assessment? Source: Forbes
And this is where the Parkinson’s affected community can play a major role, by suggesting ideas and calling for funding that is specifically focused on tools for monitoring/assessment. The ideas would involve direct consultation with the Parkinson’s community. This is how research efforts around the idea of ‘smelling Parkinson’s’ have arisen – Joy Milne in Scotland stood up at a support group meeting and said “I can smell Parkinson’s” (click here for more on this):
We need to think about really left field ideas.
Blood tests, breath tests, smart phone apps are all currently being tested. We need to think about alternatives (such as smart pills – click here and here to read more on this). And really ‘objective’ approaches are required – rather than ‘subjective’ (“how are you feeling today?”) methods which are difficult to score and quantify. Objective approaches that individuals can not affect or bias via any placebo effect.
The ideal system would involve continuous measurement, while allowing individuals to go about their daily lives.
Have a wee think about it. We’ll come back to this idea at a later date.
In this post I have tried to layout my thoughts not only regarding the Pfizer decision, but also issues that plague the field of clinical trials for neurodegenerative conditions like Parkinson’s. While I have focused much of my fury on Pfizer and their course of action, I have not intended it to be a negative statement on a company that has in the past provided many useful medical treatments. If the company or any readers object to anything I have written or have some constructive ideas regarding the material posted here, they are free to comment below or contact me directly. I would be happy to be corrected on any errors in my thinking or any content in this post. It would be to the benefit of all.
There are two outstanding questions that I haven’t found answers for regarding the Pfizer announcement:
- What the company plans to do with their options on GDNF for Parkinson’s (Click here to read about this)
- What happens to ‘Project BlueSky’ – the collaboration between IBM and Pfizer that was focused on developing new tools for measuring Parkinson’s symptoms/features (in the hope that they could aid future clinical trials – Click here to read more about this).
Efforts have been made to reach out to folks involved with both of these matters, but no responses have been had. If anyone has any information regarding this, please let us know – I for one am very curious.
Long rant.
I think I’m done.
EDITORIAL NOTE: Pfizer and many of the other companies mentioned in this post are publicly traded entities. That said, the material presented on this page should under no circumstances be considered financial advice. None of the material presented here should be considered an endorsement of any company (nor a recommendation to sell/short a particular stock). Any actions taken by the reader based on reading this material is the sole responsibility of the reader. None of the companies mentioned on this post have requested this material to be produced. Nor does the author have any financial interest in any of the companies mentioned. This post has been produced for educational purposes only and the bulk of the opinion provided here are those of the author.
The banner for today’s post was sourced from the Independent

thanks, simon. so interesting. and i’ve read that u.s. hospitals are getting into drug r&d due to frustrations with price gouging. i didn’t realize big pharma relied so much on others’ brilliant research.
the statistics about clinical trials are sad, but it seems to be a bit of a hot topic lately, so maybe there’ll be some reforms. as a subject in two trials (one done and one ongoing), i enjoy it but find it frustrating that researchers are so secretive about the data they have, e.g., blood tests. no one wants to share any insights about progression, severity, or prognosis. i feel like i have to scour the web for tidbits of information. sorry, now i’m on a rant — but i do appreciate how well you explained this, and enjoyed your inspired illustrations : )
LikeLike
Hi Beetheaven,
Thanks for your comment, glad you liked the post. I have a lot of respect for folks who get involved with clinical trials.
We are gradually moving away from the old rigid style of clinical trial and into the brave new world of adaptive trials. So rather than simply testing whether a drug works of the average person with Parkinson’s (better than a placebo/control treatment), we will start testing drugs on each individual. And the trials will be adaptive in that the data will be analysed during the study (and not just at the end) and decisions will be made based on those results during the study. So rather than a participants in a trial staying on one drug for the entire period of the trial (even if there is no benefit), they could be shifted to another drug during the trial which could have benefits for that individual. There is the risk of placebo effects in these sorts of studies, so they will need to be designed very carefully. But this is where things are hopefully heading, a more dynamic clinical trial design focused on the patient rather than the drug.
As for researchers sharing the information: during the trial it would be impossible (the possibility of influencing the participant), but after the trial it should be mandatory (and as I suggested there are efforts under way to improve this). And with an adaptive trial design there would be the possibility for REAL feedback about what worked and what didn’t work for each individual. Useful information for each participant. Fingers crossed that ‘the powers that be’ don’t drop the ball as we head in this direction. Maybe we should simply hire some of the aviation industry guys and ask them to help be part of sorting the situation out.
Thanks again for your comment.
Kind regards,
Simon
LikeLike
Simon
Another excellent thoughtful piece.
I think that the prospect of smart phone based assessment methods would hold the best hope of a large data catchment for researchers.
Regards
Keith
LikeLike
Hi Keith,
Thanks for your comment. Glad you liked the post. Smart phone apps would certainly be the easiest option to roll out, but I worry about issues like ‘practice effect’ with some of the tests on them (such as finger tapping). One could get better at these things, just by practicing rather than any particular treatment. But the motion detection/activity measures could be very useful. Food for thought.
Kind regards,
Simon
LikeLike
Thank you, Simon, for yet another well-thought through and clearly explained article. It is very interesting to see how the big companies rely so much on other, smaller R&D companies or university spin-off organisations. I help raise funds for Parkinson’s UK and would prefer to see these funds being allocated to innovative local research groups. But as you say, the key issue is about coming up with an accurate means of assessing the impact of the proposed treatment. I would be happy to be given an Apple smart wristwatch to record daily ups and downs etc! And the PD Warrior exercise programme has a good method of measuring progress made physically over the 10 week assessment period, which could be incorporated into a new overarching and objective monitoring system. Cheers – keep up the good work! Ken
LikeLike
Hi Ken,
Thanks for your comment – I hope all is well. I would also be happy to be given an Apple smart wristwatch! I have been meaning to look into the PD Warrior programme – thanks for the idea!
Glad you liked the post.
Kind regards,
Simon
LikeLike
Great post as usual.
I am wondering what the advantages might be for earlier detection of PD (for example, via smell)?
LikeLike
Hi KJJ_me,
Given the lack of effective treatment options, early detection is still a difficult beast to tackle. An early diagnostic test would be useful, but without the treatment option I’m not sure anyone would want to take that test. And this hypothetical situation may become a very real ethical dilemma later this year if the smell analysis results for the ‘Joy Milne smelling PD” study get published and they point towards specific biomarkers of early PD.
Having said all that I am currently writing a post on exercise and PD, and there are signs there of particular regimes having beneficial effects. Plus we have a host of clinical trial results which will be publishing results in the near term that may offer disease-slowing options (fingers crossed). So maybe there could be treatment options at the same time as an early diagnostic test becomes available. Here’s hoping.
Kind regards,
Simon
LikeLike
Could there be a connection between the recently passed US tax plan in Pfizer’s decision – because an article I read said they were going to do a stock buyback which perhaps only makes sense in the context of the new tax schedule?
LikeLike
Hi Marc,
Thanks for your comment. Yeah, I was also wondering if there was something going on in the background. I haven’t read anything suggesting this though. And I think the neuroscience division was not really big enough to have a major impact on buy-back schemes. Strange, however, that the decision to shut everything down came so quickly. Their neuroscience division certainly walked a strange path recently (In 2016, Chief Scientific Officer of the Neuroscience Michael Ehlers jumped ship to be head of R&D at Biogen, and Pfizer brought in Prof Ole Isacson to take over, but he lasted less than 9 months), but this still doesn’t explain the crazy announcement to terminate it all.
What article were you reading? I would be curious to hear what others think.
Kind regards,
Simon
LikeLike
Hi Simon, it may be a rant, but it’s an excellent and well-balanced one. I’m not perturbed by Pfizer’s decision; pharma companies make portfolio balancing decisions all the time. If they feel they can’t win in a particular therapeutic area, then it actually doesn’t do patients good in the long run if they carry on raising hopes and wasting money.
There are still some big companies involved, plus many more small and medium sized ones to keep us Parkies encouraged. Given the dynamics of the disease, with aging populations, it’s still an attractive “market” for pharma.
I’m more concerned that we are dealing with a heterogeneous disease (dare I say almost a syndrome?); that is assessed subjectively; that is highly variable both inter- and Intra- subject; that potentially has unrepresentative selection in clinical trials; that struggles for valid reasons to design disease-modifying trials. Maybe we need to pause and reach some kind of consensus on the way forward as industry/researchers/patients to ensure the next waves of investment aren’t wasted.
Kevin
LikeLiked by 1 person
Hi Kevin,
Thanks for the well considered comment – possibly the best comment this site has ever had. You touch on so many points and I think you are absolutely right on most of them (so much so that I would encourage you to expand on them in a separate piece – maybe on the PDUK medium page? – in order to generate more discussion about this). I am particularly in agreement with you regarding the last set of comments on the heterogeneity of the condition. I often think that one of the reasons PD drug trials may be failing is because we are focused on which drugs work better than placebo for the average PD sufferer. Pray tell what is the ‘average PD sufferer’? Even if a drug works for some participants in a particular trial, that minor success is ignored because the average barely shifted within the rest of the heterogeneous population.
While I appreciate the discipline and unbiased structure of a randomised clinical trial, the RCT only really works if one is testing a single variable (AKA the drug). But in every clinical trial there are a bunch of other variables (called the participants) that need to be considered. I am increasingly thinking that our attention is misplaced: Rather than focusing on the drug, we should be focusing on the individual. And this is why the need for adaptive clinical trials is so great. But our methods of assessment still need to be addressed. We may have drugs that help with a specific aspect of PD, but that benefit is not picked up by UPDRS or a DATscan. I’m ranting again. Apologies.
Thanks for your thoughts,
Simon
LikeLike
Hi Simon, thank you very much for the kind comment, this is definitely worth following up. Kevin
LikeLike
Simon, As others said, thank you for another thoughtful article. I’d like to follow up, though, on comments you made above about writing an article on exercise and what to do if one receives a diagnosis prior to having symptoms.
First, I have commented on this site before and spoke of my routine, but I would like to add a little more color to my approach. I am aware that the links I provide are already on your radar, but I’d be interested in hearing your interpretation of the strength of the data, You see I am actually vey active in trying to promote my ideas and have garnered the attention of Dr. Schmahmann of Harvard as well as doctors at Cambridge. I believe my routine (which is not my own making) can be effective for some (and I emphasize some) patients with neurological diagnoses in halting or slowing the progression. In short I personally am certain that someone who had a “smell” test done that came back positive would have a chance to alter the progression of their disease.
My approach stems from these 2 videos:
https://vimeo.com/191664871
The study behind the first video was this one:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4221920/
which I realize is not about PD, but I think the concept is equally applicable to a host of neurological disorders. To wit, studies to date have all been focused on one drug at a time, but these types of illnesses present with a myriad of interrelated problems so the probability of success was virtually zero. Treatments for these types of illnesses will require a multi-pronged approach (that is until we can modify genes and fix the root cause but that’s a whole other “ball of wax” )
In any case, this is dragging on a little too far so let me add a few brief facts:
1) I had many symptoms and they are all gone since beginning my routine.
2) I have convinced people around the world to try my routine and I have heard from nearly a dozen individuals that they too are experiencing an improvement in their condition.
3) Dr Mischley’s work and others seems to me clear proof that people with PD ARE today altering the progression of their disease.
Finally I’ll restate my routine and ask my question:
What are your thoughts on “Fixing the Holes in Your Roof” or stopping PD progression with a mixed therapy?
My routine:
1) exercise at 80% max heart rate 4-5 days per week plus weight training of all major muscle groups
2) a mostly vegetarian diet rich in cruciferous vegetables which avoids processed food, dairy, and meat
3) supplements including 40 g trehalose, 500 mg niagen twice daily, 50 mg pterostilbene twice daily, 2000 IU vitamin D
4) yoga 3 times a week
(note: I have also been taking trehalose intra-nasally now for about 3 months – I make a 4:1 solution using pharmacy grade trehalose and distilled water every two weeks and spray my nose 3 times a day – all under the careful watch of my GP)
Your avid reader in NY,
Joe Peck
LikeLike
Hi Joe,
Thanks for your very interesting comment – glad you liked the post.
For the sake of stimulating constructive discussion here, I’m going to do my devil’s advocate routine regarding some of the things you wrote:
When you say “I had many symptoms and they are all gone”, what exactly are you measuring? Do you mean tremor? Or stiffness? Or GI issues? And more importantly, HOW are you measuring/assessing these symptoms? Is your physician involved in that process? Is there a set of UPDRS scores that could be compared?
I ask this because there has recently been a lot of discussion both here and elsewhere on the web regarding the monitoring and assessment of PD symptoms. And this idea also applies to your trehalose and pterostilbene treatment regime – how are you measuring their efficacy? (And how did you determine dose?) Again, I am genuinely curious and I think any improvements in our tool set with regards to monitoring and assessment of PD would be in everyone’s best interest.
Thanks again for sharing – I look forward to your answers.
Kind regards,
Simon
LikeLike
Simon, I am glad to have your “Devil’s Advocate” questions as they will help in my process of improving my argument so I can garner the attention of serious researchers like yourself. First, I’m not sure if you were able to find my early post, but I need to explain that I am not suffering from PD but rather SCA1. I came to your site because the issues involved with PD are similar to polyQ disorders like mine.
Symptoms and measuring: yes I had an initial neurologist that gave me a SARA test and I scored on the outside limit of the test so a mere tenth of an improvement in score is not significant, BUT my father is rather advanced and over a 6 month period his SARA score remained the same at a point in his illness where he should have been declining rapidly. Tragically we have had to place him in a nursing home where he is no longer allowed to take niagen and pterostilbene and trehalose and his condition has immediately worsened.
Physician: Yes. My GP and multiple neurologists are now following my family including the aforementioned Dr. Schmahmann of Harvard.
How to measure efficacy: In my family’s case it is a simple function of keeping track of SARA scores. However, for myself, I am now totally symptom free. I have a CAG count of 42. I am well past the age at which I should have symptoms for SCA1. How long I can continue symptom free is my whole point. I am a smart patient. I graduated Magna Cume Laude from Dartmouth College with an MBA/BE in 5 years and was my high school valedictorian. I am going to research an answer to my own problem, BUT honestly I know my own body and KNOW I have a solution that can help people who are in a similar condition of having a genetic diagnosis of a neurological disorder, but are at the moment symptom free. I am not rich or famous, and I am running into incredible brick walls in terms of convincing doctors and researchers that there is a “cure” for pre-symptomatic patients with neurological disorders of late onset. I do not claim to have new insight; I am merely using data that has already been presented and compiling it into a usable form.
Determining dose: This is the hardest element. Right now I have myself and 9 people worldwide that are following my advice and seeing benefit. In that group we are sharing physical reactions and attempting to hone in on safe but effective dosages. The starting point is always whatever human studies are available. Fortunately there is at least one study for each of the supplements I am taking which gave me a “safe” starting point. In the end though it has come down to personal experimentation in trying to figure out an optimum dosage. The issue becomes incredibly complex as the heart of this solution is a combined therapy so one can never be certain of which element is changing which outcome.
Right now all I can say for certain is that I am 51 with a CAG count of 42 and a diagnosis of SCA1 and I should be feeling something, but I do not, BUT I did, and all I want is to convince scientists to explore this area of a multiple mode approach because I know it can help some.
Obviously as a patient I am heavily biased, but I thank you again and again for creating this website as the information you provide here is invaluable and truly helps to empower patients. I could go on for hours writing my thoughts, but I will stop here.
Here is my email: josephpeck1966@gmail.com. I hope I can provide some small amount of data in support of my opinion.
Many Thanks!
Joe
LikeLike