
|
# # # # In April of this year it was announced that the closely watched Phase II PASADENA clinical trial had not to met its primary objective. This was a large clinical evaluation of an immunotherapy approach (called prasinezumab) for disease modification in Parkinson’s. At the time of the announcement, it was indicated that the researchers who conducted the study had seen “signals of efficacy” in the data. This week the results of the study were presented at an international conference and it was reported that prasinezumab “significantly reduced decline in motor function by 35% (pooled dose levels) vs. placebo after one year of treatment“. In today’s post, we will discuss what the PASADENA study was, review the results that have been released, and discuss what might happen next. # # # # |

At 7am (just prior to the opening of the Swiss Stock Exchange) on Wednesday 22nd April 2020, the pharmaceutical company Roche published its sales results for the 1st Quarter. The financial report looked good, particularly considering the current COVID-19 economic climate, but there was one sentence on page 133 of the results (highlighted below) that grabbed a lot of attention:
 From page 133. Source: Roche
From page 133. Source: Roche
For those of you (like myself) who struggle with fine print, the sentence reads:
“Study did not meet its primary objective, but showed signals of efficacy“
This was how the Parkinson’s community found out about the top line result of the closely followed Phase II PASADENA study evaluating the immunotherapy treatment prasinezumab in individuals recently diagnosed with Parkinson’s.
Many within the Parkinson’s community were basically:
 Yet another negative clinical trial result.
Yet another negative clinical trial result.
But then, later that same day, the biotech firm Prothena – which developed prasinezumab and is partnered with Roche in the clinical testing – kindly provided a press release.
 And in that document, the company repeated that prasinezumab “showed signals of efficacy” , but importantly: “These signals were observed on multiple prespecified secondary and exploratory clinical endpoints“.
And in that document, the company repeated that prasinezumab “showed signals of efficacy” , but importantly: “These signals were observed on multiple prespecified secondary and exploratory clinical endpoints“.
And then the Parkinson’s community was like:
 This week we found out more about those “signals of efficacy” and the results of the PASADENA study, and they look interesting.
This week we found out more about those “signals of efficacy” and the results of the PASADENA study, and they look interesting.
What do the results show?
The PASADENA study is an ongoing Phase II clinical trial of the alpha synuclein-targeting immunotherapy treatment prasinezumab (the study is listed on the Clinicaltrials.gov as NCT03100149). For those readers unfamiliar with immunotherapy, prasinezumab and the PASADENA study – click here to read a previous SoPD post on this topic.
The study involves three parts (it used to be 2, but encouragingly it is now 3 parts):
Part 1 is a randomised, double-blind, placebo-controlled study involving approximately 300 people with Parkinson’s (all less than 2 years since diagnosis) to evaluate the efficacy and safety of prasinezumab/PRX002 in people with Parkinson’s over 52 weeks. Participants were randomly assigned to one of three groups (low dose/1500 mg or high dose/4500 mg of prasinezumab/PRX002, or placebo treatment). The treatments was administered (via intravenous infusion) once every 4 weeks.
Part 1 of the study is completed and the announcement made this week is associated with this part of the trial.
Part 2 of the PASADENA study is a 52-week blinded extension phase in which participants from the placebo group of the study will be re-randomly assigned into one of two doses of prasinezumab on a 1:1 basis. This means that all participants will be on active treatment (prasinezumab). Participants who were originally assigned to an active dose continue at that same dose level for the additional 52 weeks.
Part 2 of the study is still ongoing. The results that have been presented to date are from Part 1 of the study.
The recently added Part 3 of the study will be an extension of Part 2 for potentially up to 5 years (Click here to read more about the details of the study).
What do the Part 1 results suggest?
As the April release reported, the results of Part 1 of the PASADENA study found that 52 weeks of prasinezumab treatment in Parkinson’s did not meet the primary endpoint of the study.
What does primary endpoint mean?
The primary endpoint of a clinical study is a pre-determined measure of whether the agent has an effect in slowing Parkinson’s progression).
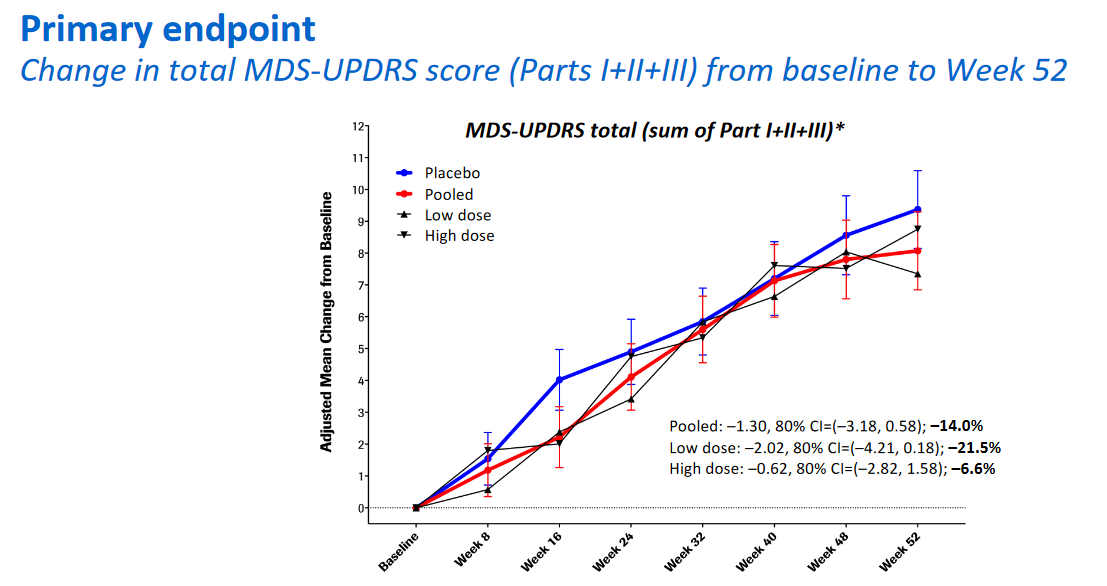
The primary end point for Part 1 of the PASADENA study was “a difference in the Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) total score (Parts I, II and III) between treatment and control groups”. Important to understand that the primary end point here was a combination of Parts I, II and III of the MDS-UPDRS.
And as you can see from the graph presented below, the blue line of the placebo group travels along basically the same trajectory as both of the treatment groups. The trajectory is an increasing change in MDS-UPDRS score (left hand axis) over time (line the bottom axis), suggesting progression of overall Parkinson’s features:
 Source: Prothena
Source: Prothena
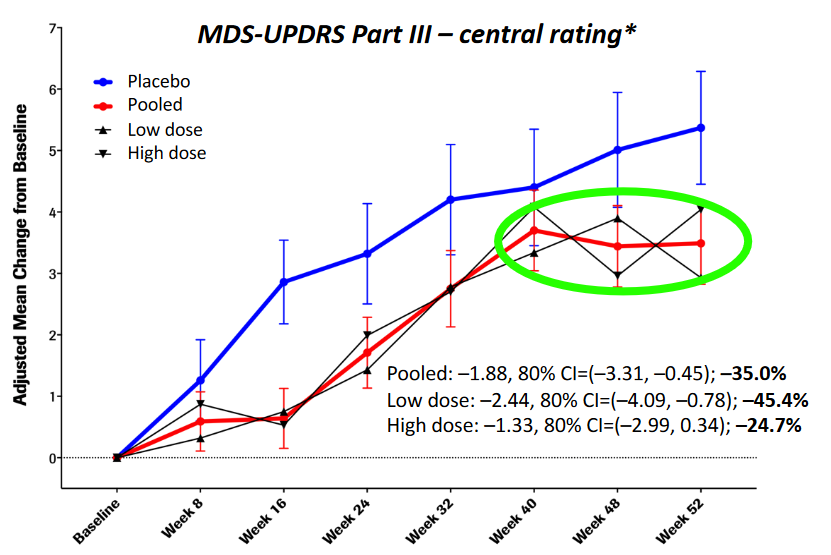
But (and it’s a big BUT), when the researchers broke the data down into individual components of the MDS-UPDRS and they looked at just Part III of the the MDS-UPDRS, they noticed both of the prasinezumab treated groups performed better that the placebo group.
Wait. What is part III of the MDS-UPDRS?
Part III is the clinician-based rating scores of the motor features of Parkinson’s.
It has 33 items (in effect there is only 18 items, but several address which side of the body, or which limb is affected) that a clinician will assess and score.
And when the researchers looked at just the Part III results, this is what they found:
 Source: Prothena
Source: Prothena
If you look at the blue line in the graph above, you will see that it is on a steeper trajectory than the black lines of the prasinezumab treated groups. And it is well above the red line, which represents the pooled data of both prasinezumab treated groups.
There are two potentially interesting phases in this data: first, the initial separation of the lines (between baseline and week 24), and then the second phase between week 40 and 52 where the prasinezumab treated groups appear to plateau (highlighted by the green oval).
The first phase begs the question: did the treatment have an immediate effect (Possibly peripheral? Maybe a reduction in inflammation?), and then the second phase prompts the obvious question can this apparent plateauing be maintained over time?
It will be interesting to see what happens in Part 2 of the PASADENA study, where everyone will be on the prasinezumab treatment. Will the part 1 placebo participants display similar patterns of responses as they shift to the prasinezumab treatment? And will participants who were on prasinezumab treatment during Part 1 continue to plateau during Part 2?
Interesting. Is this all that was reported?
No. There are other pieces of encouraging data presented in the PASADENA Part 1 results.
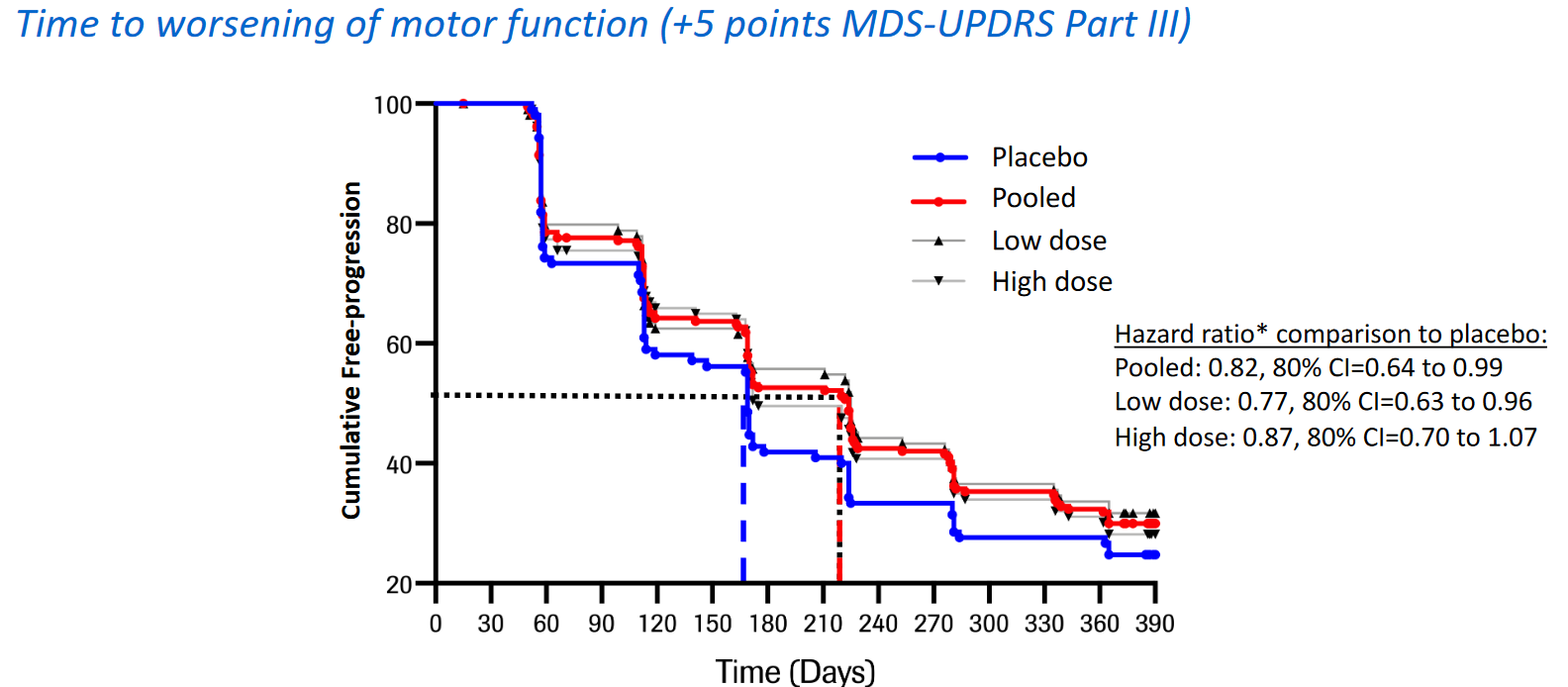
For example, the researchers also looked at the time to worsening of motor function. That is to say, how long did it take each participant to reach +5 points extra on their MDS-UPDRS Part III score. And here they found that the placebo treated group reached this mark sooner (50% of them at ~160 days) than the prasinezumab treated groups (at ~220 days). See the blue line (placebo-treated group) in the graph below is lower than the combined prasinezumab treated groups (red line), indicating more rapid progression in terms of motor features in the placebo group (compared to the prasinezumab treated groups):
 Source: Prothena
Source: Prothena
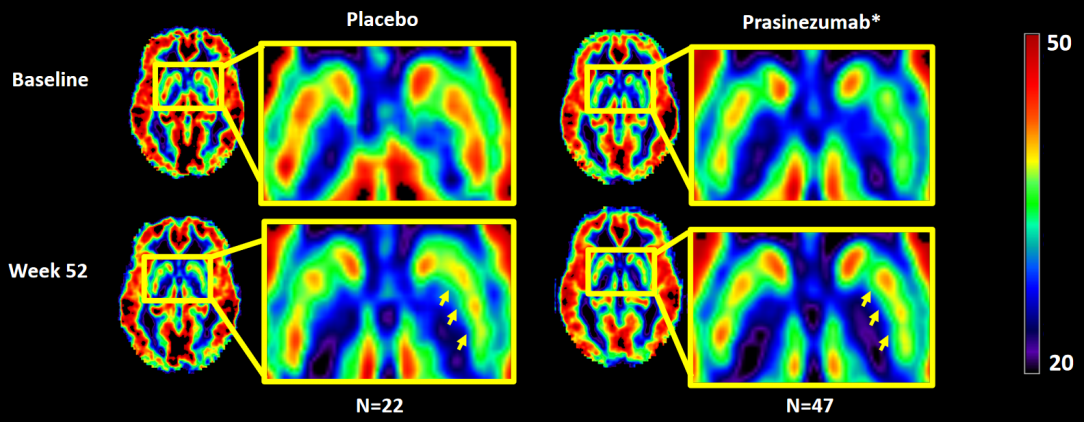
And there was another interesting difference in the data: The researchers used brain imaging to assess changes in cerebral blood flow in different brain regions in 69 participants (22 in the placebo group and 47 in the prasinezumab treated groups). They found that the prasinezumab treated groups exhibited a reduction in decline in cerebral blood flow in a region of the brain called the putamen, which is badly affected in Parkinson’s.
In the image below you have bird’s eye views of the brains of an individual treated with placebo treatment (left) and another treated with prasinezumab (right). The top row of images is from baseline measures (before treatment began), and the bottom row of images were taken after 52 weeks of treatment. Red indicates high levels of blood flow and the squared areas are where the putamen is in the brain – it lies on both sides of the brain). You will hopefully see that the difference between the top and bottom image is greater for the left hand side images (placebo) than the right hand side images (prasinezumab-treated), indicating a bigger reduction in cerebral blood flow to the putamen in the placebo group (compared to the prasinezumab treated groups):
 Less red in the placebo group. Source: Prothena
Less red in the placebo group. Source: Prothena
This difference is another bit of data suggesting that the prasinezumab-treated group had a reduction in the progression of certain aspects of their Parkinson’s.
What do you mean “certain aspects of their Parkinson’s”?
Well, the researchers did say that prasinezumab did not show any effect on:
- DaT-SPECT brain imaging (a measure of dopamine activity in the putamen)
- MDS-UPDRS Part I (non-motor experiences of daily living)
- MDS-UPDRS Part II (motor experiences of daily living)
- SE-ADL (Schwab and England Activities of Daily Living) Scale
In addition, all of the participants in the PASADENA trial were recently diagnosed cases of Parkinson’s, and they were not on any PD medication (such as L-dopa) at the start of the trial. Being on PD medication was actually an exclusionary factor for being enrolled in the study. The investigators kept track of when all of the participants finally initiated PD medication and there was no difference between the prasinezumab treated groups and the placebo-treated group with regards to initiating PD medication.
So as with the 2017 exenatide results (Click here to read a previous SoPD post about this), there are hints of something interesting potentially happening here, but it requires further investigations.
And luckily, further investigations are currently ongoing. As we mentioned above, these results are only from Part I of the PASADENA study. Part II (where everyone participating in the study is put on prasinezumab and followed for another 52 weeks) is ongoing. We will hopefully learn more about those results next year.
What is going to happen next with prasinezumab?
Roche and Prothena have concluded that their “findings support the potential of prasinezumab to slow underlying disease pathophysiology and clinical decline in patients with PD. Further investigations are warranted” (Source).
So hopefully we will learn soon about plans for some kind of follow up (maybe Phase III) trial.
So what does it all mean?
There is a furious debate in academic circles at the moment regarding immunotherapy targeting alpha synuclein in Parkinson’s. It is partly based on a mass grave yard of Phase 2 & 3 clinical trials in Alzheimer’s research. Dozens of immunotherapy approaches targeting the Alzheimer’s-associated proteins beta amyloid and Tau have failed to make a dent in the progression of dementia (except of course for Biogen’s aducanumab – click here to read more about that saga).
It is also based on theories that accumulation of alpha synuclein is resulting in a loss of function toxicity (the protein is no longer doing everything it should be doing, resulting in stress on the cell) rather than a gain of function toxicity (too much protein causing trouble).
As a result, a huge amount of attention has been focused on the PASADENA study as it is the first immunotherapy clinical trial to announce results in Parkinson’s. Another alpha synuclein-based immunotherapy trial being closely watched is the Biogen SPARK study (Click here to read a previous SoPD post about that study) as it too is in Phase II.
Whether the waring factions of academia are right or wrong will ultimately be decided by what happens in the clinical studies that are currently ongoing.
My guess is that they are both right (and wrong).
The results presented by Roche and Prothena this week are encouraging and deserve further analysis and discussion. I’ll let you know when we hear anything new.
ADDENDUM –20/10/2020: Today both Roche and Prothena announced that they will be advancing their alpha synuclein immunotherapy agent Prasinezumab into a Phase 2b study in individuals with early Parkinson’s, starting early 2021.

All of the material on this website is licensed under a
Creative Commons Attribution 4.0 International License
You can do whatever you like with it!
EDITOR’S NOTE: The information provided by the SoPD website is for information and educational purposes only. Under no circumstances should it ever be considered medical or actionable advice. It is provided by research scientists, not medical practitioners. Any actions taken – based on what has been read on the website – are the sole responsibility of the reader. Any actions being contemplated by readers should firstly be discussed with a qualified healthcare professional who is aware of your medical history. While some of the information discussed in this post may cause concern, please speak with your medical physician before attempting any change in an existing treatment regime.
Some of the companies mentioned in this post are publicly traded companies. That said, the material presented on this page should under no circumstances be considered financial advice. Any actions taken by the reader based on reading this material is the sole responsibility of the reader. None of the companies have requested that this material be produced, nor has the author had any contact with the companies beyond speaking with researcher employees about study data. This post has been produced for educational purposes only.
The banner for today’s post was sourced from Roche

Thanks for the details on this Simon. Very interesting indeed. So if the total UPDRS is not different between placebo and treated groups, but part III was significant, does this imply that parts I, II and IV actually got worse in the treated groups? Or is the Part III result too diluted to show significant change?
Also, it appears the baseline of the treated group started off with significantly lower blood flow than the placebo group. And the treated group appears to have had an increase of blood flow to the Putamen over the 52-week period. With 316 people enrolled in the trial, why do the FMRI results only compare 69 participants ? Are the graphics ‘merged’ to show an average response among brains? What difference does blood flow really make if the DaT scans are undifferentiated? Could it signal the treated group was ‘trying’ harder, but with a worse initial baseline than the placebo group, wasn’t going anywhere?
Finally, there’s also the observation that the results don’t appear to be dose dependent.
So, while interesting, it isn’t clear that it constitutes a breakthrough yet.
Fingers crossed for results from the second year of phase II, and continued retardation of progression in phase III.
Thanks again,
Tom
LikeLike
Hi Tom,
Thanks for your really interesting comment.
The difference in the absense of UPDRS Parts I & II is an intriguing aspect of the results, but I don’t think we should assume anything about the unpresented data. Part I & II are patient-based measures of non-motor and motor experiences of daily living (respectively) and can reflect tolerability issues of the treatment. The safety data, however, suggests no difference between the 3 treatment groups in terms of adverse events so this seems unlikely.
The blood flow data presented here is just two cases (prasinezumab-treated & control), so I would not read too much into that either. We’ll have to wait for the full results to be published before we will get a clearer idea of what the group baseline data looked like. I am not sure about the small number of participants involved in the imaging component. I am assuming that this was a cost issue (imaging is very expensive and large trials regularly only do imaging at one trial site – the imaging substudy for the exenatide Phase III is an example of this).
The difference between the DATscan and FMRI data is interesting. I am really not sure how to interpret it. But I agree with you that this is not necessarily “a breakthrough”, but it is encouraging. I would like to see a deeper dive into the results, particularly the blood and cerebrospinal fluid work (I am curious about inflammatory markers). All of that is still to come though.
Kind regards,
Simon
LikeLike
Hi Simon,
What do you make of some of the stats used to get some of the figures listed above? Particularly the P < 0.2?
LikeLike
Hi Ben,
It’s a great question. I have asked the study coordinators about this and they have said that the study was designed with 80% confidence intervals in order to have a relatively small sample size (otherwise the number of participants required would have been much larger).
We have to remember that this was a Phase II trial and (despite the stated primary endpoint) the investigators were firstly evaluating long term safety/tolerability, and second, looking for signals of efficacy. The stricter test of whether the treatment is working is left to larger Phase III studies.
Kind regards,
Simon
LikeLike
Always enlightening Simon.
It was also interesting to see the bradykinesia curves diverge on the smartphone app starting from t=0. Unfortunately the active group didn’t plateau like the part III scores, but it’s not clear what the scale is.
I believe the phone tracks relative slowing of finger tap and wrist turn rates during the timed test, not absolute rate or total taps (along with a bunch of other stuff) but the data shows two lines with nonspecific units that diverge. Once again a plot that can’t directly be tracked back to the metric system. (Let’s label those axes and share the data pleas?) Better than the Uncorrelated Parkinson’s Disease Rating Scale however.
On that note: I loved this presentation from Affiris.
Especially slides 8 and 9.
At some point Simon, if you’re taking requests, I’d love to hear more about whether an antibody can trigger the immune system to clear a protein from inside/on a cell or just from the surrounding goop. Seems like you really want to target both if you want to fully inhibit cell to cell spreading assuming the whole “prion like toxic protein” theory is right.
LikeLike
I was also concerned at the lack of dosage-related response. . In addition, as we all know, retrospective analyses which have not been built into the protocol beforehand should always be looked at with great skepticism. But if an anti-synuclein antibody fails to work, does it deep six the whole hypothesis or is it not penetrating into the neurons? I have more confidence in small molecular weight chemicals which could interfere with the amyloid-like misfolding of alpha synuclein
LikeLike